You might also like
- Strengthening Versus Stabilisation Exercise Programmes for Preventing and Reducing Low Back Pain in FemalesFrom EverandStrengthening Versus Stabilisation Exercise Programmes for Preventing and Reducing Low Back Pain in FemalesNo ratings yet
- Tdcs Inglês 1Document8 pagesTdcs Inglês 1Augusto ManoelNo ratings yet
- Children 08 01016Document20 pagesChildren 08 01016Ana paula CamargoNo ratings yet
- Disabilities 02 00026 v2Document14 pagesDisabilities 02 00026 v2Kaka Satria PratamaNo ratings yet
- ptrs009 01 08Document11 pagesptrs009 01 08mohamedsalahudeen193No ratings yet
- Studyprotocol Open Access: Lopes Et Al. Trials (2022) 23:87Document14 pagesStudyprotocol Open Access: Lopes Et Al. Trials (2022) 23:87Rogério MelaréNo ratings yet
- The Effects of Serial Casting On Lower Limb Function For Children With Cerebral Palsy: A Systematic Review With Meta-AnalysisDocument23 pagesThe Effects of Serial Casting On Lower Limb Function For Children With Cerebral Palsy: A Systematic Review With Meta-AnalysisDaniel MarvasoNo ratings yet
- Chronic HemiparesisDocument12 pagesChronic HemiparesisRon FranklinNo ratings yet
- An Intensive Virtual Reality Program Improves Functional Balance and Mobility of Adolescents With Cerebral PalsyDocument9 pagesAn Intensive Virtual Reality Program Improves Functional Balance and Mobility of Adolescents With Cerebral PalsyStephGrenNo ratings yet
- 1 s2.0 S1013702515000615 MainDocument9 pages1 s2.0 S1013702515000615 MainLalala Safitri2000No ratings yet
- MineDocument13 pagesMineZahra Faras SukmaNo ratings yet
- Pedia TriDocument6 pagesPedia TriRIZHAN ATHAYANo ratings yet
- JCM 11 05162 v2Document13 pagesJCM 11 05162 v2林良駿No ratings yet
- Investigeting The Effects of Standing Training On Body Functions and Activity For Nonambulatory Children With MyelomeningoceleDocument6 pagesInvestigeting The Effects of Standing Training On Body Functions and Activity For Nonambulatory Children With MyelomeningoceleMutiarahmiNo ratings yet
- Robot-Assisted Gait Training (Lokomat) Improves Walking Function and Activity in People With Spinal Cord Injury: A Systematic ReviewDocument13 pagesRobot-Assisted Gait Training (Lokomat) Improves Walking Function and Activity in People With Spinal Cord Injury: A Systematic ReviewSAMUEL ENRIQUE ASTUDILLO VARGASNo ratings yet
- Plyometric Training Effectiveness and Optimal.3Document11 pagesPlyometric Training Effectiveness and Optimal.3LeonardoValenzuelaNo ratings yet
- Medicina: Ffect of A Combined Stretching and StrengthDocument12 pagesMedicina: Ffect of A Combined Stretching and StrengthKimum KimúmNo ratings yet
- Kassim 2022Document12 pagesKassim 2022ع الNo ratings yet
- sergii,+Journal+editor,+03Hamed Articulo 2Document8 pagessergii,+Journal+editor,+03Hamed Articulo 2anye daniela gilNo ratings yet
- Interventions To Improve Gross Motor Performance in Children With Neurodevelopmental Disorders A Meta AnalysisDocument16 pagesInterventions To Improve Gross Motor Performance in Children With Neurodevelopmental Disorders A Meta AnalysissilNo ratings yet
- Effectiveness of Treadmill Training On Gait Function in Children With Cerebral Palsy: Meta-AnalysisDocument10 pagesEffectiveness of Treadmill Training On Gait Function in Children With Cerebral Palsy: Meta-AnalysisNovie AstiniNo ratings yet
- Studyprotocol Open AccessDocument19 pagesStudyprotocol Open AccessBryan Alexis Rodriguez CastroNo ratings yet
- 1 B 94Document16 pages1 B 94Auzia Tania UtamiNo ratings yet
- University of Essex School of Sport, Rehabilitation and Exercise Sciences SE720 Using Evidence in Healthcare Practice Assignment WorkbookDocument85 pagesUniversity of Essex School of Sport, Rehabilitation and Exercise Sciences SE720 Using Evidence in Healthcare Practice Assignment WorkbookShibli LondonNo ratings yet
