You might also like
- HAPP-PICO Tissue Pathology Journal ResearchDocument4 pagesHAPP-PICO Tissue Pathology Journal ResearchArlynn MartinezNo ratings yet
- Psoriasis: Common DermatosesDocument7 pagesPsoriasis: Common DermatoseslaluneNo ratings yet
- Ichthyosis: A Road Model For Skin Research: Review ArticleDocument10 pagesIchthyosis: A Road Model For Skin Research: Review ArticlebaihaqiNo ratings yet
- Dermatologia: Anais Brasileiros deDocument3 pagesDermatologia: Anais Brasileiros deSango AyraNo ratings yet
- Herediter and Acquired Ichthyosis VulgarisDocument4 pagesHerediter and Acquired Ichthyosis VulgarisprajnamitaNo ratings yet
- Peeling SindromeDocument3 pagesPeeling Sindromecrisalet1No ratings yet
- Eritroderma - Bolognia 4th EditionDocument15 pagesEritroderma - Bolognia 4th EditionAisyahNo ratings yet
- Lupus Er Ythematosus: EpidemiologyDocument55 pagesLupus Er Ythematosus: EpidemiologyJelena BajagicNo ratings yet
- Scleroderma: Ivory-ColoredDocument5 pagesScleroderma: Ivory-ColoredRiena Austine Leonor NarcillaNo ratings yet
- Diagnosis of Atopic Dermatitis: Mimics, Overlaps, and ComplicationsDocument35 pagesDiagnosis of Atopic Dermatitis: Mimics, Overlaps, and ComplicationsneleaNo ratings yet
- Cutis Laxa Syndrome in Siblings Confirmed by Genetic TestingDocument4 pagesCutis Laxa Syndrome in Siblings Confirmed by Genetic TestingSunil MulgundNo ratings yet
- Common Cutaneous Disorders in ElderlyDocument6 pagesCommon Cutaneous Disorders in Elderlyirvinaldi9No ratings yet
- Desordenes Comunes de AmazonasDocument6 pagesDesordenes Comunes de AmazonasJessica RuizNo ratings yet
- Atypical Manifestations of Tinea Corporis: Case ReportsDocument5 pagesAtypical Manifestations of Tinea Corporis: Case ReportsMuhammad HafizuddinNo ratings yet
- Humano Bongiorno2009 Unusual Clinical Variants of Cutaneous Leishmaniasis in SicilyDocument4 pagesHumano Bongiorno2009 Unusual Clinical Variants of Cutaneous Leishmaniasis in SicilyFabíola AndradeNo ratings yet
- D. AtopikDocument4 pagesD. AtopikDias SeptariiaNo ratings yet
- Chapter 19 - Fever and RashDocument11 pagesChapter 19 - Fever and RashSerious LeoNo ratings yet
- Scleroderma: Quick Recertific Ation SeriesDocument2 pagesScleroderma: Quick Recertific Ation SeriesvieeveeNo ratings yet
- Scleroderma - Oral Manifestations and Treatment ChallengesDocument5 pagesScleroderma - Oral Manifestations and Treatment ChallengesLujainNo ratings yet
- Cancer Sweating GuideDocument11 pagesCancer Sweating GuidedocbinNo ratings yet
- X-Linked Ichthyosis: An Oculocutaneous Genodermatosis: EviewDocument6 pagesX-Linked Ichthyosis: An Oculocutaneous Genodermatosis: EviewTrustia RizqandaruNo ratings yet
- Oral Ulcers 1Document6 pagesOral Ulcers 1Khushbu MehtaNo ratings yet
- Ewa OsuchDocument5 pagesEwa OsuchNurmega Kurnia SaputriNo ratings yet
- 2019 Zebras in Foreskin Dermatopathology (Natural Circumcision)Document6 pages2019 Zebras in Foreskin Dermatopathology (Natural Circumcision)msdsubNo ratings yet
- 334-Article Text-1213-1-10-20160514Document7 pages334-Article Text-1213-1-10-20160514Balakrishna GopinathNo ratings yet
- Lichenoid and Interface DermatosesDocument13 pagesLichenoid and Interface DermatosesArlen ElisaNo ratings yet
- Skin Manifestations of Systemic Disease: Key PointsDocument7 pagesSkin Manifestations of Systemic Disease: Key PointsJUAN DAVID RESTREPO MARINNo ratings yet
- Perioral Dermatitis 2011Document5 pagesPerioral Dermatitis 2011Hamza Abu HumaidNo ratings yet
- Approach To Reticulate Hyperpigmentation: Clinical Dermatology - Review ArticleDocument8 pagesApproach To Reticulate Hyperpigmentation: Clinical Dermatology - Review ArticledelfiaNo ratings yet
