You might also like
- Classification of AntidiureticsDocument7 pagesClassification of AntidiureticsJot grewal100% (1)
- Types of Skull FractureDocument5 pagesTypes of Skull FractureKhor Hui DiNo ratings yet
- Skull FractureDocument13 pagesSkull FractureEddie LimNo ratings yet
- Tumor OtakDocument17 pagesTumor Otakmona030988No ratings yet
- Basic Principles of Surgery: DEVELOPING A SURGICAL DIAGNOSIS: Important DecisionsDocument5 pagesBasic Principles of Surgery: DEVELOPING A SURGICAL DIAGNOSIS: Important DecisionsStudent FemNo ratings yet
- Neurological History ReviewDocument7 pagesNeurological History ReviewM NNo ratings yet
- Fracture 01Document42 pagesFracture 01api-19916399No ratings yet
- Complication of FractureDocument38 pagesComplication of FractureAshok BalwadaNo ratings yet
- Supracondylar FractureDocument53 pagesSupracondylar Fracturedesire kbpNo ratings yet
- Malunion Delayed Union and Nonunion FracturesDocument31 pagesMalunion Delayed Union and Nonunion FracturesRasjad ChairuddinNo ratings yet
- Cranial Nerves Examination GuideDocument14 pagesCranial Nerves Examination GuideMoussa FarhatNo ratings yet
- Clinical Pathology Case StudiesDocument10 pagesClinical Pathology Case StudiesKwadwo Sarpong JnrNo ratings yet
- N C C N D: Ursing ARE OF Lients With Eurologic IsordersDocument96 pagesN C C N D: Ursing ARE OF Lients With Eurologic IsordersMatt Lao DionelaNo ratings yet
- Introduction To FracturesDocument40 pagesIntroduction To FracturesAnisah Pangandag MapandiNo ratings yet
- SC - Fracture ZMHDocument51 pagesSC - Fracture ZMHMis StromNo ratings yet
- Neurologicdisorders 100816033614 Phpapp01 PDFDocument96 pagesNeurologicdisorders 100816033614 Phpapp01 PDFenam professorNo ratings yet
- Stroke Rsu Banjar: DR Fuad Hanif Sps M.KesDocument80 pagesStroke Rsu Banjar: DR Fuad Hanif Sps M.KesRobert HarrisNo ratings yet
- 3-Introduction To The Interviewing ProcessDocument23 pages3-Introduction To The Interviewing Processkashmala afzalNo ratings yet
- Pre Operative Planning For Total Hip ArthroplastyDocument78 pagesPre Operative Planning For Total Hip ArthroplastyJulio EspinozaNo ratings yet
- Neurology - : Approach To Headache DisordersDocument8 pagesNeurology - : Approach To Headache DisordersKarenNo ratings yet
- Orthopedic SlidesDocument78 pagesOrthopedic SlidesAzry Mustapa100% (1)
- Deep Vein ThrombosisDocument5 pagesDeep Vein ThrombosisnikaaraaaNo ratings yet
- Ocular InjuryDocument46 pagesOcular InjurysnyNo ratings yet
- Rheumatoid ArthritisDocument19 pagesRheumatoid ArthritisKim GonzalesNo ratings yet
- Osteoarthritis: T Person's of Developing Osteoarthritis. It IncludesDocument5 pagesOsteoarthritis: T Person's of Developing Osteoarthritis. It IncludesLove Shery SabrosoNo ratings yet
- Vertebrobasilar Insufficiency/Syndrome: Hitesh Rohit (3 Year BPT)Document14 pagesVertebrobasilar Insufficiency/Syndrome: Hitesh Rohit (3 Year BPT)Hitesh N RohitNo ratings yet
- Fractures of The Upper LimbDocument3 pagesFractures of The Upper LimbJim Jose AntonyNo ratings yet
- Spinal InjuriesDocument22 pagesSpinal InjuriesPak Budi warsonoNo ratings yet
- Operative Procedures: 1130 SRB's Manual of SurgeryDocument1 pageOperative Procedures: 1130 SRB's Manual of SurgerymadhuNo ratings yet
- Pelvic FracturesDocument8 pagesPelvic FracturesArif AbubakarNo ratings yet
- Fracture HealingDocument33 pagesFracture HealingAgnes RusliNo ratings yet
