You might also like
- APA Style NDocument21 pagesAPA Style NZainab SheikhNo ratings yet
- About APA StyleDocument17 pagesAbout APA StyleMazen SultanNo ratings yet
- Sample Paper For A StudentDocument4 pagesSample Paper For A StudentMāh Wīßh FātīmāNo ratings yet
- Using APA Style (7th Edition, 2020) : Edition Publication Manual of The American Psychological AssociationDocument16 pagesUsing APA Style (7th Edition, 2020) : Edition Publication Manual of The American Psychological AssociationPapiscott comedyNo ratings yet
- Apa Style Ch 2_3 SummaryDocument32 pagesApa Style Ch 2_3 Summaryماجدة صبري شايعNo ratings yet
- General Apa GuidelinesDocument8 pagesGeneral Apa GuidelinesplntbuenNo ratings yet
- Meeting 8: APA Formatting For Papers and How To Write and Format An APA AbstractDocument4 pagesMeeting 8: APA Formatting For Papers and How To Write and Format An APA AbstractcindyantNo ratings yet
- Abstract and Sections of an APA PaperDocument5 pagesAbstract and Sections of an APA PaperMartin Zarate AzorsaNo ratings yet
- APA STYLE Guide To Learning The Basics of APA Style For Manuscript Preparation Isabelle DDocument20 pagesAPA STYLE Guide To Learning The Basics of APA Style For Manuscript Preparation Isabelle DmaxikheavyNo ratings yet
- Writing Center Style Apa 7th Edition Template Without AbstractDocument5 pagesWriting Center Style Apa 7th Edition Template Without AbstractKhánh NgọcNo ratings yet
- APA 7th Template Student PaperDocument13 pagesAPA 7th Template Student PapertereNo ratings yet
- General Format (Cont'd) : Your Essay Should Include Four Major SectionsDocument6 pagesGeneral Format (Cont'd) : Your Essay Should Include Four Major SectionsaplatanskaNo ratings yet
- Apa FormatDocument16 pagesApa FormatWalidTranscendentalist100% (1)
- APA Style Sample Paper FormattingDocument5 pagesAPA Style Sample Paper Formattingbonnie reese100% (3)
- Formatting GuideDocument33 pagesFormatting GuidemugwovictorNo ratings yet
- APA Style: APA Style Is A Writing Style and Format For Academic Documents Such As Articles and BooksDocument8 pagesAPA Style: APA Style Is A Writing Style and Format For Academic Documents Such As Articles and BooksHarsha VincentNo ratings yet
- Sample Research Paper With Apa CitationDocument4 pagesSample Research Paper With Apa Citationc9hpjcb3100% (1)
- APA GuidelinesDocument43 pagesAPA GuidelinesCristy PestilosNo ratings yet
- American Psychological Association (APA) Formatting GuideDocument11 pagesAmerican Psychological Association (APA) Formatting GuideWan Nor FarehahNo ratings yet
- APA Referencing Guide - : Health Sciences, Medicine and Nursing 2008Document11 pagesAPA Referencing Guide - : Health Sciences, Medicine and Nursing 2008Tr4zrNo ratings yet
- Title of Your Paper: Your Name University Affiliation Course Name Instructor Name DateDocument6 pagesTitle of Your Paper: Your Name University Affiliation Course Name Instructor Name DateUsman KhanNo ratings yet
- APA Sample Paper 6th EditionDocument10 pagesAPA Sample Paper 6th EditionMuhammad Ikhwanul HakimNo ratings yet
- APA Presentation Updated PDFDocument32 pagesAPA Presentation Updated PDFMimeroseNo ratings yet
- APA Quick Reference GuideDocument25 pagesAPA Quick Reference Guidegent_ohnoNo ratings yet
- Purdue Owl APADocument37 pagesPurdue Owl APAdumindiNo ratings yet
- GROUP 1 Notes Research 2Document6 pagesGROUP 1 Notes Research 2celino.euniceeNo ratings yet
