You might also like
- Suture and Staple RemovalDocument15 pagesSuture and Staple RemovalRajaNo ratings yet
- Vol28 I4 Non-Invasive External PDFDocument5 pagesVol28 I4 Non-Invasive External PDFSilvia Febrieni Puspitasari MulyonoNo ratings yet
- Facial Fat FitnessDocument13 pagesFacial Fat FitnessDaniela GonzalezNo ratings yet
- MesoterapiaDocument139 pagesMesoterapiaVeronica Tomasello100% (1)
- 2005 Mesotherapy For Body ContouringDocument5 pages2005 Mesotherapy For Body ContouringDra. Tatiane FariaNo ratings yet
- Refinement of Technique in Injection Lipolysis Based On Scientific Studies and Clinical EvaluationDocument15 pagesRefinement of Technique in Injection Lipolysis Based On Scientific Studies and Clinical EvaluationtassianaNo ratings yet
- Topical Aminophylline: Is It Safe and Effective in Causing Regional Fat Loss?Document4 pagesTopical Aminophylline: Is It Safe and Effective in Causing Regional Fat Loss?Brian MacíaNo ratings yet
- Journal of Exercise Science & FitnessDocument6 pagesJournal of Exercise Science & FitnessDoraisy SHNo ratings yet
- The Science of Mesotherapy: Chemical Anarchy: Hot TopicsDocument4 pagesThe Science of Mesotherapy: Chemical Anarchy: Hot Topics小次郎 佐々木No ratings yet
- Low Frequency Ultrasound Cavitation Versus Phosphatidylcholine Injection On Fat Adiposity in Women With Gynoid ObesityDocument5 pagesLow Frequency Ultrasound Cavitation Versus Phosphatidylcholine Injection On Fat Adiposity in Women With Gynoid ObesityCarola AlvaradoNo ratings yet
- Fat Reduction. Pathophysiology and Treatment Strategies (Liposuction)Document13 pagesFat Reduction. Pathophysiology and Treatment Strategies (Liposuction)Anonymous LnWIBo1GNo ratings yet
- Effect of High-Intensity Interval Training On Total, Abdominal and Visceral Fat Mass: A Meta-AnalysisDocument23 pagesEffect of High-Intensity Interval Training On Total, Abdominal and Visceral Fat Mass: A Meta-AnalysisJuan David TarapuezNo ratings yet
- Criolipolise X CavitaçãoDocument6 pagesCriolipolise X CavitaçãoPolyana AlencarNo ratings yet
- 232-Article Text-429-1-10-20190606Document6 pages232-Article Text-429-1-10-20190606Achmad JunaidiNo ratings yet
- Dmso 4 141Document14 pagesDmso 4 141doctorbanNo ratings yet
- Zebra Fish ObeseDocument11 pagesZebra Fish ObesesultanmsajidmNo ratings yet
- Kiyoji Tanaka Maeng-Kyu Kim, Tsugio Tomita, Mi-Ji Kim, Hiroyuki Sasai, Seiji Maeda andDocument8 pagesKiyoji Tanaka Maeng-Kyu Kim, Tsugio Tomita, Mi-Ji Kim, Hiroyuki Sasai, Seiji Maeda andAnwar SiddiquiNo ratings yet
- European Journal of Integrative Medicine: Research PaperDocument7 pagesEuropean Journal of Integrative Medicine: Research PaperNatalia Franco PérezNo ratings yet
- Gluteal Augmentation With Fat GraftingDocument9 pagesGluteal Augmentation With Fat GraftingDiego Henrique MoreiraNo ratings yet
- Fphys 11 575363Document8 pagesFphys 11 575363Huda TrisenaNo ratings yet
- Mesotherapy, Microneedling, and Chemicalpeels: Johnson C. Lee,, Mark A. Daniels,, Malcolm Z. RothDocument13 pagesMesotherapy, Microneedling, and Chemicalpeels: Johnson C. Lee,, Mark A. Daniels,, Malcolm Z. RothVinicius MelloNo ratings yet
- Physical Therapy in The Treatment of Body Aesthetics Dysfuntions-Literature ReviewDocument11 pagesPhysical Therapy in The Treatment of Body Aesthetics Dysfuntions-Literature ReviewAngel Daniel Flores AmezcuaNo ratings yet
- Effect of High-Intensity Interval Training On Total, Abdominal and Visceral Fat Mass: A Meta-AnalysisDocument20 pagesEffect of High-Intensity Interval Training On Total, Abdominal and Visceral Fat Mass: A Meta-AnalysisAngelica GarciaNo ratings yet
- DRP2018 5276528Document9 pagesDRP2018 5276528cientifico FismatekNo ratings yet
