You might also like
- APPLICATION OF RADIOBIOLOGY PRINCIPLES IN RADIOTHERAPYDocument61 pagesAPPLICATION OF RADIOBIOLOGY PRINCIPLES IN RADIOTHERAPYnilesh kumarNo ratings yet
- An Evidence-Based Approach to the Management of Nasopharyngeal Cancer: From Basic Science to Clinical Presentation and TreatmentFrom EverandAn Evidence-Based Approach to the Management of Nasopharyngeal Cancer: From Basic Science to Clinical Presentation and TreatmentBaharudin AbdullahNo ratings yet
- Optimize Radiotherapy for Head and Neck CancersDocument90 pagesOptimize Radiotherapy for Head and Neck Cancersyunia chairunnisaNo ratings yet
- Atlas of Hybrid Imaging Sectional Anatomy for PET/CT, PET/MRI and SPECT/CT Vol. 2: Thorax Abdomen and Pelvis: Sectional Anatomy for PET/CT, PET/MRI and SPECT/CTFrom EverandAtlas of Hybrid Imaging Sectional Anatomy for PET/CT, PET/MRI and SPECT/CT Vol. 2: Thorax Abdomen and Pelvis: Sectional Anatomy for PET/CT, PET/MRI and SPECT/CTNo ratings yet
- Women's Imaging: MRI with Multimodality CorrelationFrom EverandWomen's Imaging: MRI with Multimodality CorrelationMichele A. BrownRating: 5 out of 5 stars5/5 (1)
- Head and Neck Cancer Care in a Pandemic: Prioritizing Safe CareFrom EverandHead and Neck Cancer Care in a Pandemic: Prioritizing Safe CareNo ratings yet
- Clinical PET/MRIFrom EverandClinical PET/MRIOnofrio Antonio CatalanoNo ratings yet
- Head and Neck Cancer Radiotherapy Guidelines 2019 - DAHANCADocument45 pagesHead and Neck Cancer Radiotherapy Guidelines 2019 - DAHANCAMilda InayahNo ratings yet
- Problem Solving in Oncology 1st 2008Document26 pagesProblem Solving in Oncology 1st 2008Anirban Halder100% (1)
- Pituitary Adenoma FinalDocument44 pagesPituitary Adenoma FinalTuhinaRaj100% (1)
- Surgical Incisions Balancing Surgical and Cosmetic Outcomes in Head and Neck OncosurgeryDocument4 pagesSurgical Incisions Balancing Surgical and Cosmetic Outcomes in Head and Neck OncosurgeryDwarika Prasad BajgaiNo ratings yet
- Principles RadiotherapyDocument71 pagesPrinciples RadiotherapyHasan AlomariNo ratings yet
- Atlas of Hybrid Imaging Sectional Anatomy for PET/CT, PET/MRI and SPECT/CT Vol. 1: Brain and Neck: Sectional Anatomy for PET/CT, PET/MRI and SPECT/CTFrom EverandAtlas of Hybrid Imaging Sectional Anatomy for PET/CT, PET/MRI and SPECT/CT Vol. 1: Brain and Neck: Sectional Anatomy for PET/CT, PET/MRI and SPECT/CTNo ratings yet
- Rtog 0813 Marina CousinsDocument22 pagesRtog 0813 Marina Cousinsapi-426094285No ratings yet
- Diseases of the Nose, Throat and Ear: For Practitioners and StudentsFrom EverandDiseases of the Nose, Throat and Ear: For Practitioners and StudentsA. Logan TurnerNo ratings yet
- RF Coils for MRIFrom EverandRF Coils for MRIJ. Thomas VaughanNo ratings yet
- Snoring, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandSnoring, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Topics in Radiation Dosimetry: Radiation Dosimetry, Vol. 1From EverandTopics in Radiation Dosimetry: Radiation Dosimetry, Vol. 1Frank H. AttixNo ratings yet
- Three-Dimensional Conformal Radiation Therapy (3DCRT) For Prostate CancerDocument34 pagesThree-Dimensional Conformal Radiation Therapy (3DCRT) For Prostate CancerMuhammad Safwan Ahmad FadzilNo ratings yet
- Sources, Fields, Measurements, and Applications: Radiation Dosimetry, Vol. 3From EverandSources, Fields, Measurements, and Applications: Radiation Dosimetry, Vol. 3Frank H. AttixNo ratings yet
- 6516516584123XDocument144 pages6516516584123XJohn M. HemsworthNo ratings yet
- The 4th Edition of The Head and Neck WHO Blue BookDocument11 pagesThe 4th Edition of The Head and Neck WHO Blue Bookjarzcorpify100% (1)
- HoskinsDocument558 pagesHoskinsSA NodeNo ratings yet