- Head Trauma Causes, Symptoms, Diagnosis and TreatmentDocument50 pagesHead Trauma Causes, Symptoms, Diagnosis and TreatmentNatasya Saraswati100% (1)
- What Is PolymyositisDocument24 pagesWhat Is PolymyositisAshraf MobyNo ratings yet
- Introduction To Trauma: LSU Medical Student Clerkship, New Orleans, LADocument31 pagesIntroduction To Trauma: LSU Medical Student Clerkship, New Orleans, LAnandangNo ratings yet
- Classification of NeuropathyDocument16 pagesClassification of NeuropathysekiannNo ratings yet
- Motor Neuron Disease: Amyotrophic Lateral Sclerosis (ALS)Document2 pagesMotor Neuron Disease: Amyotrophic Lateral Sclerosis (ALS)james cordenNo ratings yet
- Chapter 257: Head Trauma: Introduction and EpidemiologyDocument35 pagesChapter 257: Head Trauma: Introduction and EpidemiologyIustitia Septuaginta SambenNo ratings yet
- Shingles Rash Caused by Varicella-Zoster VirusDocument16 pagesShingles Rash Caused by Varicella-Zoster VirusColleen De la RosaNo ratings yet
- Chest and Abdominal Injuries: Forensic Medicine by Yazan AbueidehDocument54 pagesChest and Abdominal Injuries: Forensic Medicine by Yazan AbueidehRayyan Alali100% (1)
- Motor Neuron DiseaseDocument4 pagesMotor Neuron Diseasem3d1kNo ratings yet
- Abdominal IncisionsDocument12 pagesAbdominal IncisionsHUZAIFA YAMAANNo ratings yet
- 328 Management of Polytrauma PatientDocument62 pages328 Management of Polytrauma PatientYanesh BishundatNo ratings yet
- STROKEDocument9 pagesSTROKEhillary elsaNo ratings yet
- Ortho - Surgery PDFDocument15 pagesOrtho - Surgery PDFIC BNo ratings yet
- Spinal Cord InjuryDocument17 pagesSpinal Cord InjuryMuhammad FaridNo ratings yet
- Subacute Combined Degeneration of Spinal CordDocument4 pagesSubacute Combined Degeneration of Spinal CordPriyanka MathurNo ratings yet
- General SurgeryDocument11 pagesGeneral Surgeryhuzaifa usmanNo ratings yet
- FractureDocument302 pagesFractureMaryjoy Gabriellee De La CruzNo ratings yet
- Cholinergic DrugsDocument15 pagesCholinergic DrugsChris Girgis100% (1)
- Hemorrhoid MedscapeDocument10 pagesHemorrhoid MedscapeRastho Mahotama100% (1)
- Optic Nerve Disease, Papillaedema Optic Atropy, Visual FieldDocument31 pagesOptic Nerve Disease, Papillaedema Optic Atropy, Visual FieldsamxtraNo ratings yet
- Management of Fracture of The Nasal BonesDocument53 pagesManagement of Fracture of The Nasal BonesMaikka IlaganNo ratings yet
- Fracture: Presented By: Ms. Durga Joshi M. SC NursingDocument63 pagesFracture: Presented By: Ms. Durga Joshi M. SC NursingSanjaya PutraNo ratings yet
- Supracondylar Humerus FractureDocument20 pagesSupracondylar Humerus FractureMusyawarah MelalaNo ratings yet
- Introduction to Intervertebral Disc Anatomy and PIVD ManagementDocument104 pagesIntroduction to Intervertebral Disc Anatomy and PIVD ManagementVivek SaxenaNo ratings yet
- Patient Data Report for Haemorrhoid CaseDocument3 pagesPatient Data Report for Haemorrhoid CaseBrother Vs CanonNo ratings yet
- Cerebrovascular AccidentDocument30 pagesCerebrovascular AccidentJaydee Dalay100% (2)
- Truncus ArteriosusDocument4 pagesTruncus ArteriosuskemalahmadNo ratings yet
- Head Injury Causes and TreatmentDocument47 pagesHead Injury Causes and TreatmentnikowareNo ratings yet
- Hand Out2007Document36 pagesHand Out2007Roza IsmarniNo ratings yet
- Why I Am Not A Primitivist - Jason McQuinnDocument9 pagesWhy I Am Not A Primitivist - Jason McQuinnfabio.coltroNo ratings yet
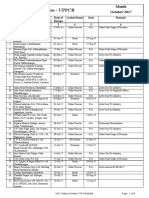