- Title of Your EssayDocument5 pagesTitle of Your EssayazrihazNo ratings yet
- APA Formatting & Style Guide: Edward Christian R. Gan Ma. Corazon SalazarDocument61 pagesAPA Formatting & Style Guide: Edward Christian R. Gan Ma. Corazon SalazarEdward GanNo ratings yet
- APA FormatDocument11 pagesAPA FormatSangar IsmailNo ratings yet
- Note of Research ProposalDocument5 pagesNote of Research ProposalAtiqullah sherzadNo ratings yet
- Lyceum of The Philippines University Cavite Campus DOA Coecsa A.Y. 2020-2021Document7 pagesLyceum of The Philippines University Cavite Campus DOA Coecsa A.Y. 2020-2021Learnce MasculinoNo ratings yet
- Running Head Format For APA Style Papers: Paper TitleDocument17 pagesRunning Head Format For APA Style Papers: Paper TitleJhonvee De MesaNo ratings yet
- APA Formatting EssentialsDocument39 pagesAPA Formatting EssentialsEdward GanNo ratings yet
- 4 Apa 7th EditionDocument47 pages4 Apa 7th EditionClyde Alexis Tapado Manlogon80% (5)
- Apa Format Citation For Research PaperDocument4 pagesApa Format Citation For Research Paperafeaynwqz100% (1)
- Running Head: Title of Paper 1Document5 pagesRunning Head: Title of Paper 1Meghna CmNo ratings yet
- APA Student Paper TemplateDocument5 pagesAPA Student Paper TemplatesatthgurujiNo ratings yet
- Student case study analysisDocument5 pagesStudent case study analysishermitpassi100% (1)
- Guidelines For Report Writing of Research ArticlesDocument7 pagesGuidelines For Report Writing of Research ArticlesDreamcatcherNo ratings yet
- Running Head: Guidelines For Using Apa 1Document7 pagesRunning Head: Guidelines For Using Apa 1M'Lissa Evans KurtzNo ratings yet
- APA style guide for student papersDocument8 pagesAPA style guide for student papersMuziana MuziNo ratings yet
- APA7 Template Paper W Abstract Tables 7.21Document11 pagesAPA7 Template Paper W Abstract Tables 7.21coemgen127No ratings yet
- APA7 Sample Paper AnnotatedDocument7 pagesAPA7 Sample Paper AnnotatedemiltheressebastianNo ratings yet
- Sample Apa Research Paper With in Text CitationsDocument5 pagesSample Apa Research Paper With in Text Citationsmqolulbkf100% (1)
- WCU APA Format Template 2Document6 pagesWCU APA Format Template 2madeleine raymondNo ratings yet
- APA Style Manuscript Format - BedfordDocument2 pagesAPA Style Manuscript Format - Bedfordcantor2000No ratings yet
- APA 7th Edition Paper With Mult ExperimentsDocument20 pagesAPA 7th Edition Paper With Mult ExperimentsMIA100% (1)
- APA Style Guide for Student PapersDocument33 pagesAPA Style Guide for Student PapersWided KrimNo ratings yet
- APA Example PaperDocument14 pagesAPA Example PaperSangar IsmailNo ratings yet
- Font For Research Paper ApaDocument7 pagesFont For Research Paper Apatwfmadsif100% (1)
- Formatting APA 7th GuideDocument3 pagesFormatting APA 7th GuideKRISTIAN HENRY PALOMANo ratings yet
- APA Style Student Report Template 7th Edition Ensayo T.1.9Document5 pagesAPA Style Student Report Template 7th Edition Ensayo T.1.9ananny200308No ratings yet
- GS-module 4 APA 7th EDITIONDocument46 pagesGS-module 4 APA 7th EDITIONJulia LegaspiNo ratings yet
- Research Paper Reference Page FormatDocument4 pagesResearch Paper Reference Page Formattuigauund100% (1)
- APA Formatting and Style Guide EssentialsDocument42 pagesAPA Formatting and Style Guide EssentialsKaraNo ratings yet