- Dr. Scott Connelly Manninen56Document3 pagesDr. Scott Connelly Manninen56Sean DrewNo ratings yet
- Fat Transfer To The Face: Technique and New Concepts: Facial Plastic Surgery Clinics of North America June 2001Document10 pagesFat Transfer To The Face: Technique and New Concepts: Facial Plastic Surgery Clinics of North America June 2001Priya BabyNo ratings yet
- S0738081X21001668Document10 pagesS0738081X21001668Fajar Sartika HadiNo ratings yet
- Seminario 7 Digestion y Absorcion de Lipidos Keogh 2011Document7 pagesSeminario 7 Digestion y Absorcion de Lipidos Keogh 2011pau_sebNo ratings yet
- 9c65d8 PDFDocument7 pages9c65d8 PDFsophipepisNo ratings yet
- Nutrition, Pharmacological and Training Strategies Adopted by Six Bodybuilders: Case Report and Critical ReviewDocument17 pagesNutrition, Pharmacological and Training Strategies Adopted by Six Bodybuilders: Case Report and Critical ReviewDeepak SinghNo ratings yet
- Effectiveness of Mesotherapy On Body Contouring: BackgroundDocument7 pagesEffectiveness of Mesotherapy On Body Contouring: BackgroundNita Dewi NNo ratings yet
- Adipose Tissue: Classification & QuantificationDocument30 pagesAdipose Tissue: Classification & QuantificationAli.m DaoodNo ratings yet
- Lymph 4659 EsmerDocument8 pagesLymph 4659 Esmerr.barca98No ratings yet
- Normobaric Hyperoxygenation Enhances Initial Survival, Regeneration, and Final Retention in Fat GraftingDocument9 pagesNormobaric Hyperoxygenation Enhances Initial Survival, Regeneration, and Final Retention in Fat GraftingVanessaGGSNo ratings yet
- Efficacy of A Novel Herbal Formulation For Weight Loss Demonstrated in A 16-WeekDocument31 pagesEfficacy of A Novel Herbal Formulation For Weight Loss Demonstrated in A 16-WeekAstri YuliandiniNo ratings yet
- Vogt Belluscio Article Released OptDocument26 pagesVogt Belluscio Article Released OptDr. Daniel BelluscioNo ratings yet
- Ozonio No SobrepesoDocument7 pagesOzonio No SobrepesoGislaine BianchiNo ratings yet
- Oxidacion de Acido GrasoDocument7 pagesOxidacion de Acido GrasoLuisNo ratings yet
- Obesity - 2022 - Christoffersen - Beyond Appetite Regulation Targeting Energy Expenditure Fat Oxidation and Lean MassDocument18 pagesObesity - 2022 - Christoffersen - Beyond Appetite Regulation Targeting Energy Expenditure Fat Oxidation and Lean Massiman prawiraNo ratings yet
- Lipoplasty of The BackDocument7 pagesLipoplasty of The BackAng BiNo ratings yet
- Lipolytic DrugsDocument7 pagesLipolytic DrugsPradeep AggarwalNo ratings yet
- Irisina y EjercicioDocument7 pagesIrisina y Ejerciciojose carrasquillaNo ratings yet
- Location, Location, Location: Beneficial Effects of Autologous Fat TransplantationDocument11 pagesLocation, Location, Location: Beneficial Effects of Autologous Fat TransplantationBlanche AltheaNo ratings yet
- Red Light Vs Liposuction For Weight LossDocument15 pagesRed Light Vs Liposuction For Weight LossMark Sloan100% (1)
- Suplementacao em NutricaoDocument9 pagesSuplementacao em NutricaoJoyce CamposNo ratings yet
- Strategies To Counter Weight Loss-Induced Reductions in Metabolic RateDocument8 pagesStrategies To Counter Weight Loss-Induced Reductions in Metabolic RateAlonso FernandezNo ratings yet
- Clinical Nutrition ESPEN: Original ArticleDocument8 pagesClinical Nutrition ESPEN: Original ArticleMar DianaNo ratings yet
- Mechanisms of Weight Regain After Weight Loss - The Role of Adipose TissueDocument14 pagesMechanisms of Weight Regain After Weight Loss - The Role of Adipose TissueThiago SartiNo ratings yet