- NOC Status for UPPCB in October 2017Document6 pagesNOC Status for UPPCB in October 2017Jeevan jyoti vnsNo ratings yet
- Cooper Tire Warranty InformationDocument28 pagesCooper Tire Warranty InformationAbdulAziz AlGhamdiNo ratings yet
- Fuji Synapse PACS Quick GuideDocument1 pageFuji Synapse PACS Quick GuideM MNo ratings yet
- Process Safety Management System-PaperDocument11 pagesProcess Safety Management System-PaperV. Balasubramaniam100% (2)
- Internal Control QuestionnaireDocument19 pagesInternal Control QuestionnaireIchsanNo ratings yet
- Cot 1 Detailed Lesson Plan in Science 10Document3 pagesCot 1 Detailed Lesson Plan in Science 10Arlen FuentebellaNo ratings yet
- Medical Instrumentation Application and Design 4th Edition Webster Solutions ManualDocument13 pagesMedical Instrumentation Application and Design 4th Edition Webster Solutions ManualSaraRogersrbwgd100% (15)
- Public Health Risks of Inadequate Prison HealthcareDocument3 pagesPublic Health Risks of Inadequate Prison HealthcarerickahrensNo ratings yet
- India's Fertilizer IndustryDocument15 pagesIndia's Fertilizer Industrydevika20No ratings yet
- Macroeconomics: University of Economics Ho Chi Minh CityDocument193 pagesMacroeconomics: University of Economics Ho Chi Minh CityNguyễn Văn GiápNo ratings yet
- EngM6 TB WebDocument161 pagesEngM6 TB WebNong BillNo ratings yet
- Conference Flyer ChosenDocument4 pagesConference Flyer ChosenOluwatobi OgunfoworaNo ratings yet
- Cazul Cyril Burt 3Document3 pagesCazul Cyril Burt 3Cosmina MihaelaNo ratings yet
- 0000 0000 0335Document40 pages0000 0000 0335Hari SetiawanNo ratings yet
- Anatomija Za Umetnike PDFDocument4 pagesAnatomija Za Umetnike PDFДанило ВујачићNo ratings yet
- BTechSyllabus EC PDFDocument140 pagesBTechSyllabus EC PDFHHNo ratings yet
- Uss Port Royal (CG 73)Document9 pagesUss Port Royal (CG 73)samlagroneNo ratings yet
- Prueba Final Inglres Robert PalaciosDocument2 pagesPrueba Final Inglres Robert PalaciosCarlos GuerreroNo ratings yet
- Philo Q1module 4Document18 pagesPhilo Q1module 4Abygiel Salas100% (1)
- Bobcat Sambron Telescopics Handler Tec3070 3092 Spare Parts Catalog 63902 1Document15 pagesBobcat Sambron Telescopics Handler Tec3070 3092 Spare Parts Catalog 63902 1elijahmitchellmd220597jrpNo ratings yet
- Arlington Value's 2013 LetterDocument7 pagesArlington Value's 2013 LetterValueWalk100% (7)
- 40 Business Book SummariesDocument196 pages40 Business Book SummariesAnshuman SrivastavaNo ratings yet
- Health and Safety Plan TranslationDocument17 pagesHealth and Safety Plan TranslationEvaristo MudenderNo ratings yet
- Ruibal & Shoemaker 1984 - Osteoders in AnuransDocument17 pagesRuibal & Shoemaker 1984 - Osteoders in AnuransRuivo LucasNo ratings yet
- Electrode ChemDocument17 pagesElectrode Chemapi-372366467% (3)
- Sample Action Research in MathDocument12 pagesSample Action Research in MathKresta BenignoNo ratings yet
- Its Raining Idioms A Figurative Language ActivityDocument11 pagesIts Raining Idioms A Figurative Language ActivityTyrone MoogNo ratings yet
- Cook's Illustrated 090Document36 pagesCook's Illustrated 090vicky610100% (3)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (17)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (403)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Algorithms to Live By: The Computer Science of Human DecisionsFrom EverandAlgorithms to Live By: The Computer Science of Human DecisionsRating: 4.5 out of 5 stars4.5/5 (722)
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)