You might also like
- Test Bank For Clinical Laboratory Hematology 2nd Edition MckenzieDocument12 pagesTest Bank For Clinical Laboratory Hematology 2nd Edition Mckenzienoumenalskall0wewNo ratings yet
- Dengue NCPDocument3 pagesDengue NCPnj_pink08179456% (9)
- Nursing Care Plan Diabetes Mellitus Type 1Document2 pagesNursing Care Plan Diabetes Mellitus Type 1deric85% (47)
- NCP Risk For Deficient Fluid Volume PotentialDocument4 pagesNCP Risk For Deficient Fluid Volume PotentialArian May Marcos100% (1)
- NCP - Fluid and Electrolyte ImbalanceDocument3 pagesNCP - Fluid and Electrolyte ImbalancePaolo Belleza78% (9)
- NURSING CARE PLAN - Liver CirrhosisDocument2 pagesNURSING CARE PLAN - Liver Cirrhosisderic100% (27)
- 10 Quality Indicators For Blood Bank: Adverse Transfusion Reaction Rate %Document2 pages10 Quality Indicators For Blood Bank: Adverse Transfusion Reaction Rate %Toni StarkNo ratings yet
- Capillary Puncture Equipment and ProcedureDocument3 pagesCapillary Puncture Equipment and ProcedureSieg100% (1)
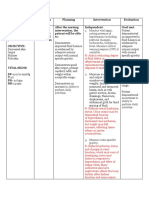
- Cues/Needs Nursing Diagnosis Rationale Goals and Objectives Interventions Rationale Evaluation Subjective Data: IndependentDocument2 pagesCues/Needs Nursing Diagnosis Rationale Goals and Objectives Interventions Rationale Evaluation Subjective Data: IndependentArabelle GONo ratings yet
- Nursing Care PlanDocument3 pagesNursing Care Planmust dietNo ratings yet
- NCP DengueDocument3 pagesNCP DenguejhaninahNo ratings yet
- NCPs Durano Aireen E.Document6 pagesNCPs Durano Aireen E.Doneva Lyn MedinaNo ratings yet
- Ncp.-Fluid Volume DeficitDocument1 pageNcp.-Fluid Volume DeficitAdia Cavrinni De JesusNo ratings yet
- Pedia NCPDocument9 pagesPedia NCPTyn TynNo ratings yet
- NCP GI EditedDocument4 pagesNCP GI EditednicoleNo ratings yet
- NCP CaprichoDocument3 pagesNCP CaprichoElishah CaprichoNo ratings yet
- Dengue NCPDocument3 pagesDengue NCPingridNo ratings yet
- Module 2 1Document3 pagesModule 2 1Lacangan, Thea YvonneNo ratings yet
- NCP Liver CirrhosisDocument2 pagesNCP Liver Cirrhosismarlx5100% (3)
- Assessment Diagnosis Planning Implementation Rationale EvaluationDocument3 pagesAssessment Diagnosis Planning Implementation Rationale EvaluationHanz AlecNo ratings yet
- Nursing Care Plan: Histolytica, ADocument4 pagesNursing Care Plan: Histolytica, AkristennemarieNo ratings yet
- NCP - DM - FatigueDocument12 pagesNCP - DM - FatigueJisel-Apple BulanNo ratings yet
- NCP - AgeDocument5 pagesNCP - Ageunsp3akabl386% (7)
- Assessment/ Cues Nursing Diagnosis Background Knowledge Goal and Objectives Nursing Interventions and Rationale EvaluationDocument6 pagesAssessment/ Cues Nursing Diagnosis Background Knowledge Goal and Objectives Nursing Interventions and Rationale EvaluationimnasNo ratings yet
- Acute Renal Failure Nursing Care PlanDocument4 pagesAcute Renal Failure Nursing Care PlanKrisianne Mae Lorenzo Francisco80% (5)
- NCP Deficient Fluid VolumeDocument5 pagesNCP Deficient Fluid VolumeCHRISTINE GRACE ELLONo ratings yet
- NCP ProperDocument9 pagesNCP Properstephanie eduarteNo ratings yet
- NCP Fluid and Electrolyte ImbalanceDocument3 pagesNCP Fluid and Electrolyte ImbalanceVitha100% (1)
- Gi-Rle - NCP For Deficient Fluid VolumeDocument2 pagesGi-Rle - NCP For Deficient Fluid VolumeEvangeline Villa de Gracia100% (1)
- Cues Nursing Diagnosis Background and Knowledge Goals and Objectives Nursing Intervention and Rationale EvaluationDocument3 pagesCues Nursing Diagnosis Background and Knowledge Goals and Objectives Nursing Intervention and Rationale EvaluationKristiene Kyle AquinoNo ratings yet