- Structura ReferatDocument3 pagesStructura ReferatMeditatii Limba Engleza BufteaNo ratings yet
- Running Head: Assignment Title Here 1Document5 pagesRunning Head: Assignment Title Here 1Emma Smith FiverrNo ratings yet
- Origins of Projective Tests: How Projective Tests Are Used To Measure PersonalityDocument3 pagesOrigins of Projective Tests: How Projective Tests Are Used To Measure PersonalityZainab SheikhNo ratings yet
- Psychological Assessment and Perspectives Postgraduate CollegeDocument2 pagesPsychological Assessment and Perspectives Postgraduate CollegeZainab SheikhNo ratings yet
- APA 7th Edition OverviewDocument3 pagesAPA 7th Edition OverviewZainab SheikhNo ratings yet
- Postgraduate College For Women HaripurDocument2 pagesPostgraduate College For Women HaripurZainab SheikhNo ratings yet
- Authority LetterDocument1 pageAuthority LetterZainab SheikhNo ratings yet
- APA Style and Grammar Guidelines SummaryDocument4 pagesAPA Style and Grammar Guidelines SummaryZainab SheikhNo ratings yet
- 5 Levels of Heading PDFDocument1 page5 Levels of Heading PDFZainab SheikhNo ratings yet
- New Microsoft Word DocumentDocument1 pageNew Microsoft Word DocumentZainab SheikhNo ratings yet
- PMHP Handbook 2013 PDFDocument171 pagesPMHP Handbook 2013 PDFZainab SheikhNo ratings yet
- Star BurnDocument1 pageStar BurnJ SELVA ANTONY SANTOSHNo ratings yet
- Advance Research Methods-7Document33 pagesAdvance Research Methods-7Sajjul KhanNo ratings yet
- 5 Levels of Heading PDFDocument1 page5 Levels of Heading PDFZainab SheikhNo ratings yet
- Managing Social Anxiety Disorder: Doctor Discussion GuideDocument3 pagesManaging Social Anxiety Disorder: Doctor Discussion GuideZainab SheikhNo ratings yet
- Pleasant Activity Scheduling Worksheet PDFDocument2 pagesPleasant Activity Scheduling Worksheet PDFZainab SheikhNo ratings yet
- De Catastroph I ZingDocument1 pageDe Catastroph I ZingNadera SerhanNo ratings yet
- 14 CBT With Older PeopleDocument7 pages14 CBT With Older PeopleZainab SheikhNo ratings yet
- 14 CBT With Older PeopleDocument7 pages14 CBT With Older PeopleZainab SheikhNo ratings yet
- Star BurnDocument1 pageStar BurnJ SELVA ANTONY SANTOSHNo ratings yet
- The Over Scheduled ChildDocument2 pagesThe Over Scheduled ChildGreatAkbar1No ratings yet
- CADDRA ADHD Information Resources HandoutDocument2 pagesCADDRA ADHD Information Resources HandoutMustafa AlmasoudiNo ratings yet
- Gudiance and CounsellingDocument17 pagesGudiance and CounsellingPrity Devi100% (2)
- Physical Education Grading Rubic PDFDocument1 pagePhysical Education Grading Rubic PDFJammie Aure EsguerraNo ratings yet
- Understanding Consumer Behaviour: © Macmillan Publishers India Ltd. 1Document12 pagesUnderstanding Consumer Behaviour: © Macmillan Publishers India Ltd. 1KavinNo ratings yet
- Snyder Et Al. 1977 Social Perception and Interpersonal BehaviorDocument11 pagesSnyder Et Al. 1977 Social Perception and Interpersonal BehaviorBelmaDžinićNo ratings yet
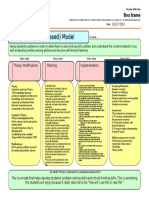
- Problem-Solving Based Model OriginalDocument1 pageProblem-Solving Based Model Originalapi-314418210No ratings yet
- Breaking The Drama TriangleDocument3 pagesBreaking The Drama TriangleSvetlana Radovanovic100% (5)
- Life Skills and Inclusive EducationDocument6 pagesLife Skills and Inclusive EducationAnonymous CwJeBCAXpNo ratings yet
