You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- HEALTH K 12 Curriculum Guide Grades 1 and 7Document14 pagesHEALTH K 12 Curriculum Guide Grades 1 and 7Vanessa Ann Cabello ElbanoNo ratings yet
- Changes in Infectious Disease Mortality In.5Document5 pagesChanges in Infectious Disease Mortality In.5TakaNo ratings yet
- Tujuan Pembangunan Milenium: (Millenium Development Goals, MDGS)Document12 pagesTujuan Pembangunan Milenium: (Millenium Development Goals, MDGS)TakaNo ratings yet
- Erlen Rosance Faturaja. Tugas Farmasi KlinikDocument1 pageErlen Rosance Faturaja. Tugas Farmasi KlinikTakaNo ratings yet
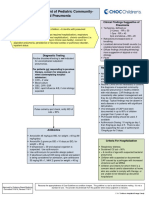
- Outpatient Management of Pediatric Community-Acquired PneumoniaDocument2 pagesOutpatient Management of Pediatric Community-Acquired PneumoniaTakaNo ratings yet
- Erlen Rosance Faturaja. Tugas Farmasi KlinikDocument1 pageErlen Rosance Faturaja. Tugas Farmasi KlinikTakaNo ratings yet
- VentolinDocument4 pagesVentolinTakaNo ratings yet
- Type 2 Diabetes Mellitus and Psychological Stress - A Modifiable Risk FactorDocument15 pagesType 2 Diabetes Mellitus and Psychological Stress - A Modifiable Risk FactorTakaNo ratings yet
- IFCCstd PDFDocument4 pagesIFCCstd PDFPaulina LizzethNo ratings yet
- GratitudeJournalingIntervention Schache2019Document5 pagesGratitudeJournalingIntervention Schache2019TakaNo ratings yet
- The Biopharmaceutical Anomaly: FeatureDocument8 pagesThe Biopharmaceutical Anomaly: FeatureTakaNo ratings yet
- Hba Standardisation: History, Science and Politics: CommentaryDocument6 pagesHba Standardisation: History, Science and Politics: CommentaryTakaNo ratings yet
- Use of Glycated Haemoglobin (Hba1C) in The Diagnosis of Diabetes MellitusDocument25 pagesUse of Glycated Haemoglobin (Hba1C) in The Diagnosis of Diabetes MellitusSiskawati Suparmin100% (1)
- Glycated Hemoglobin.....Document9 pagesGlycated Hemoglobin.....TakaNo ratings yet
- Therapies For Type 2 Diabetes: Lowering Hba1C and Associated Cardiovascular Risk FactorsDocument13 pagesTherapies For Type 2 Diabetes: Lowering Hba1C and Associated Cardiovascular Risk FactorsTakaNo ratings yet
- Therapies For Type 2 Diabetes: Lowering Hba1C and Associated Cardiovascular Risk FactorsDocument13 pagesTherapies For Type 2 Diabetes: Lowering Hba1C and Associated Cardiovascular Risk FactorsTakaNo ratings yet
- 2992 PDF PDFDocument4 pages2992 PDF PDFTakaNo ratings yet
- 2992 PDF PDFDocument4 pages2992 PDF PDFTakaNo ratings yet
- Research in Social and Administrative Pharmacy: A B A ADocument11 pagesResearch in Social and Administrative Pharmacy: A B A AYusufAbdullahKhaidirNo ratings yet
- HHS Public Access: Stress and A1c Among People With Diabetes Across The LifespanDocument16 pagesHHS Public Access: Stress and A1c Among People With Diabetes Across The LifespanTakaNo ratings yet
- Nihms 1044222 PDFDocument18 pagesNihms 1044222 PDFTakaNo ratings yet
- PI e HBA1C - ONE 16 PDFDocument2 pagesPI e HBA1C - ONE 16 PDFTakaNo ratings yet
- Use of Glycated Haemoglobin (Hba1C) in The Diagnosis of Diabetes MellitusDocument25 pagesUse of Glycated Haemoglobin (Hba1C) in The Diagnosis of Diabetes MellitusSiskawati Suparmin100% (1)
- Relationship Between Depression and Stress With Blood Sugar Levels in Patients With Diabetes Melitus 7841 PDFDocument5 pagesRelationship Between Depression and Stress With Blood Sugar Levels in Patients With Diabetes Melitus 7841 PDFTakaNo ratings yet
- The Role of A Community Pharmacist in Diabetes EducationDocument3 pagesThe Role of A Community Pharmacist in Diabetes EducationTakaNo ratings yet
- Pharmacy 08 00193 v2 PDFDocument9 pagesPharmacy 08 00193 v2 PDFTakaNo ratings yet
- How Clinical Pharmacists Can Improve Outpatient Diabetes Care PDFDocument3 pagesHow Clinical Pharmacists Can Improve Outpatient Diabetes Care PDFTakaNo ratings yet
- Circoutcomes 115 002184 PDFDocument9 pagesCircoutcomes 115 002184 PDFTakaNo ratings yet
- Role of Clinical Pharmacist in The Management of Type II Diabetes Mellitus and Its Outcomes PDFDocument7 pagesRole of Clinical Pharmacist in The Management of Type II Diabetes Mellitus and Its Outcomes PDFTakaNo ratings yet