- Cholesteatoma, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCholesteatoma, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Proton Therapy for Cancer Treatment Using High-Energy ProtonsDocument48 pagesProton Therapy for Cancer Treatment Using High-Energy ProtonsSUBHA100% (1)
- Radiation Oncology Management Decisions 2002 (Perez)Document773 pagesRadiation Oncology Management Decisions 2002 (Perez)abdullmajeed50% (2)
- Cleft Lip and Palate Management: A Comprehensive AtlasFrom EverandCleft Lip and Palate Management: A Comprehensive AtlasRicardo D. BennunNo ratings yet
- Brachytherapy in Cancer CervixDocument65 pagesBrachytherapy in Cancer CervixSatyesh NadellaNo ratings yet
- Prostate Radiotherapy - Current Standards and Future DirectionsDocument40 pagesProstate Radiotherapy - Current Standards and Future Directionsvikram_bansal84No ratings yet
- Radiation Oncology: DR - Durgesh Mishra Dy - Cmo, MJPJAY, MahDocument13 pagesRadiation Oncology: DR - Durgesh Mishra Dy - Cmo, MJPJAY, MahKASATSANo ratings yet
- Atlas of Topographical and Pathotopographical Anatomy of the Head and NeckFrom EverandAtlas of Topographical and Pathotopographical Anatomy of the Head and NeckNo ratings yet
- Eustachian Tube: Structure, Function, and Role in Middle-Ear Disease, 2eFrom EverandEustachian Tube: Structure, Function, and Role in Middle-Ear Disease, 2eNo ratings yet
- Postlaryngectomy voice rehabilitation with voice prosthesesFrom EverandPostlaryngectomy voice rehabilitation with voice prosthesesNo ratings yet
- Bailey's 5th Ed (2014) - Ossicular RekonstruksiDocument12 pagesBailey's 5th Ed (2014) - Ossicular RekonstruksiMei Risanti SiraitNo ratings yet
- Paranasal Sinuses: Anatomy and FunctionDocument49 pagesParanasal Sinuses: Anatomy and FunctionYoel Lia NieNo ratings yet
- IMRT Basics: R. Alfredo C. Siochi, Ph.D. Juan Carlos Celi, PH.DDocument3 pagesIMRT Basics: R. Alfredo C. Siochi, Ph.D. Juan Carlos Celi, PH.DSantanu SamantaNo ratings yet
- Advances in Radiation Biology V14: Relative Radiation Sensitivities of Human Organ Systems. Part IIFrom EverandAdvances in Radiation Biology V14: Relative Radiation Sensitivities of Human Organ Systems. Part IIJohn LettNo ratings yet
- Step-By-Step Approach To Endoscopic Cadaveric DissectionDocument205 pagesStep-By-Step Approach To Endoscopic Cadaveric DissectionJavier Gutiérrez CastilloNo ratings yet
- MR Af ProstataDocument8 pagesMR Af ProstataKamran AfzalNo ratings yet
- Maxillary ArteryDocument30 pagesMaxillary ArteryMeriam AntonyNo ratings yet
- Image Guided Radiotherapy Technique - IGRTDocument13 pagesImage Guided Radiotherapy Technique - IGRTbadusha vpNo ratings yet
- Protocol 4 SlicesDocument143 pagesProtocol 4 SlicessaeedNo ratings yet
- Chemotherapy in Ent My PTDocument25 pagesChemotherapy in Ent My PTRajarshi Sannigrahi0% (1)
- Open SeptorhinoplastyDocument6 pagesOpen SeptorhinoplastybarbiemeNo ratings yet
- Thesis Setup Error PelvicDocument43 pagesThesis Setup Error PelvichandiaviNo ratings yet
- Logan Turner's Diseases of the Nose, Throat and EarFrom EverandLogan Turner's Diseases of the Nose, Throat and EarRating: 4 out of 5 stars4/5 (2)
- CholesteatomaDocument29 pagesCholesteatomawhitelotusoo7No ratings yet
- Prodige 23Document14 pagesProdige 23josebaNo ratings yet
- The Lecture: "Tumours of The Mammary Gland."Document21 pagesThe Lecture: "Tumours of The Mammary Gland."top theNo ratings yet
- Paranasal Sinus (Repaired) EntDocument48 pagesParanasal Sinus (Repaired) EntDr-Firas Nayf Al-ThawabiaNo ratings yet
- Lazer in OtolaryngologyDocument2 pagesLazer in OtolaryngologyDr-Firas Nayf Al-ThawabiaNo ratings yet
- The Most Common (Autosaved) in OtolaryngologyDocument15 pagesThe Most Common (Autosaved) in OtolaryngologyDr-Firas Nayf Al-ThawabiaNo ratings yet
