You might also like
- PHCP312 SyllabusDocument9 pagesPHCP312 SyllabusDanica PamintuanNo ratings yet
- Stanford Hospital & Clinics Antimicrobial Dosing Reference Guide 2013Document3 pagesStanford Hospital & Clinics Antimicrobial Dosing Reference Guide 2013SANCHOSKYNo ratings yet
- Grays Anatomy For Students 5th Edition 2023Document16 pagesGrays Anatomy For Students 5th Edition 2023AnandSreeNo ratings yet
- Menigitis & EncephalitisDocument38 pagesMenigitis & EncephalitisKim GonzalesNo ratings yet
- Nclex PointersDocument4 pagesNclex PointersCarl Michael de Guzman75% (12)
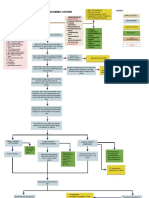
- Acute Ischemic Stroke Concept MapDocument6 pagesAcute Ischemic Stroke Concept MapMoonyeen Jann Casera Balic100% (2)
- Dr. Lola Susianti, Sppd-FinasimDocument28 pagesDr. Lola Susianti, Sppd-Finasimfahmy_tampanNo ratings yet
- Farmakologi Obat Analgesik, Anti Piretik & Anti Inflamasi: Andri Tilaqza, M.Farm., AptDocument45 pagesFarmakologi Obat Analgesik, Anti Piretik & Anti Inflamasi: Andri Tilaqza, M.Farm., AptDark BlueNo ratings yet
- NyeriDocument33 pagesNyeriAndriHernadiNo ratings yet
- Basic Rheumatology: 1. Inflammation 2. Pain Mechanism and Rheumatic Pain 3. Bone Metabolism and OsteoporosisDocument78 pagesBasic Rheumatology: 1. Inflammation 2. Pain Mechanism and Rheumatic Pain 3. Bone Metabolism and OsteoporosisTutde SedanaNo ratings yet
- Nonsteroidal Antiinflammatory Drugs and Antipyretic-AnalgesicsDocument60 pagesNonsteroidal Antiinflammatory Drugs and Antipyretic-AnalgesicsCHANG ZHI NING / UPMNo ratings yet
- 2 NSAIDsDocument12 pages2 NSAIDsأحہمہد بہنہ قہمہوNo ratings yet
- PharmarespiDocument19 pagesPharmarespiMark Lorenz NaldozaNo ratings yet
- Topic 2. Pharmacology For Pain and Inflammation RDocument52 pagesTopic 2. Pharmacology For Pain and Inflammation RKendrick GalosoNo ratings yet
- 2021 Update Management Pain (Dokter & Medical)Document30 pages2021 Update Management Pain (Dokter & Medical)Andri MuliaNo ratings yet
- PHARMA-R1.1-NSAIDs, DMARDs, Non-Opioid Analgesics and Drugs Used in GoutDocument11 pagesPHARMA-R1.1-NSAIDs, DMARDs, Non-Opioid Analgesics and Drugs Used in Goutcharmainemargaret.parreno.medNo ratings yet
- Vioxx COX2i Workshop CB 2020Document34 pagesVioxx COX2i Workshop CB 2020Castobary MunishiNo ratings yet
- Emd166 Slide Acute Coronary PDFDocument40 pagesEmd166 Slide Acute Coronary PDFlorinsyacderminnatNo ratings yet
- Dr. Marcelia Suryatenggara, Sp. S - How To Choose Your AnalgeticsDocument9 pagesDr. Marcelia Suryatenggara, Sp. S - How To Choose Your AnalgeticsFreade AkbarNo ratings yet
- Analgesicos No Opiodes No Esteroideos y Cox SelectivosDocument14 pagesAnalgesicos No Opiodes No Esteroideos y Cox SelectivosXY PragmaNo ratings yet
- Reuben Drug Classes and Actions NsaidsDocument2 pagesReuben Drug Classes and Actions NsaidsKarinaKarinaNo ratings yet
- Group 3 AntiinflammatoryDocument83 pagesGroup 3 AntiinflammatoryJesseleAikaAraisNo ratings yet