- Liposuction and Liposculpture: Francesco M. Egro, Nathaniel A. Blecher, J. Peter Rubin, and Sydney R. ColemanDocument9 pagesLiposuction and Liposculpture: Francesco M. Egro, Nathaniel A. Blecher, J. Peter Rubin, and Sydney R. Colemanโสภาพรรณวดี รวีวารNo ratings yet
- Intermitente de Alta Intensidad para Reducir GrasaDocument7 pagesIntermitente de Alta Intensidad para Reducir GrasaJennifer DuchiNo ratings yet
- Five Reasons For Doing Sprints For Physique DevelopmentDocument6 pagesFive Reasons For Doing Sprints For Physique DevelopmentIvan KulevNo ratings yet
- The Journal of Physical Therapy Science The Journal of Physical Therapy ScienceDocument4 pagesThe Journal of Physical Therapy Science The Journal of Physical Therapy ScienceSafiyah SindiNo ratings yet
- Anti-Obesity MedicationsDocument33 pagesAnti-Obesity MedicationsJorge Luis Alva AlonsoNo ratings yet
- Dry Cupping For CelluliteDocument6 pagesDry Cupping For CelluliteAndri Praja SatriaNo ratings yet
- Nunes 2018Document9 pagesNunes 2018jhomarlaiNo ratings yet
- Physical Activity and Exercise in The Regulation of Human Adipose Tissue PhysiologyDocument35 pagesPhysical Activity and Exercise in The Regulation of Human Adipose Tissue PhysiologyLISTIA NURBAETINo ratings yet
- Marta Garaulet, Francisca Pérez-Llamas, Millán Pérez-Ayala, Pedro Martínez, Fermín Sánchez de Medina, Francisco J Tebar, and Salvador ZamoraDocument7 pagesMarta Garaulet, Francisca Pérez-Llamas, Millán Pérez-Ayala, Pedro Martínez, Fermín Sánchez de Medina, Francisco J Tebar, and Salvador ZamoraZachary LeeNo ratings yet
- Mesotherapy Minimally Invasive TechniqueDocument11 pagesMesotherapy Minimally Invasive TechniqueDenisse ZayasNo ratings yet
- Combinatory Effects of Phytoestrogens and Exercise On Body Fat Mass andDocument9 pagesCombinatory Effects of Phytoestrogens and Exercise On Body Fat Mass andyhenti widjayantiNo ratings yet
- JURNAL - Jaringan AdiposaDocument10 pagesJURNAL - Jaringan AdiposaPramesvara NaoriNo ratings yet
- Lower Facial Rejuvenation Using Absorbable Casting Barbed Thread. 19 EneroDocument4 pagesLower Facial Rejuvenation Using Absorbable Casting Barbed Thread. 19 EneroLorena AcevedoNo ratings yet
- Humphrey2016 Combination Therapy in Midfacial RejuvenationDocument6 pagesHumphrey2016 Combination Therapy in Midfacial RejuvenationLorena AcevedoNo ratings yet
- Lower Facial Rejuvenation Using Absorbable Casting Barbed Thread. 19 EneroDocument4 pagesLower Facial Rejuvenation Using Absorbable Casting Barbed Thread. 19 EneroLorena AcevedoNo ratings yet
- Bleiker Et Al-2005-British Journal of DermatologyDocument10 pagesBleiker Et Al-2005-British Journal of DermatologyLorena AcevedoNo ratings yet
- NEUROTIXINASDocument11 pagesNEUROTIXINASLorena AcevedoNo ratings yet
- The Hair Follicle EnigmaDocument6 pagesThe Hair Follicle EnigmaLorena AcevedoNo ratings yet
- Quantitative Correlation Between Hyaluronic Acid Filler and Hyaluronidase.Document4 pagesQuantitative Correlation Between Hyaluronic Acid Filler and Hyaluronidase.Lorena AcevedoNo ratings yet
- Plasma For Facial Rejuvenation 10.1111@jocd.12876Document9 pagesPlasma For Facial Rejuvenation 10.1111@jocd.12876Lorena AcevedoNo ratings yet
- Consenso Dysport Tercio Sup Ascher 2010 PDFDocument7 pagesConsenso Dysport Tercio Sup Ascher 2010 PDFLorena AcevedoNo ratings yet
- 1 Consenso Carruthers2016Document12 pages1 Consenso Carruthers2016Lorena AcevedoNo ratings yet
- Exilis Elite CLIN Apoptosis-Porcine-McDaniels HQ ENDocument5 pagesExilis Elite CLIN Apoptosis-Porcine-McDaniels HQ ENLorena AcevedoNo ratings yet
- Uls Core Value: SolidarityDocument5 pagesUls Core Value: SolidarityKeith CaboteNo ratings yet
- United States v. Eastom, 10th Cir. (2009)Document20 pagesUnited States v. Eastom, 10th Cir. (2009)Scribd Government DocsNo ratings yet