- Tracheostomy EmergenciesDocument32 pagesTracheostomy EmergenciesDr-Firas Nayf Al-Thawabia100% (1)
- Facial Nerve Surgical ApproachesDocument4 pagesFacial Nerve Surgical ApproachesDr-Firas Nayf Al-ThawabiaNo ratings yet
- CT Imaging of The Temporal Bone: An Anatomical Review With Illustrative Cases of CholesteatomasDocument116 pagesCT Imaging of The Temporal Bone: An Anatomical Review With Illustrative Cases of CholesteatomasDr-Firas Nayf Al-Thawabia100% (1)
- AJCC Cancer Staging Form Supplement PDFDocument520 pagesAJCC Cancer Staging Form Supplement PDFopi akbarNo ratings yet
- Neonatal Facial Nerve Palsy PDFDocument5 pagesNeonatal Facial Nerve Palsy PDFDr-Firas Nayf Al-ThawabiaNo ratings yet
- Facial Nerve Palsy in Children Causes and TreatmentDocument5 pagesFacial Nerve Palsy in Children Causes and TreatmentDr-Firas Nayf Al-ThawabiaNo ratings yet
- Ramsay Hunt Syndrome EntDocument3 pagesRamsay Hunt Syndrome EntDr-Firas Nayf Al-Thawabia100% (1)
- Zaghal 2014 - Anatomy of Facial Nerve and Tympanic AnnulusDocument5 pagesZaghal 2014 - Anatomy of Facial Nerve and Tympanic AnnulusDr-Firas Nayf Al-ThawabiaNo ratings yet
- Temporalbone 151227031114Document350 pagesTemporalbone 151227031114Dr-Firas Nayf Al-ThawabiaNo ratings yet
- Facial Nerve Surgical ApproachesDocument4 pagesFacial Nerve Surgical ApproachesDr-Firas Nayf Al-ThawabiaNo ratings yet
- Juvenile Nasopharyngial AngiofibromaDocument8 pagesJuvenile Nasopharyngial AngiofibromaDr-Firas Nayf Al-ThawabiaNo ratings yet
- CSF RhinorrheaDocument10 pagesCSF RhinorrheaDr-Firas Nayf Al-ThawabiaNo ratings yet
- Facial Nerve Trauma: Maisa AlsmadiDocument28 pagesFacial Nerve Trauma: Maisa AlsmadiDr-Firas Nayf Al-ThawabiaNo ratings yet
- Zaghal 2014 - Anatomy of Facial Nerve and Tympanic AnnulusDocument5 pagesZaghal 2014 - Anatomy of Facial Nerve and Tympanic AnnulusDr-Firas Nayf Al-ThawabiaNo ratings yet
- HRCT Temporal Bone AnatomyDocument66 pagesHRCT Temporal Bone AnatomyDr-Firas Nayf Al-Thawabia100% (1)
- Traumatic Facial Nerve PalsyDocument12 pagesTraumatic Facial Nerve PalsyDr-Firas Nayf Al-ThawabiaNo ratings yet
- Trauma: Accidental Temporal Bone Fractures Classification SchemesDocument12 pagesTrauma: Accidental Temporal Bone Fractures Classification SchemesDr-Firas Nayf Al-ThawabiaNo ratings yet
- Allergic Rhinitiseditedppt2614Document43 pagesAllergic Rhinitiseditedppt2614Dr-Firas Nayf Al-ThawabiaNo ratings yet
- Intercollegiate Specialty Exam in ENT RegulationsDocument4 pagesIntercollegiate Specialty Exam in ENT RegulationsDr-Firas Nayf Al-ThawabiaNo ratings yet
- MCQ S For StudentsDocument58 pagesMCQ S For StudentsJohn M. Hemsworth100% (2)
- Bell's PalsyDocument9 pagesBell's PalsyDr-Firas Nayf Al-ThawabiaNo ratings yet
- Allergic RhinitisDocument38 pagesAllergic RhinitisDr-Firas Nayf Al-ThawabiaNo ratings yet
- Allergicrhinitis 140911185124 Phpapp01Document24 pagesAllergicrhinitis 140911185124 Phpapp01Dr-Firas Nayf Al-ThawabiaNo ratings yet
- 105.fullcong NasalDocument12 pages105.fullcong NasalDr-Firas Nayf Al-ThawabiaNo ratings yet
- Pedi Nasal Mass Slides 060607Document54 pagesPedi Nasal Mass Slides 060607Dr-Firas Nayf Al-ThawabiaNo ratings yet
- Allergic Rhinitis: S PandeyDocument37 pagesAllergic Rhinitis: S PandeyDr-Firas Nayf Al-ThawabiaNo ratings yet
- (Culture and History of The Ancient Near East 65) Leslie Anne Warden - Pottery and Economy in Old Kingdom Egypt-Brill Academic Publishers (2014)Document343 pages(Culture and History of The Ancient Near East 65) Leslie Anne Warden - Pottery and Economy in Old Kingdom Egypt-Brill Academic Publishers (2014)HugoBotello100% (1)