- Cox-1 and Cox-2 Inhibitor For Treatment Acute Chronic Pain, What's The Difference?Document57 pagesCox-1 and Cox-2 Inhibitor For Treatment Acute Chronic Pain, What's The Difference?EmranNo ratings yet
- 184 Up Ains CS-1Document99 pages184 Up Ains CS-1Devi ShilviaNo ratings yet
- Manajemen Nyeri Dengan DexketoprofenDocument27 pagesManajemen Nyeri Dengan Dexketoprofenmaya santiNo ratings yet
- Analgesic Antiinflammation: Pharmacology Lab. of FKUBDocument11 pagesAnalgesic Antiinflammation: Pharmacology Lab. of FKUBHanny Prasetiana YuriantiNo ratings yet
- Gangguan Kel. AdrenalDocument16 pagesGangguan Kel. AdrenalInna Nur Fitri DahliyantiNo ratings yet
- 1 - NSAIDsDocument13 pages1 - NSAIDscontactaraizhussainNo ratings yet
- Reuben - Drug Classes and Actions NsaidsDocument2 pagesReuben - Drug Classes and Actions NsaidsTricia Kaye IblanNo ratings yet
- F.R 1.3 Farmakologi Obat Antipiretik Dan Induksi DemamDocument64 pagesF.R 1.3 Farmakologi Obat Antipiretik Dan Induksi Demamasa0411 behiraNo ratings yet
- Final CPD PAIN MANAGEMENT LECTURE Edit 2Document57 pagesFinal CPD PAIN MANAGEMENT LECTURE Edit 2auliaNo ratings yet
- 1 - AINS Interaction PotenciesDocument9 pages1 - AINS Interaction PotenciesTitian DiasNo ratings yet
- Anti-Inflammatory DrugsDocument36 pagesAnti-Inflammatory Drugsnezifzenu2023No ratings yet
- 5 - PAH Management 4Document34 pages5 - PAH Management 4puskommedic 003No ratings yet
- Nem-Szteroid Gyulladásgátlók (Nsaids) : 1. Gyulladásgátlás 2. Fájdalomcsillapítás 3. LázcsillapításDocument34 pagesNem-Szteroid Gyulladásgátlók (Nsaids) : 1. Gyulladásgátlás 2. Fájdalomcsillapítás 3. LázcsillapításSoodn Kang SoodnNo ratings yet
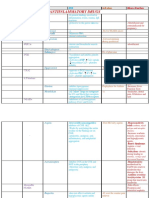
- Drug Sheet 2Document88 pagesDrug Sheet 2Umbe ChinakaNo ratings yet
- Articulo 1 Patogeneral SrisDocument21 pagesArticulo 1 Patogeneral SrisFabiola GuevaraNo ratings yet
- 3 - Vascular Endothelium IMBS 2023Document18 pages3 - Vascular Endothelium IMBS 2023Francisco HenriquezNo ratings yet
- Pharma Topic 2 NotesDocument8 pagesPharma Topic 2 NotesAshley Franceska CansanayNo ratings yet
- L9 Inflammation (NSAIDs)Document25 pagesL9 Inflammation (NSAIDs)SaadNo ratings yet
- Farmakologi Blok Muskuloskeletal - AnalgetikDocument49 pagesFarmakologi Blok Muskuloskeletal - AnalgetikFaridNo ratings yet
- Year Ii Pharmacology Drugs ListDocument21 pagesYear Ii Pharmacology Drugs ListsaifuddinNo ratings yet
- Nama Riwayat PekerjaanDocument35 pagesNama Riwayat PekerjaanfgrehNo ratings yet
- NsaidsDocument16 pagesNsaidsraffia mahakNo ratings yet
- Drug Study: Patient Name: SSG. Tungson, Christian 34 Y/oDocument11 pagesDrug Study: Patient Name: SSG. Tungson, Christian 34 Y/oNelle ReyNo ratings yet
- Chapter 18Document5 pagesChapter 18Jessie Marie DuhaylungsodNo ratings yet
- Pharmacology of P-A Mediators Lecture Notes 12-13Document20 pagesPharmacology of P-A Mediators Lecture Notes 12-13Fikadu GidiNo ratings yet