- Nursing Care Plan: IndependentDocument2 pagesNursing Care Plan: IndependentAdhaNo ratings yet
- Nursing Care Plan TemplateDocument3 pagesNursing Care Plan TemplateTricia LiporadaNo ratings yet
- Nursing Care Plan Patient's Name: Age: Sex: Address:: Nursing-Notes/communicable - Diseases - Notes/amoebiasisDocument4 pagesNursing Care Plan Patient's Name: Age: Sex: Address:: Nursing-Notes/communicable - Diseases - Notes/amoebiasisGILIANNE MARIE JIMENEANo ratings yet
- Student Nurses' Community: NURSING CARE PLAN AppendicitisDocument2 pagesStudent Nurses' Community: NURSING CARE PLAN AppendicitisJamaica Leslie NovenoNo ratings yet
- Nursing Care Plan For DM PatientDocument10 pagesNursing Care Plan For DM PatientRainier Rhett Concha100% (5)
- DM NCP - Trixia U. Almendral GRP 6Document3 pagesDM NCP - Trixia U. Almendral GRP 6Trixia AlmendralNo ratings yet
- Global City Innovative CollegeDocument3 pagesGlobal City Innovative CollegemadypadNo ratings yet
- NCP 3rd ROTATIONDocument17 pagesNCP 3rd ROTATIONMarie Ashley CasiaNo ratings yet
- Fluid Volume Deficit Nursing Care PlanDocument4 pagesFluid Volume Deficit Nursing Care PlanTipey SegismundoNo ratings yet
- Renal Concept MapDocument1 pageRenal Concept MapShaira Ann CalambaNo ratings yet
- Assessment Diagnosis Planning Intervention-Rationale Evaluation Fluid Volume Excess Related ToDocument3 pagesAssessment Diagnosis Planning Intervention-Rationale Evaluation Fluid Volume Excess Related ToJen BallesterosNo ratings yet
- Emilio Aguinaldo College: School of NursingDocument2 pagesEmilio Aguinaldo College: School of NursingdaliaNo ratings yet
- NCP For Dehydration 1Document3 pagesNCP For Dehydration 1Khalid KhanNo ratings yet
- Chronic Renal Failure Nursing Care PlanDocument6 pagesChronic Renal Failure Nursing Care PlanRuva Oscass JimmyNo ratings yet
- NCP HmoleDocument5 pagesNCP HmolemeriiNo ratings yet
- Choler A: Prepared By: Angelou Mortos John Radley SantosDocument11 pagesCholer A: Prepared By: Angelou Mortos John Radley SantosAdhaNo ratings yet
- Nursing Diagnosis 2Document3 pagesNursing Diagnosis 2anon_168410816No ratings yet
- Deficient Fluid Volume (Vanene)Document7 pagesDeficient Fluid Volume (Vanene)jajalerNo ratings yet
- Peritonitis NCPDocument3 pagesPeritonitis NCPANNA V. LARITANo ratings yet
- NCP and Drug Study (Isph-Gs Nursery)Document4 pagesNCP and Drug Study (Isph-Gs Nursery)Cristyl Shine BariaoNo ratings yet
- Fluid Volume Defict Ms. HicksDocument8 pagesFluid Volume Defict Ms. HicksShenna RegaspiNo ratings yet
- NCPDocument9 pagesNCPYesha Mae MartinNo ratings yet
- Nursing Care PlanDocument11 pagesNursing Care PlanKirstin del CarmenNo ratings yet
- Date Cues Nursing Diagnosis Scientific Basis Goal of Care Nursing Intervention Rationale EvaluationDocument2 pagesDate Cues Nursing Diagnosis Scientific Basis Goal of Care Nursing Intervention Rationale Evaluationkimglaidyl bontuyanNo ratings yet
- Post Partum Hemorrhage Nursing Care Plan PDFDocument2 pagesPost Partum Hemorrhage Nursing Care Plan PDFA sison100% (1)
- Final NCP1 2Document2 pagesFinal NCP1 2hahahahaaaaaaaNo ratings yet
- Assessment Diagnosis Planning Implementation Evaluation Case: Amoebiasis Subjective:" Madalas Po AkongDocument47 pagesAssessment Diagnosis Planning Implementation Evaluation Case: Amoebiasis Subjective:" Madalas Po AkongNylia AtibiNo ratings yet
- Nursing Care Plan For Acute Gastrointestinal HemorrhageDocument2 pagesNursing Care Plan For Acute Gastrointestinal HemorrhageMia PascualNo ratings yet