- 2017 Article 457Document10 pages2017 Article 457JoeNo ratings yet
- Develop Med Child Neuro - 2020 - Ryan - Progressive Resistance Training For Adolescents With Cerebral Palsy The STARDocument12 pagesDevelop Med Child Neuro - 2020 - Ryan - Progressive Resistance Training For Adolescents With Cerebral Palsy The STARAkun NgasalNo ratings yet
- Aras Et Al. (2019)Document10 pagesAras Et Al. (2019)ع الNo ratings yet
- Effect of A Mixed Reality-Based Intervention On Arm, Hand, and Finger Function On Chronic StrokeDocument11 pagesEffect of A Mixed Reality-Based Intervention On Arm, Hand, and Finger Function On Chronic StrokeRosario Hentry kishoreNo ratings yet
- 12883_2024_Article_3614Document11 pages12883_2024_Article_3614lismuc.pa.21No ratings yet
- Effects of A Supported Speed Treadmill Training Exercise Program On Impairment and Function For Children With Cerebral PalsyDocument9 pagesEffects of A Supported Speed Treadmill Training Exercise Program On Impairment and Function For Children With Cerebral PalsyKimum KimúmNo ratings yet
- CCT - MeaningDocument10 pagesCCT - Meaningmandeep axonNo ratings yet
- Ijsr-1320 oDocument8 pagesIjsr-1320 oAzaelCarionNo ratings yet
- BMC PediatricsDocument11 pagesBMC PediatricsMica FrediNo ratings yet
- Regimen On Balance Impairment in Frail Effects of An Interactive Computer Game ExerciseDocument16 pagesRegimen On Balance Impairment in Frail Effects of An Interactive Computer Game ExerciseBruno FischerNo ratings yet
- Effects of Transcranial Direct Current Stimulat StudyDocument14 pagesEffects of Transcranial Direct Current Stimulat Studydinto dNo ratings yet
- FulltextDocument9 pagesFulltextVivek Edamuriyil RamesanNo ratings yet
- Kabat 4Document19 pagesKabat 4Nathalia Gutierrez RestrepoNo ratings yet
- A Backward Walking Training Program To ImproveDocument10 pagesA Backward Walking Training Program To ImproveRadhiatul AdillahNo ratings yet
- 1471 2377 12 129 PDFDocument8 pages1471 2377 12 129 PDFGita TikihaiNo ratings yet
- Effects of aerobic exercise using cycle ergometry on balance and functional capacity in post stroke patients a systematic review and meta analysisDocument8 pagesEffects of aerobic exercise using cycle ergometry on balance and functional capacity in post stroke patients a systematic review and meta analysisluigi.adacampoNo ratings yet
- Research Article Effect of Sports Nutrition Supplement On The Increase of Physical Strength Based On Mobile Sensor Network TechnologyDocument12 pagesResearch Article Effect of Sports Nutrition Supplement On The Increase of Physical Strength Based On Mobile Sensor Network Technologyarman jamshidiNo ratings yet
- McDonough2010 Article TheBack2ActivityTrialEducation PDFDocument8 pagesMcDonough2010 Article TheBack2ActivityTrialEducation PDFSandro PerilloNo ratings yet
- Int. Therapy Research DatoreDocument25 pagesInt. Therapy Research DatoreAll About Kids100% (1)
- Ijerph 18 10709Document13 pagesIjerph 18 10709Pablo Orellana StevensNo ratings yet
- Body-Weight-Supported Treadmill Training: Using Evidence To Guide Physical Therapy InterventionDocument5 pagesBody-Weight-Supported Treadmill Training: Using Evidence To Guide Physical Therapy InterventionSeries Tiếng Anh Song NgữNo ratings yet
- Whole-Body Intensive Rehabilitation PDFDocument9 pagesWhole-Body Intensive Rehabilitation PDFAlexandra NistorNo ratings yet
- Ffects of Neuromuscular Training On Motor: E Competence and Physical Performance in Young Female Volleyball PlayersDocument12 pagesFfects of Neuromuscular Training On Motor: E Competence and Physical Performance in Young Female Volleyball PlayersnurulaqilahizzatiNo ratings yet