- Adrenal Control Within The Body: Presented byDocument20 pagesAdrenal Control Within The Body: Presented byhumnaNo ratings yet
- Comparison of Cyclooxygenase (Cox-1 and Cox-2) EnzymesDocument11 pagesComparison of Cyclooxygenase (Cox-1 and Cox-2) EnzymesCyberLifeNo ratings yet
- Endocrine Functions of The Heart From Bench To BedsideDocument13 pagesEndocrine Functions of The Heart From Bench To Bedsidejtrujillo70No ratings yet
- Pain Management AulDocument23 pagesPain Management AulauliaulfaNo ratings yet
- Anti-Inflammatory Drugs Lec1 &2Document31 pagesAnti-Inflammatory Drugs Lec1 &2s.nilormee1201No ratings yet
- Chapter 7 - Analgesics For Treatment of Acute O - 2008 - Clinical Ocular PharmacDocument15 pagesChapter 7 - Analgesics For Treatment of Acute O - 2008 - Clinical Ocular PharmacsNo ratings yet
- L P 3 Analgesics FinalDocument24 pagesL P 3 Analgesics FinalZakria Al-HadadNo ratings yet
- Curriculum Vitae: Nama: Natsir Akil Riwayat PendidikanDocument50 pagesCurriculum Vitae: Nama: Natsir Akil Riwayat PendidikanSelica ErlindiNo ratings yet
- Update On The Clinical Pharmacology of Etoricoxib A Potent Cyclooxygenase2 InhibitorDocument21 pagesUpdate On The Clinical Pharmacology of Etoricoxib A Potent Cyclooxygenase2 InhibitorAnh Quoc LeNo ratings yet
- Gould: Chpt. 2, Porth: Chpt. 18: Figure 22.3 MariebDocument8 pagesGould: Chpt. 2, Porth: Chpt. 18: Figure 22.3 MariebLinda NguyenNo ratings yet
- ProstaglandinsDocument6 pagesProstaglandinsHassan KamalNo ratings yet
- Nonsteroidal Antiinflammatory DrugsDocument12 pagesNonsteroidal Antiinflammatory DrugsAlano S. LimgasNo ratings yet
- Rheumatic Heart DiseaseDocument15 pagesRheumatic Heart DiseaseAica AnisNo ratings yet
- Nsaid (: Non Steroid Anti Inflammation Drugs) & Gout TherapyDocument46 pagesNsaid (: Non Steroid Anti Inflammation Drugs) & Gout TherapyTutde SedanaNo ratings yet
- Aldosterone: International Series of Monographs in Pure and Applied BiologyFrom EverandAldosterone: International Series of Monographs in Pure and Applied BiologyNo ratings yet
- Lipid MediatorsFrom EverandLipid MediatorsFiona M. CunninghamNo ratings yet
- A Comparative Study OF NIHSS Between Ischemic Stroke Patients With and Without Risk FactorsDocument4 pagesA Comparative Study OF NIHSS Between Ischemic Stroke Patients With and Without Risk FactorsKlinik HanisNo ratings yet
- Copd - NCPDocument6 pagesCopd - NCPMonique Sacherow BacherNo ratings yet
- Ajr 163 3 8079866-1Document12 pagesAjr 163 3 8079866-1Damara Marell FerdyansyahNo ratings yet
- 5f40e819948bc198-209-GP-Epidemiological-S Srujana Reddy-5971861561Document12 pages5f40e819948bc198-209-GP-Epidemiological-S Srujana Reddy-5971861561MOHAMMED KHAYYUMNo ratings yet
- Generic NameDocument7 pagesGeneric NameGia Bautista-AmbasingNo ratings yet
- Selected Anomalies and Diseases of The Eye: Compiled by Virginia E. Bishop, Ph.D. 1986Document57 pagesSelected Anomalies and Diseases of The Eye: Compiled by Virginia E. Bishop, Ph.D. 1986Matthew MckenzieNo ratings yet