- IM PS Fashion-Business-Digital-Communication-And-Media 3Y Course Pathway MI 04Document7 pagesIM PS Fashion-Business-Digital-Communication-And-Media 3Y Course Pathway MI 04oliwia bujalskaNo ratings yet
- Value YourselfDocument7 pagesValue YourselfTalha KhalidNo ratings yet
- What Is Mean?: Extrapolation InterpolationDocument2 pagesWhat Is Mean?: Extrapolation InterpolationVinod SharmaNo ratings yet
- Javelin Mobility Ability 2.0 GuideDocument36 pagesJavelin Mobility Ability 2.0 Guideroham25156No ratings yet
- S-H Polarimeter Polartronic-532 Eng - 062015 PDFDocument2 pagesS-H Polarimeter Polartronic-532 Eng - 062015 PDFSuresh KumarNo ratings yet
- 2020 Exam-Sample-Questions-Computer-ScienceDocument8 pages2020 Exam-Sample-Questions-Computer-ScienceNesrine LaradjiNo ratings yet
- Pcit Brochure TemplateDocument2 pagesPcit Brochure Templateapi-370829251No ratings yet
- Acrogym: by Ahana AnandDocument9 pagesAcrogym: by Ahana AnandAhana AnandNo ratings yet
- Labconco-3905503 Rev e Purifier Hepa Filtered and Class I Filtered Enclosures User ManualDocument77 pagesLabconco-3905503 Rev e Purifier Hepa Filtered and Class I Filtered Enclosures User ManualCalixto GrajalesNo ratings yet
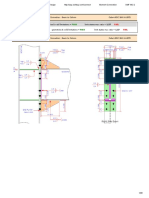
- Bridge Manual Retaining Walls - Section 3.62 Page 3.2-2Document1 pageBridge Manual Retaining Walls - Section 3.62 Page 3.2-2lomoscribdNo ratings yet
- Cultures of Learning: Language Classrooms in China: Martin Cortazzi Lixian JinDocument54 pagesCultures of Learning: Language Classrooms in China: Martin Cortazzi Lixian JinyhoulhandhariNo ratings yet
- MsdsDocument6 pagesMsdsGis GeorgeNo ratings yet
- Junguian PsychotherapyDocument194 pagesJunguian PsychotherapyRene Galvan Heim100% (13)
- Pediatrics Study ScheduleDocument2 pagesPediatrics Study ScheduleNatnaelNo ratings yet
- Project management software enables collaborationDocument4 pagesProject management software enables collaborationNoman AliNo ratings yet
- Result Summary - Overall: Moment Connection - Beam To Column Code AISC 360-16 LRFDDocument29 pagesResult Summary - Overall: Moment Connection - Beam To Column Code AISC 360-16 LRFDYash Suthar100% (2)
- Albert Einstein - Wikipedia, The Free EncyclopediaDocument34 pagesAlbert Einstein - Wikipedia, The Free EncyclopediaalhanunNo ratings yet
- Modigliani MillerDocument12 pagesModigliani MillerAlvaro CamañoNo ratings yet
- Families of Carbon Compounds: Functional Groups, Intermolecular Forces, & Infrared (IR) SpectrosDocument79 pagesFamilies of Carbon Compounds: Functional Groups, Intermolecular Forces, & Infrared (IR) SpectrosRuryKharismaMuzaqieNo ratings yet
- Fundamentals of Computer Hardware NotesDocument7 pagesFundamentals of Computer Hardware NotesSreemoyee RoyNo ratings yet
- German Companies in RwandaDocument6 pagesGerman Companies in RwandaTabitha KaraniNo ratings yet
- Carbon Disulfide: Hazard SummaryDocument5 pagesCarbon Disulfide: Hazard SummaryAlyssa ZerlinaNo ratings yet
- THC124 - Lesson 1. The Impacts of TourismDocument50 pagesTHC124 - Lesson 1. The Impacts of TourismAnne Letrondo Bajarias100% (1)
- Bharathidasan University UG/PG Exam ApplicationDocument2 pagesBharathidasan University UG/PG Exam ApplicationOppili yappanNo ratings yet
- Vici Line Card 2015Document14 pagesVici Line Card 2015Argel Linard Francisco MabagaNo ratings yet
- Neolithic Farming Villages Jericho and Catal HuyukDocument1 pageNeolithic Farming Villages Jericho and Catal HuyukPream BoleoNo ratings yet
- Method Overloading in JavaDocument6 pagesMethod Overloading in JavaPrerna GourNo ratings yet
- LP Science WeatheringDocument4 pagesLP Science WeatheringHazel L Ibarra100% (1)
- Kiro Urdin BookDocument189 pagesKiro Urdin BookDane BrdarskiNo ratings yet