- Rheumatic Skin DiseasesDocument31 pagesRheumatic Skin DiseasesNour SamadNo ratings yet
- By Dr. Nouran Abou Khedr: Xeroderma PigmentosumDocument6 pagesBy Dr. Nouran Abou Khedr: Xeroderma PigmentosumBahaa ShaabanNo ratings yet
- Annular LesionsDocument8 pagesAnnular LesionshpmcentreNo ratings yet
- Beetle Dermatitis StudyDocument3 pagesBeetle Dermatitis StudyKarina Terry AmartiniNo ratings yet
- Psoriasis Case Report on 33-Year-Old MaleDocument7 pagesPsoriasis Case Report on 33-Year-Old Malenathalia gabriellaNo ratings yet
- Disorders of Abnormal Keratinization Classification and ExamplesDocument9 pagesDisorders of Abnormal Keratinization Classification and Examplessoumalya481No ratings yet
- Splenomegaly by DR Bashir Ahmed Dar Associate Professor Medicine Chinkipora Sopore Kashmir Email Drbashir123@Document96 pagesSplenomegaly by DR Bashir Ahmed Dar Associate Professor Medicine Chinkipora Sopore Kashmir Email Drbashir123@Prof Dr Bashir Ahmed Dar Chinki Pora Sopore Kashmir100% (3)
- Target and targetoid lesions in dermatology.copyDocument5 pagesTarget and targetoid lesions in dermatology.copyKuldeepSinghBanaNo ratings yet
- Seminars in Diagnostic Pathology: Mark R. WickDocument11 pagesSeminars in Diagnostic Pathology: Mark R. WickAbdillah AkbarNo ratings yet
- Alniaimi 2008Document6 pagesAlniaimi 2008Laura GarciaNo ratings yet
- Dermatopathology For The Surgical Pathologist A Pattern-Based Approach To The Diagnosis of Inflammatory Skin Disorders Part IDocument21 pagesDermatopathology For The Surgical Pathologist A Pattern-Based Approach To The Diagnosis of Inflammatory Skin Disorders Part IkarigargiuloNo ratings yet
- Psoriasis Western and Ayurvedic Approaches To Treatment by Kim TamiettiDocument13 pagesPsoriasis Western and Ayurvedic Approaches To Treatment by Kim TamiettiEstudio LFANo ratings yet
- A Case of Ehlers Danlos Syndrome Associated With Cleft Lip and Palate Okamura 1984Document6 pagesA Case of Ehlers Danlos Syndrome Associated With Cleft Lip and Palate Okamura 1984elmancuernoNo ratings yet
- Cutaneous Lesions of The Canine ScrotumDocument14 pagesCutaneous Lesions of The Canine ScrotumLuciana Diegues100% (1)
- Bullous, Pseudobullous & Pustular Skin DiseasesDocument11 pagesBullous, Pseudobullous & Pustular Skin DiseasesCynthia OktariszaNo ratings yet
- Icthyosis As A Manifestation of Internal DiseaseDocument24 pagesIcthyosis As A Manifestation of Internal DiseaseSRIRAM CKNo ratings yet
- Eosinophilic DermatosesDocument15 pagesEosinophilic DermatosesmikelNo ratings yet
- 11 194scleroderma A Case ReportDocument3 pages11 194scleroderma A Case ReportAfiatul MukarromahNo ratings yet
- Hallmark: Thickened Skin: Green Book and Additional NotesDocument6 pagesHallmark: Thickened Skin: Green Book and Additional NotesVon HippoNo ratings yet
- Update on Diagnosis and Topical Management of ErythrasmaDocument4 pagesUpdate on Diagnosis and Topical Management of ErythrasmaJeliny Bintan MaisuriNo ratings yet
- 1 s2.0 S0738081X15001200 MainDocument4 pages1 s2.0 S0738081X15001200 MainPeem PrinNo ratings yet
- Cellulitis Treatment and SymptomsDocument37 pagesCellulitis Treatment and SymptomswindhymonicaNo ratings yet
- Presentation Advanced TechnologyDocument26 pagesPresentation Advanced Technologyahmad allalaNo ratings yet
- Lupus Erythematosus - Considerations For DentistryDocument10 pagesLupus Erythematosus - Considerations For DentistryJessica BastoNo ratings yet
- Lamb 2017Document6 pagesLamb 2017Carolina González RiveraNo ratings yet
- ErythrodermaDocument48 pagesErythrodermaShwan OmarNo ratings yet
- Case StudyDocument12 pagesCase StudyEllen Diana CortelNo ratings yet