- CoC - A Handful of DustDocument42 pagesCoC - A Handful of DustMikiNo ratings yet
- Ip CameraDocument2 pagesIp CameraRaghavendar Reddy BobbalaNo ratings yet
- HETP Evaluation of Structured and Randomic Packing Distillation ColumnDocument31 pagesHETP Evaluation of Structured and Randomic Packing Distillation Columnjesus_manrique2753No ratings yet
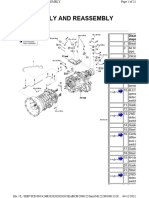
- Disassembly and Reassembly: Disas StepsDocument21 pagesDisassembly and Reassembly: Disas StepsNishanth BenedictNo ratings yet
- Digitization DigitalizationDocument1 pageDigitization Digitalizationace espinosaNo ratings yet
- Textbook Ebook The U S Banking System Laws Regulations and Risk Management 1St Ed 2020 Edition Felix I Lessambo All Chapter PDFDocument43 pagesTextbook Ebook The U S Banking System Laws Regulations and Risk Management 1St Ed 2020 Edition Felix I Lessambo All Chapter PDFjames.sheehan941100% (6)
- Answers To Eocqs: Cambridge International As Level ChemistryDocument1 pageAnswers To Eocqs: Cambridge International As Level ChemistryYashaswi Moktan100% (1)
- 03 StorekingDocument10 pages03 Storekingqwqw11No ratings yet
- Chapter 8 - Between-Subjects DesignDocument17 pagesChapter 8 - Between-Subjects DesignSumendra RathoreNo ratings yet
- Application Form: Plan International CambodiaDocument5 pagesApplication Form: Plan International CambodiaSong KeoNo ratings yet
- Thesis Shaheen AhmadDocument64 pagesThesis Shaheen AhmadCung LevanNo ratings yet
- 1 The Foundations of IncenseDocument10 pages1 The Foundations of Incensegfrankel72No ratings yet
- g+5 Building Pr1Document13 pagesg+5 Building Pr1aftabNo ratings yet
- A Study On Customer Preference For Honda H'nessDocument9 pagesA Study On Customer Preference For Honda H'nessAshokNo ratings yet
- 2nd Q Week 6 - Local Materials Used in The PhilippinesDocument26 pages2nd Q Week 6 - Local Materials Used in The PhilippinesAngel Natty New100% (1)
- ADP Systems Code, Form #09.025Document309 pagesADP Systems Code, Form #09.025Sovereignty Education and Defense Ministry (SEDM)100% (1)
- Beam Design PDFDocument2 pagesBeam Design PDFsathishlinshanNo ratings yet
- Mod 6 Fuels and CombustionDocument58 pagesMod 6 Fuels and CombustionVarsha VarmaNo ratings yet
- 037-People v. Pabalan, G.R. No. 113530 and 117819-21, Sept 30, 1996Document9 pages037-People v. Pabalan, G.R. No. 113530 and 117819-21, Sept 30, 1996Jopan SJ100% (1)
- Dfysdfys: Japanese Particles Cheat Sheet Japanese Particles Cheat SheetDocument1 pageDfysdfys: Japanese Particles Cheat Sheet Japanese Particles Cheat SheetVictor BadoiuNo ratings yet
- The Role of Riparian Corridors in Maintaining Regional Biodiversity. Naiman Et Al. 1993Document5 pagesThe Role of Riparian Corridors in Maintaining Regional Biodiversity. Naiman Et Al. 1993Iuri AmazonasNo ratings yet
- Anil's ResumeDocument1 pageAnil's ResumeAnil kumar NNo ratings yet
- ElectricalDocument43 pagesElectricalryanNo ratings yet
- Ali Raza - Franziska Roy - Benjamin Zachariah - The Internationalist Moment - South Asia, Worlds, and World Views 1917-39-SAGE Publications (2015)Document313 pagesAli Raza - Franziska Roy - Benjamin Zachariah - The Internationalist Moment - South Asia, Worlds, and World Views 1917-39-SAGE Publications (2015)adriNo ratings yet
- Aops Community Russian TST 2015: Days 1-6 Day 7 P1Document4 pagesAops Community Russian TST 2015: Days 1-6 Day 7 P1魏志恒No ratings yet
- 204 Ancient Indian BuddhismDocument21 pages204 Ancient Indian BuddhismShivu KesanoorNo ratings yet
- 21-09 Janitorial Services NFLDocument19 pages21-09 Janitorial Services NFLEmeka EzeonyilimbaNo ratings yet