- Abbey Faro RecDocument1 pageAbbey Faro Recapi-407871224No ratings yet
- Own Personal and Professional Development: Prepared by Mohamad Imaduddin Bin Zainal AbidinDocument25 pagesOwn Personal and Professional Development: Prepared by Mohamad Imaduddin Bin Zainal Abidinmasni matNo ratings yet
- Edad 694 SHDocument9 pagesEdad 694 SHapi-508707703No ratings yet
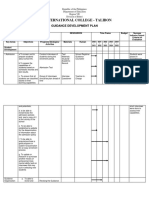
- Bit International College - Talibon: Guidance Development PlanDocument9 pagesBit International College - Talibon: Guidance Development Planjeo nalugonNo ratings yet
- Styles of World's LeadershipDocument22 pagesStyles of World's LeadershipEnah Sazi Ale ArbalNo ratings yet
- Lecture - Applied Social PsychologyDocument81 pagesLecture - Applied Social PsychologyMz_Smikle100% (17)
- Tools in Family Assessment: Ed Marie M. Togonon-Cruz, M.D.,DFM July 16, 2021Document36 pagesTools in Family Assessment: Ed Marie M. Togonon-Cruz, M.D.,DFM July 16, 2021Ed Marie CruzNo ratings yet
- Management Guidelines For Anxiety Disorders in Children and AdolescentsDocument23 pagesManagement Guidelines For Anxiety Disorders in Children and AdolescentsHari HaranNo ratings yet
- Running Head: Cultural Preferences For Luxury Goods 1Document9 pagesRunning Head: Cultural Preferences For Luxury Goods 1Bryan LazaroNo ratings yet
- HUMANITAS Vol. 11-2.131-142 ISSN : 1693-7236 Kualitas Kehidupan Kerja, Kecerdasan Emosi dan Efetivitas Tim Kerja dengan Mediator Komitmen OrganisasiDocument12 pagesHUMANITAS Vol. 11-2.131-142 ISSN : 1693-7236 Kualitas Kehidupan Kerja, Kecerdasan Emosi dan Efetivitas Tim Kerja dengan Mediator Komitmen OrganisasialbertNo ratings yet
- Psychology Notes Revised by Ayesha YounasDocument56 pagesPsychology Notes Revised by Ayesha YounasAyesha100% (1)
- Full Research On MR ChildrenDocument167 pagesFull Research On MR ChildrenDipali kharodeNo ratings yet
- Documentation of Planning Cycle Part 1 N Part BDocument7 pagesDocumentation of Planning Cycle Part 1 N Part BOfficial WorkNo ratings yet
- Chapter Ii KatherenDocument5 pagesChapter Ii KatherenFerdinand MartinezNo ratings yet
- Contoh Kalimat Bahasa InggrisDocument2 pagesContoh Kalimat Bahasa Inggrismike gita rahayuNo ratings yet
- HRM-380-1-Quiz-3-Introduction To Compensation Management-Group-C-ove Kabir Eon-1731923630Document2 pagesHRM-380-1-Quiz-3-Introduction To Compensation Management-Group-C-ove Kabir Eon-1731923630Ove Kabir Eon 1731923100% (1)
- Topic 5 Contingency Leadership TheoriesDocument69 pagesTopic 5 Contingency Leadership Theoriesfariez79No ratings yet
- Studying Spirituality in The Context of Grit and Resilience of College-Going Young AdultsDocument7 pagesStudying Spirituality in The Context of Grit and Resilience of College-Going Young AdultsJannah FielNo ratings yet
- Annotated BibliographyDocument4 pagesAnnotated Bibliographyapi-241310299No ratings yet
- Effects of A Brief Early Start Denver Model (ESDM) - Based Parent Intervention On Toddlers at Risk For Autism Spectrum Disorders A Randomized Controlled TrialDocument14 pagesEffects of A Brief Early Start Denver Model (ESDM) - Based Parent Intervention On Toddlers at Risk For Autism Spectrum Disorders A Randomized Controlled TrialLuis Seixas100% (1)
- 25 Leadership Qualities That Make You a Great LeaderDocument31 pages25 Leadership Qualities That Make You a Great LeaderMarcela Consigo RamosNo ratings yet