- Perioral Dermatitis: Acta Dermatovenerologica Croatica: ADC / Hrvatsko Dermatolosko Drustvo February 2008Document6 pagesPerioral Dermatitis: Acta Dermatovenerologica Croatica: ADC / Hrvatsko Dermatolosko Drustvo February 2008Firdani MutiaraNo ratings yet
- Derma-Chronicles-issue 1 - 26-5-16 HiResDocument4 pagesDerma-Chronicles-issue 1 - 26-5-16 HiResParthMairNo ratings yet
- Covid 19 CPR 7 RulesDocument21 pagesCovid 19 CPR 7 RulesMiguel Cuevas DolotNo ratings yet
- How Can Patients Visitors Help - May18Document2 pagesHow Can Patients Visitors Help - May18Miguel Cuevas DolotNo ratings yet
- Clinical Examination of The Ear, Nose and Throat: Dave Pothier ST Mary's 2003Document30 pagesClinical Examination of The Ear, Nose and Throat: Dave Pothier ST Mary's 2003Ekambaram TrmNo ratings yet
- Covid 19 CPR 7 RulesDocument21 pagesCovid 19 CPR 7 RulesMiguel Cuevas DolotNo ratings yet
- Effectiveness of Transdermal MagnesiumDocument2 pagesEffectiveness of Transdermal MagnesiumMiguel Cuevas Dolot100% (1)
- ACLS Cardiac Arrest Algorithm For Suspected or Confirmed COVID-19 PatientsDocument1 pageACLS Cardiac Arrest Algorithm For Suspected or Confirmed COVID-19 PatientsMariuxi Tatiana ChocoNo ratings yet
- (MED) COVID-19 Trans V. 2.0Document6 pages(MED) COVID-19 Trans V. 2.0Isabel VinasNo ratings yet
- Physical Examination in ENT: Ussana Promyothin, MDDocument60 pagesPhysical Examination in ENT: Ussana Promyothin, MDMiguel Cuevas DolotNo ratings yet
- Cook Book (Filipino) 13 PDFDocument23 pagesCook Book (Filipino) 13 PDFAdina AnghelNo ratings yet
- Covid 19 PDFDocument18 pagesCovid 19 PDFMiguel Cuevas DolotNo ratings yet
- Benign Paroxysmal Positional Vertigo: Waseem WatadDocument37 pagesBenign Paroxysmal Positional Vertigo: Waseem WatadnoviNo ratings yet
- Pedia Tickler Update 2017Document2 pagesPedia Tickler Update 2017Tani BokNo ratings yet
- Physical Examination in ENT: Ussana Promyothin, MDDocument60 pagesPhysical Examination in ENT: Ussana Promyothin, MDMiguel Cuevas DolotNo ratings yet
- Vertigo Gail Ishiyama 1 13 10Document40 pagesVertigo Gail Ishiyama 1 13 10Myname Rama LienNo ratings yet
- A Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFDocument12 pagesA Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFMiguel Cuevas DolotNo ratings yet
- Physical Assessment: Ear, Nose, Mouth, and ThroatDocument59 pagesPhysical Assessment: Ear, Nose, Mouth, and ThroatMiguel Cuevas DolotNo ratings yet
- A Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFDocument12 pagesA Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFMiguel Cuevas DolotNo ratings yet
- Nocturnals Physiology 2018Document14 pagesNocturnals Physiology 2018Miguel Cuevas DolotNo ratings yet
- Drug IndexDocument2 pagesDrug IndexMiguel Cuevas DolotNo ratings yet
- Active Listening HANDOUT PDFDocument26 pagesActive Listening HANDOUT PDFMiguel Cuevas DolotNo ratings yet
- Clinical AbstractDocument4 pagesClinical AbstractMiguel Cuevas DolotNo ratings yet
- HEMAreviewDocument3 pagesHEMAreviewMiguel Cuevas DolotNo ratings yet
- Anesthesia Pocket Cards 7 18 18Document6 pagesAnesthesia Pocket Cards 7 18 18Miguel Cuevas DolotNo ratings yet
- Pediatric History and Physical Exam GuideDocument7 pagesPediatric History and Physical Exam GuideIndunil AnuruddhikaNo ratings yet
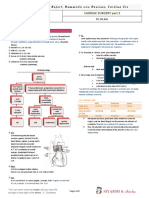
- TCVS - Cardiac Surgery Part 2 Dr. de AsisDocument8 pagesTCVS - Cardiac Surgery Part 2 Dr. de AsisMiguel Cuevas DolotNo ratings yet
- Kerosene PDFDocument31 pagesKerosene PDFRudyMLanaNo ratings yet
- Neurologic ExamDocument1 pageNeurologic ExamMiguel Cuevas DolotNo ratings yet