- Spondylosis Information LeafletDocument3 pagesSpondylosis Information LeafletAnis Azizah MogilNo ratings yet
- Thesis AdhdDocument6 pagesThesis Adhdfjmav19f100% (1)
- Disseminated Intravascular Coagulation by Group2Document33 pagesDisseminated Intravascular Coagulation by Group2Aji Cruz-MataNo ratings yet
- Rsik of ICH in Anticoagulation Primary Brain Tumor PatientDocument7 pagesRsik of ICH in Anticoagulation Primary Brain Tumor PatientFithry RahmaNo ratings yet
- 96-Article Text-328-1-10-20211022Document7 pages96-Article Text-328-1-10-20211022Asaad AlnhayerNo ratings yet
- Apathy Associated With Antidepressant Drugs A Systematic ReviewDocument16 pagesApathy Associated With Antidepressant Drugs A Systematic ReviewJ MrNo ratings yet
- Acid/Base and ABG Interpretation Made SimpleDocument45 pagesAcid/Base and ABG Interpretation Made SimpleekadtorNo ratings yet
- Association of Loneliness With Suicide Risk and Depression in Individuals With Schizophrenia: Moderating Effects of Self - Esteem and Perceived Support From Families and FriendsDocument7 pagesAssociation of Loneliness With Suicide Risk and Depression in Individuals With Schizophrenia: Moderating Effects of Self - Esteem and Perceived Support From Families and Friends簡千芮No ratings yet
- Mastering The Art of ArdsDocument69 pagesMastering The Art of ArdsRsc LmdNo ratings yet
- Module 10Document5 pagesModule 10Yuki Xairah TunayNo ratings yet
- National Filariasis Elimination ProgramDocument20 pagesNational Filariasis Elimination ProgramNaomi Cyden YapNo ratings yet
- Dokumen - Tips Loa LoaDocument28 pagesDokumen - Tips Loa LoaSababil AliNo ratings yet
- Galea - Abdominal Pain in ChildhoodDocument30 pagesGalea - Abdominal Pain in Childhoodsanty anggroiniNo ratings yet
- Identification, Evaluation, and Management of Children With ASDDocument69 pagesIdentification, Evaluation, and Management of Children With ASDWing Sze FUNGNo ratings yet
- WEEK 6 PPT PainDocument22 pagesWEEK 6 PPT PainDanica FrancoNo ratings yet
- Felocell Felv Helps Prevent Disease Cause by Feline Leukemia Virus (Felv)Document1 pageFelocell Felv Helps Prevent Disease Cause by Feline Leukemia Virus (Felv)Reginaldo ParcianelloNo ratings yet
- Anorectal Malformations in A Tertiary Pediatric Surgery Center Fromromania 20 Years of Experience 1584 9341-12-2 3Document5 pagesAnorectal Malformations in A Tertiary Pediatric Surgery Center Fromromania 20 Years of Experience 1584 9341-12-2 3Jeff LapianNo ratings yet
- Tool Box Talk - Working in Hot WeatherDocument1 pageTool Box Talk - Working in Hot WeatherMobashir MahmoodNo ratings yet
- Prado, Catherine BSN IIB (Activity 1 Case Scenario)Document52 pagesPrado, Catherine BSN IIB (Activity 1 Case Scenario)Catherine PradoNo ratings yet
- Paper AnalysisDocument4 pagesPaper AnalysisLayali MassisNo ratings yet