- ROSABIA, Micaela Pauline J. .-BSN-2A-ISDH-GS-NURSERY-NCPDocument6 pagesROSABIA, Micaela Pauline J. .-BSN-2A-ISDH-GS-NURSERY-NCPkimberly quitonNo ratings yet
- NCP With DsDocument11 pagesNCP With DsMissDyYournurseNo ratings yet
- Assessment Inference Diagnosis Planning Intervention Rationale EvaluationDocument3 pagesAssessment Inference Diagnosis Planning Intervention Rationale EvaluationSteffi Blair OngNo ratings yet
- Ascites, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandAscites, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- In Haematology - Diploma LevelDocument16 pagesIn Haematology - Diploma LevelSAMMYNo ratings yet
- ABO Blood GroupDocument41 pagesABO Blood GroupSafura IjazNo ratings yet
- Scrap Alkes FIXDocument18 pagesScrap Alkes FIXrosidNo ratings yet
- Explanations of Case Studies and ScenariosDocument10 pagesExplanations of Case Studies and ScenariosMa. Ferimi Gleam BajadoNo ratings yet
- Lab Values 1Document30 pagesLab Values 1Ezekiel John GarciaNo ratings yet
- Hematologic System, Oncologic Disorders & Anemias: DR Ibrahreem Bashayreh, RN, PHDDocument68 pagesHematologic System, Oncologic Disorders & Anemias: DR Ibrahreem Bashayreh, RN, PHDYA HONo ratings yet
- ABO Subgroups and Bombay GroupDocument15 pagesABO Subgroups and Bombay GrouphamaadaNo ratings yet
- What Is-Thrombocythemia and ThrombocytosisDocument4 pagesWhat Is-Thrombocythemia and ThrombocytosisFred C. MirandaNo ratings yet
- Component TherapyDocument18 pagesComponent TherapyjosereyescclNo ratings yet
- Common Medical AbbreviationsDocument3 pagesCommon Medical Abbreviationschester De GuzmanNo ratings yet
- 9 Th. Lec. Lewis Blood Group SystemDocument11 pages9 Th. Lec. Lewis Blood Group Systemda202263357026No ratings yet
- Cara Kerja Kimia Klinik SpektrofotometriDocument1 pageCara Kerja Kimia Klinik SpektrofotometrilabrsiabcmNo ratings yet
- Asa Qurrotul' Ain KtiDocument64 pagesAsa Qurrotul' Ain KtiAnangNo ratings yet
- HEMA LAB Reticulocyte Study ESR OFT RBC CountDocument17 pagesHEMA LAB Reticulocyte Study ESR OFT RBC CountJam RamosNo ratings yet
- HemorrhageDocument13 pagesHemorrhagekins.bhojaniNo ratings yet
- Blood Typing Lab Activity FinalDocument3 pagesBlood Typing Lab Activity FinalMrRightNo ratings yet
- 13 HemostasisDocument38 pages13 HemostasissiratelNo ratings yet
- Coagulation TestsDocument25 pagesCoagulation Testsdave_1128No ratings yet
- Booklet 2 Donador de SangreDocument16 pagesBooklet 2 Donador de SangreKatherine QuinteroNo ratings yet
- Medical Care of Pregnant Women With EPH Gestosis: October 2013Document16 pagesMedical Care of Pregnant Women With EPH Gestosis: October 2013Lara GadžunNo ratings yet
- Blood Group O Convalescent Plasma Donations HaveDocument5 pagesBlood Group O Convalescent Plasma Donations HaveANANo ratings yet
- 3 Reagent For Hemoglobin DeterminationDocument4 pages3 Reagent For Hemoglobin DeterminationEricka GenoveNo ratings yet
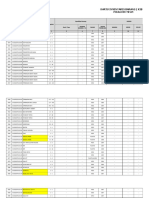
- Revised Daily Inventory FormDocument1 pageRevised Daily Inventory FormMary Terybel Lasay-astilloNo ratings yet
- Hole's Human Anatomy & Physiology: Eighth EditionDocument25 pagesHole's Human Anatomy & Physiology: Eighth Editionhanif amirusdiNo ratings yet
- Hema2 Lec PrefinalDocument9 pagesHema2 Lec Prefinallai cruzNo ratings yet
- Platelet and Plasma Transfusion Policy. in Blood Transfusion Guideline PDFDocument13 pagesPlatelet and Plasma Transfusion Policy. in Blood Transfusion Guideline PDFbencleeseNo ratings yet
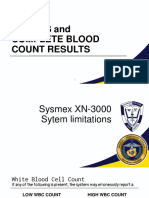
- Errors and The CBC Result 2.0Document43 pagesErrors and The CBC Result 2.0Ella OrtegaNo ratings yet