- Journal of Neuroengineering and Rehabilitation: Biofeedback For Robotic Gait RehabilitationDocument11 pagesJournal of Neuroengineering and Rehabilitation: Biofeedback For Robotic Gait Rehabilitationnandhini raguNo ratings yet
- RevisionSistematicayMetaanalisis - TFNP.Stroke MariaJulianaGonzalezSilva ArticuloDocument18 pagesRevisionSistematicayMetaanalisis - TFNP.Stroke MariaJulianaGonzalezSilva Articulomariasol63No ratings yet
- 10.1186@s12984 019 0485 0Document9 pages10.1186@s12984 019 0485 0Angie VillafuerteNo ratings yet
- 55.literature Review About Neurodevelopmental Approaches-1Document37 pages55.literature Review About Neurodevelopmental Approaches-1Zeeshan AhmadNo ratings yet
- 2022 Article 16332Document11 pages2022 Article 16332ClaudiaNo ratings yet
- Strength Training for Adolescents With Cerebral Palsy (STAR)- Study Protocol of a Randomised Controlled Trial to Determine the Feasibility, Acceptability and Efficacy of Resistance Training for Adolescents With Cerebral PalsyDocument14 pagesStrength Training for Adolescents With Cerebral Palsy (STAR)- Study Protocol of a Randomised Controlled Trial to Determine the Feasibility, Acceptability and Efficacy of Resistance Training for Adolescents With Cerebral PalsyLeyla Valdebenito AlidNo ratings yet
- KinesiopaperDocument6 pagesKinesiopaperHermidaririn fisioNo ratings yet
- Kiper2015 Propio PDFDocument6 pagesKiper2015 Propio PDFJuan Pedro BarrientosNo ratings yet
- Acceptability of A Digital Health Intervention Alongside Physiotherapy To Support Patients Following Anterior Cruciate Ligament ReconstructionDocument11 pagesAcceptability of A Digital Health Intervention Alongside Physiotherapy To Support Patients Following Anterior Cruciate Ligament ReconstructionDianaNo ratings yet
- Journal Pone 0252193Document24 pagesJournal Pone 0252193SadoNo ratings yet
- Effect of Selective PercutaneouSDocument6 pagesEffect of Selective PercutaneouSMarcin ChłostaNo ratings yet
- 9 - TechnologicalAdvancements in CerebralPalsy RehabilitationDocument13 pages9 - TechnologicalAdvancements in CerebralPalsy RehabilitationMariaNo ratings yet
- Iterative Learning Control in Health Care: Electrical Stimulation and Robotic-Assisted Upper-Limb Stroke RehabilitationDocument26 pagesIterative Learning Control in Health Care: Electrical Stimulation and Robotic-Assisted Upper-Limb Stroke RehabilitationantiwongNo ratings yet
- Effects of Fundamental Movement Skills Training On Children With Developmental Coordination DisorderDocument23 pagesEffects of Fundamental Movement Skills Training On Children With Developmental Coordination DisorderAna paula CamargoNo ratings yet
- Gpsych 2018 000009Document9 pagesGpsych 2018 000009Ana paula CamargoNo ratings yet
- Evidence-Informed Milestones For Developmental Surveillance ToolsDocument29 pagesEvidence-Informed Milestones For Developmental Surveillance Toolsjaque mouraNo ratings yet
- Genetic and Genomics in Congenital Heart Disease: A Clinical ReviewDocument10 pagesGenetic and Genomics in Congenital Heart Disease: A Clinical ReviewAna paula CamargoNo ratings yet
- A Five-Week Exercise ProgramDocument11 pagesA Five-Week Exercise ProgramWahyu Wiji PamungkasNo ratings yet
- Brain Stimulation: SciencedirectDocument3 pagesBrain Stimulation: SciencedirectAna paula CamargoNo ratings yet
- Bilateral Theta-Burst Magnetic Stimulation Influence On Event-Related Brain PotentialsDocument13 pagesBilateral Theta-Burst Magnetic Stimulation Influence On Event-Related Brain PotentialsAna paula CamargoNo ratings yet
- 07 Prevalence of Autism Spectrum Disorder AmongDocument16 pages07 Prevalence of Autism Spectrum Disorder AmongMarcela LimaNo ratings yet