- Pharmacists' Attitudes and Role in Diabetes Management in KuwaitDocument7 pagesPharmacists' Attitudes and Role in Diabetes Management in KuwaitTakaNo ratings yet
- PAE Sulistyorini PDFDocument17 pagesPAE Sulistyorini PDFTakaNo ratings yet
- TB WorkplaceDocument4 pagesTB WorkplaceGigi CabanaNo ratings yet
- HIV AIDS and SRH UpdatedDocument327 pagesHIV AIDS and SRH UpdatedEyob DestaNo ratings yet
- ACSM - 2007 SpringDocument7 pagesACSM - 2007 SpringTeo SuciuNo ratings yet
- Health Extension Program in EthiopiaDocument34 pagesHealth Extension Program in Ethiopianimona berhanuNo ratings yet
- Global Health Issues, Challenges and Trends The Importance of Global HealthDocument10 pagesGlobal Health Issues, Challenges and Trends The Importance of Global HealthIan James P. BranganNo ratings yet
- CHN FinalDocument3 pagesCHN FinalMañoza, MarifeNo ratings yet
- GFBR9Document42 pagesGFBR9emsanchezNo ratings yet
- Using Alcohol Screening and Brief Intervention To Address Patients' Risky DrinkingDocument5 pagesUsing Alcohol Screening and Brief Intervention To Address Patients' Risky DrinkingfasdunitedNo ratings yet
- NURS FPX 6614 Assessment 3 Disseminating The Evidence Scholarly Video Media SubmissionDocument7 pagesNURS FPX 6614 Assessment 3 Disseminating The Evidence Scholarly Video Media SubmissionEmma WatsonNo ratings yet
- Bps Nursing RFP 2018Document32 pagesBps Nursing RFP 2018sconnors13No ratings yet
- Vision 2015: Medical Council of IndiaDocument60 pagesVision 2015: Medical Council of IndiaAli Hyder SyedNo ratings yet
- History, Evolution & Classification of HospitalsDocument10 pagesHistory, Evolution & Classification of HospitalsAnonymous ibmeej9100% (1)
- Reporter Issue 765Document32 pagesReporter Issue 765backbackNo ratings yet
- Apollo-Annual Report 2016 PDFDocument143 pagesApollo-Annual Report 2016 PDFShriniket PatilNo ratings yet
- Primary Health Care Notes Health What Is Illness and Causes of Illness?Document22 pagesPrimary Health Care Notes Health What Is Illness and Causes of Illness?Nano KaNo ratings yet
- Former Seattle Firefighters LawsitDocument14 pagesFormer Seattle Firefighters LawsitDaily Caller News FoundationNo ratings yet
- Reliability and Predictive Validity of Inlow's 60-Second Diabetic Foot Screen ToolDocument6 pagesReliability and Predictive Validity of Inlow's 60-Second Diabetic Foot Screen ToolburhanNo ratings yet
- Item 2 Models of Health and Health CareDocument7 pagesItem 2 Models of Health and Health CareSarah LambleyNo ratings yet
- CRM NotesDocument41 pagesCRM NotesSitaKumariNo ratings yet
- CPH Lec ReviewrDocument24 pagesCPH Lec ReviewrCresma Santa Rayjane DesamparoNo ratings yet
- Health Indicators and Health Determinants L 8Document33 pagesHealth Indicators and Health Determinants L 8Female calmNo ratings yet
- New York Medicaid APG CrosswalkDocument6,734 pagesNew York Medicaid APG CrosswalksdpetesrhsNo ratings yet
- Mental Health Atlas - 2017 Questionnaire: Department of Mental Health and Substance Abuse World Health OrganizationDocument20 pagesMental Health Atlas - 2017 Questionnaire: Department of Mental Health and Substance Abuse World Health OrganizationMemmo AgirreNo ratings yet
- From Eco Pathology' To Agroecosystem Health'Document18 pagesFrom Eco Pathology' To Agroecosystem Health'GemaNo ratings yet
- Assess The Knowledge and Attitude On Prevention of Dengue Among The Patients AttendantsDocument6 pagesAssess The Knowledge and Attitude On Prevention of Dengue Among The Patients AttendantsIJAR JOURNALNo ratings yet
- Failure To ThriveDocument8 pagesFailure To ThriveFitria AhdiyantiNo ratings yet
- Inclusiveness Chapter - 3Document14 pagesInclusiveness Chapter - 3SKY Stationery100% (1)
- Sector Grant and Budget Guidelines 2017/18Document152 pagesSector Grant and Budget Guidelines 2017/18NsubugaNo ratings yet
- The Pathological Effects of Hyperglycaemia On The Cardiovascular (CV) System and BrainDocument5 pagesThe Pathological Effects of Hyperglycaemia On The Cardiovascular (CV) System and BrainRyzka Izza MayFanyNo ratings yet