- Community-Acquired Pneumonia - CPG 2016Document26 pagesCommunity-Acquired Pneumonia - CPG 2016Jamie SebastianNo ratings yet
- 19C.Revolution and Counter Rev. in Ancient India PARTIII PDFDocument94 pages19C.Revolution and Counter Rev. in Ancient India PARTIII PDFVeeramani ManiNo ratings yet
- Bion W R - Complite Works Vol IIDocument272 pagesBion W R - Complite Works Vol IIjanusz100% (4)
- Test Bank For Behavior Modification Principles and Procedures 6th EditionDocument36 pagesTest Bank For Behavior Modification Principles and Procedures 6th Editionempericetagragyj6f8100% (31)
- Already GoneDocument3 pagesAlready GoneladymyaNo ratings yet
- Activityideabank FinalDocument72 pagesActivityideabank FinalJoy Tu TranNo ratings yet
- Sinha-Dhanalakshmi2019 Article EvolutionOfRecommenderSystemOv PDFDocument20 pagesSinha-Dhanalakshmi2019 Article EvolutionOfRecommenderSystemOv PDFRui MatosNo ratings yet
- Languages of The Northern HimalayasDocument358 pagesLanguages of The Northern Himalayas6755kdpNo ratings yet
- Water and Sanitation CrisisDocument4 pagesWater and Sanitation CrisisKarl EstenzoNo ratings yet
- Amarok 2011Document79 pagesAmarok 2011NPNo ratings yet
- Intro To Rhetorical FunctionDocument28 pagesIntro To Rhetorical FunctiondianNo ratings yet
- Presentation of E Commerce Website ProjectDocument13 pagesPresentation of E Commerce Website ProjectSibu Star25% (4)
- State of Employee Engagement: Global Survey 2010Document16 pagesState of Employee Engagement: Global Survey 2010aptmbaNo ratings yet
- Dessler Fund5 09Document35 pagesDessler Fund5 09api-410371654No ratings yet
- AM 2442FX AM 3242FX: User's Manual Manual Del UsuarioDocument32 pagesAM 2442FX AM 3242FX: User's Manual Manual Del UsuarioarsieiraNo ratings yet
- Indus Script - WikipediaDocument55 pagesIndus Script - WikipediaMuhammad Afzal BrohiNo ratings yet
- ManpowerGroup Total Employment Management Solution PDFDocument1 pageManpowerGroup Total Employment Management Solution PDFAMERICO SANTIAGONo ratings yet
- The Advanced Trauma Operative Management Course inDocument6 pagesThe Advanced Trauma Operative Management Course inFathiH.SaadNo ratings yet
- Chapter 1 ReviewDocument6 pagesChapter 1 ReviewSolyKalNo ratings yet
- Love Letters Reveal Deep EmotionsDocument21 pagesLove Letters Reveal Deep EmotionsChima NnosimikeNo ratings yet
- Parallel Worlds ChessDocument2 pagesParallel Worlds ChessRobert BonisoloNo ratings yet
- Saint Aquinas and Mercantilism School of ThoughtsDocument11 pagesSaint Aquinas and Mercantilism School of ThoughtsKatunga MwiyaNo ratings yet
- Exam StructuralDocument1 pageExam StructuralJoyce DueroNo ratings yet
- Sample Questions For RTI ActDocument5 pagesSample Questions For RTI ActAnjali RaiNo ratings yet
- Protein Expression HandbookDocument118 pagesProtein Expression HandbookLuis Arístides Torres SánchezNo ratings yet
- User's Manual: & Technical DocumentationDocument20 pagesUser's Manual: & Technical DocumentationPODOSALUD HUANCAYONo ratings yet
- The Small Trees High Productivity Initiative: Principles and Practice in High Density Orchard DesignDocument1 pageThe Small Trees High Productivity Initiative: Principles and Practice in High Density Orchard DesignPutchong SaraNo ratings yet
- Data Compilation TemplateDocument257 pagesData Compilation TemplateemelyseuwaseNo ratings yet
- Gauda Kingdom - WikipediaDocument4 pagesGauda Kingdom - Wikipediaolivernora777No ratings yet
- CV - Diego Allendes - Civil EngineerDocument1 pageCV - Diego Allendes - Civil EngineerPari D. ShitPostingNo ratings yet
- 33 1-3 - 093 - J Dilla's Donuts - Jordan Ferguson (Retail) PDFDocument147 pages33 1-3 - 093 - J Dilla's Donuts - Jordan Ferguson (Retail) PDFNicolas GomezNo ratings yet