- Does Corticospinal Tract Connectivity Influence The Response To Intensive Bimanual Therapy in Children With Unilateral Cerebral Palsy?Document11 pagesDoes Corticospinal Tract Connectivity Influence The Response To Intensive Bimanual Therapy in Children With Unilateral Cerebral Palsy?Ana paula CamargoNo ratings yet
- Studyprotocol Open Access: Grecco Et Al. BMC Pediatrics 2013, 13:168Document11 pagesStudyprotocol Open Access: Grecco Et Al. BMC Pediatrics 2013, 13:168Ana paula CamargoNo ratings yet
- A Longitudinal Analysis of Gross Motor Coordination in Overweight and Obese Children Versus Normal-Weight PeersDocument7 pagesA Longitudinal Analysis of Gross Motor Coordination in Overweight and Obese Children Versus Normal-Weight PeersAna paula CamargoNo ratings yet
- Artigo 7.09Document5 pagesArtigo 7.09Ana paula CamargoNo ratings yet
- Brain Stimulation: SciencedirectDocument3 pagesBrain Stimulation: SciencedirectAna paula CamargoNo ratings yet
- Brazilian Journal of Physical TherapyDocument6 pagesBrazilian Journal of Physical TherapyAna paula CamargoNo ratings yet
- Systematic Review of The Main Motor Scales For Clinical Assessment of Individuals With Down SyndromeDocument12 pagesSystematic Review of The Main Motor Scales For Clinical Assessment of Individuals With Down SyndromeAna paula CamargoNo ratings yet
- Clinical Tools Used in Young Infants Born Very Preterm To Predict Motor and Cognitive Delay (Not Cerebral Palsy) : A Systematic ReviewDocument9 pagesClinical Tools Used in Young Infants Born Very Preterm To Predict Motor and Cognitive Delay (Not Cerebral Palsy) : A Systematic ReviewAna paula CamargoNo ratings yet
- Effectiveness of Hammock Positioning in Reducing Pain and Improving Sleep-Wakefulness State in Preterm InfantsDocument6 pagesEffectiveness of Hammock Positioning in Reducing Pain and Improving Sleep-Wakefulness State in Preterm InfantsAna paula CamargoNo ratings yet
- NIV For CFDocument72 pagesNIV For CFAna paula CamargoNo ratings yet
- Respiratory Muscle Training For CFDocument41 pagesRespiratory Muscle Training For CFAna paula CamargoNo ratings yet
- Acupuncture and The Retrospect of Its Modern Research: E V I E WDocument8 pagesAcupuncture and The Retrospect of Its Modern Research: E V I E WAna paula CamargoNo ratings yet
- En - 2316 9117 FP 26 04 380Document14 pagesEn - 2316 9117 FP 26 04 380Ana paula CamargoNo ratings yet
- PEP Physiotheraphy For Arway Clearance in People With CFDocument91 pagesPEP Physiotheraphy For Arway Clearance in People With CFAna paula CamargoNo ratings yet
- Importance of Initiating A "Tummy Time" Intervention Early in Infants With Down SyndromeDocument8 pagesImportance of Initiating A "Tummy Time" Intervention Early in Infants With Down SyndromeAna paula CamargoNo ratings yet
- Activity Performance CurvesDocument12 pagesActivity Performance CurvesAna paula CamargoNo ratings yet
- Artigo 7.09Document5 pagesArtigo 7.09Ana paula CamargoNo ratings yet
- Hanna Et Al., 2009Document8 pagesHanna Et Al., 2009Ana paula CamargoNo ratings yet
- Systematic Review of The Main Motor Scales For Clinical Assessment of Individuals With Down SyndromeDocument12 pagesSystematic Review of The Main Motor Scales For Clinical Assessment of Individuals With Down SyndromeAna paula CamargoNo ratings yet
- Systematic Review of The Main Motor Scales For Clinical Assessment of Individuals With Down SyndromeDocument12 pagesSystematic Review of The Main Motor Scales For Clinical Assessment of Individuals With Down SyndromeAna paula CamargoNo ratings yet
- Rock Solid Immunity, Naturally - by Rajeev Agarwal R3Document5 pagesRock Solid Immunity, Naturally - by Rajeev Agarwal R3Rajeev B AgarwalNo ratings yet
- AOTA Statement On Role of OT in NICUDocument9 pagesAOTA Statement On Role of OT in NICUMapi RuizNo ratings yet
- Exercises For Task 3 InglesDocument3 pagesExercises For Task 3 InglesNoelia De Los SantosNo ratings yet
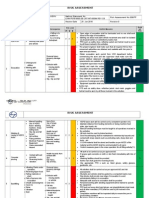
- Hse Risk Assessment - 006 Ra - Hdpe Duct LayingDocument7 pagesHse Risk Assessment - 006 Ra - Hdpe Duct Layingbinunalukandam83% (12)
- UG MaharashtraNationalLawUniversityMNLUMumbaiDocument5 pagesUG MaharashtraNationalLawUniversityMNLUMumbaiArpan KushwahaNo ratings yet
- Preface: Color Profile: Disabled Composite Default ScreenDocument2 pagesPreface: Color Profile: Disabled Composite Default ScreenCláudio CastroNo ratings yet
- Ulcerative ColitisDocument12 pagesUlcerative Colitisthap87No ratings yet
- Round Hill Community Garden FAQ - Round Hill, VirginiaDocument3 pagesRound Hill Community Garden FAQ - Round Hill, VirginiaZafiriou MavrogianniNo ratings yet
- Strain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorDocument1 pageStrain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorUdaydeep SinghNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormAlintana JobelleNo ratings yet
- VGEC 2024_Thư mời hội nghịDocument8 pagesVGEC 2024_Thư mời hội nghịkhongquantam101010No ratings yet
- Top 5 Consumer Court CasesDocument7 pagesTop 5 Consumer Court CasesTanishka SoniNo ratings yet
- Managing STEM AthletesDocument13 pagesManaging STEM Athletesanon_629662799No ratings yet
- Metabolic Surge - Rapid Fat Loss ProgramDocument5 pagesMetabolic Surge - Rapid Fat Loss ProgramTamer Luka100% (2)
- ESCAPE Study - JAMA 2005Document9 pagesESCAPE Study - JAMA 2005MICHAEL AMARILLO CORREANo ratings yet
- 1992 2007 Kpds Ilgisiz Cumle Sorulari Seyfihocacom - Pdf.pdfsifreDocument24 pages1992 2007 Kpds Ilgisiz Cumle Sorulari Seyfihocacom - Pdf.pdfsifreozgurekinsuNo ratings yet
- 1.2 POWERPOINT History of ForensicsDocument23 pages1.2 POWERPOINT History of ForensicsSilay Parole & ProbationNo ratings yet
- 50 Human Studies Identify High Risks of Prenatal Ultrasound - The Healthy Home EconomistDocument26 pages50 Human Studies Identify High Risks of Prenatal Ultrasound - The Healthy Home EconomistkromotNo ratings yet
- Breaking The Silence - Art TherapyDocument43 pagesBreaking The Silence - Art TherapyAdriana100% (1)
- List of Mandatory Documents: Document Checklist For Medical Treatment Visa Forms Can Be Downloaded atDocument2 pagesList of Mandatory Documents: Document Checklist For Medical Treatment Visa Forms Can Be Downloaded atAdegokeNo ratings yet
- EBM TerbaruDocument5 pagesEBM TerbaruTetty PrasetyaNo ratings yet
- Grand Unification For World Peace Music THerapy For Integrating Healthcare PDFDocument339 pagesGrand Unification For World Peace Music THerapy For Integrating Healthcare PDFDr Suvarna NalapatNo ratings yet
- Head To Toe Patient AssessmentDocument2 pagesHead To Toe Patient AssessmentJaypee Nuñez100% (2)
- Affidavit of Accident Dominador Rosario BagamaspadDocument2 pagesAffidavit of Accident Dominador Rosario BagamaspadJaime GonzalesNo ratings yet
- Effects of Energy Gel Ingestion On Blood Glucose, Lactate, and Performance Measures During Prolonged CyclingDocument9 pagesEffects of Energy Gel Ingestion On Blood Glucose, Lactate, and Performance Measures During Prolonged Cyclingjose david HerreraNo ratings yet
- HSE Management Plan Rev. 08Document61 pagesHSE Management Plan Rev. 08rajaNo ratings yet
- CPT 2021 guide for identifying medical proceduresDocument7 pagesCPT 2021 guide for identifying medical proceduresChester FernandezNo ratings yet
- Vitamin Water - Arnel Ricafranca PDFDocument32 pagesVitamin Water - Arnel Ricafranca PDFAlaa EssamNo ratings yet
- Reading Skills in 350 WordsDocument16 pagesReading Skills in 350 WordsCarthy Tang100% (2)
- RaweDocument34 pagesRaweSonuNo ratings yet