You might also like
- Management of Hereditary Colorectal Cancer: A Multidisciplinary ApproachFrom EverandManagement of Hereditary Colorectal Cancer: A Multidisciplinary ApproachJose G. GuillemNo ratings yet
- Survival of Children With A Wilms Tumor in Blantyre, Malawi: Pediatric Hematology and OncologyDocument8 pagesSurvival of Children With A Wilms Tumor in Blantyre, Malawi: Pediatric Hematology and OncologyLady HeruNo ratings yet
- Unintended Pregnancy Among HIV PDFDocument11 pagesUnintended Pregnancy Among HIV PDFTitin JuherniNo ratings yet
- 05-Long-Term Neurodevelopmental Outcome After Prenatal Exposure To Maternal Hematological MalignaDocument13 pages05-Long-Term Neurodevelopmental Outcome After Prenatal Exposure To Maternal Hematological MalignaInggita Adinda PutriNo ratings yet
- 1472 6874 10 8 PDFDocument7 pages1472 6874 10 8 PDFhirsi200518No ratings yet
- Cervical Cancer Prevention in Transgender Men: A Review: Version of Record Doi: 10.1111/1471-0528.16503Document13 pagesCervical Cancer Prevention in Transgender Men: A Review: Version of Record Doi: 10.1111/1471-0528.16503tavo823No ratings yet
- Acta Obstet Gynecol Scand - 2019 - Poirot - Ovarian Tissue Cryopreservation For Fertility Preservation in 418 Girls andDocument8 pagesActa Obstet Gynecol Scand - 2019 - Poirot - Ovarian Tissue Cryopreservation For Fertility Preservation in 418 Girls andLucas Monteiro LopesNo ratings yet
- Patient Reported BarriesDocument14 pagesPatient Reported Barriesdani catriaNo ratings yet
- Health&Clinical ManagementDocument125 pagesHealth&Clinical ManagementAnjum100% (1)
- New Microsoft Office Word DocumentDocument11 pagesNew Microsoft Office Word DocumentMihaela AndreiNo ratings yet
- Evaluation of Male Partner Participation in Prevention of Mother To Child Transmission of HIVAIDs at Hoima Referral HospitalDocument14 pagesEvaluation of Male Partner Participation in Prevention of Mother To Child Transmission of HIVAIDs at Hoima Referral HospitalKIU PUBLICATION AND EXTENSIONNo ratings yet
- ResearchDocument11 pagesResearchPaulNo ratings yet
- ThesisDocument5 pagesThesisJiehainie IragNo ratings yet
- Progestogen TreatmentDocument6 pagesProgestogen TreatmentIndah HaneNo ratings yet
- Anemia in Pregnancy in Malaysia: A Cross-Sectional Survey: Original ArticleDocument10 pagesAnemia in Pregnancy in Malaysia: A Cross-Sectional Survey: Original ArticleThomson AffendyNo ratings yet
- Effective Screening12Document9 pagesEffective Screening12ponekNo ratings yet
- The Severity of Abortion in MalawiDocument5 pagesThe Severity of Abortion in MalawiSaidi EdwardNo ratings yet
- Knowledge Attitude and Practice of ContraceptiveDocument5 pagesKnowledge Attitude and Practice of ContraceptiveSam AdeNo ratings yet
- Sickle Cell ServicesDocument3 pagesSickle Cell Servicesstephen X-SILVERNo ratings yet
- Childhood Cancer Literature ReviewDocument4 pagesChildhood Cancer Literature Reviewafmzjbxmbfpoox100% (1)
- Epidural HematomaDocument88 pagesEpidural HematomaRyanAgootNo ratings yet
- Challenges and Outcome of Wilms' Tumour Management in A Resource-Constrained SettingDocument3 pagesChallenges and Outcome of Wilms' Tumour Management in A Resource-Constrained Settingcallisto3487No ratings yet
- 1 SMDocument5 pages1 SMali syahbanaNo ratings yet
- Intl J Gynecology Obste - 2021 - WilailakDocument5 pagesIntl J Gynecology Obste - 2021 - WilailakKalaivathanan VathananNo ratings yet
- Trends and Determinants of Maternal Mortality in Mizan-Tepi University Teaching and Bonga General Hospital From 2011 - 2015: A Case Control StudyDocument8 pagesTrends and Determinants of Maternal Mortality in Mizan-Tepi University Teaching and Bonga General Hospital From 2011 - 2015: A Case Control StudyTegenne LegesseNo ratings yet
- Prospects and Potential For Expanding Women's Oncofertility Options - Gabriella TranDocument18 pagesProspects and Potential For Expanding Women's Oncofertility Options - Gabriella TrannurjNo ratings yet
- Anaemia in Pregnancy Malaysia, APJCN2006 PDFDocument10 pagesAnaemia in Pregnancy Malaysia, APJCN2006 PDFAkhmal SidekNo ratings yet
- Clinico-Pathological Features of Breast Cancer in PakistanDocument10 pagesClinico-Pathological Features of Breast Cancer in PakistanMurk NiazNo ratings yet
- Research: Knowledge, Attitudes, Beliefs, Behaviour and Breast Cancer Screening Practices in Ghana, West AfricaDocument10 pagesResearch: Knowledge, Attitudes, Beliefs, Behaviour and Breast Cancer Screening Practices in Ghana, West AfricaSaheed AbdulkarimNo ratings yet
- The Heterogeneity of Global Pediatric Surgery: Defining Needs and Opportunities Around The WorldDocument12 pagesThe Heterogeneity of Global Pediatric Surgery: Defining Needs and Opportunities Around The WorldAndi.Roem_97No ratings yet
- Factors Influencing Utilization of Prevention of Mother To Child Transmission (PMTCT) Services Among Pregnant Women Attending Ante-Natal ClinicDocument6 pagesFactors Influencing Utilization of Prevention of Mother To Child Transmission (PMTCT) Services Among Pregnant Women Attending Ante-Natal ClinicIPROJECCT100% (1)
- 7a Fee ARTDocument12 pages7a Fee ARTVinod GaurNo ratings yet
- JWH 2006 0295 LowlinkDocument7 pagesJWH 2006 0295 LowlinkRiskhan VirniaNo ratings yet
- Factors Associated With Neonatal Near-Miss in Selected Hospitals of Gamo and Gofa Zones, Southern Ethiopia: Nested Case-Control StudyDocument8 pagesFactors Associated With Neonatal Near-Miss in Selected Hospitals of Gamo and Gofa Zones, Southern Ethiopia: Nested Case-Control StudyringgoNo ratings yet
- A Review On Cervical Cancer VaccinationDocument3 pagesA Review On Cervical Cancer VaccinationKIU PUBLICATION AND EXTENSIONNo ratings yet
- 42B169F57392Document6 pages42B169F57392denekeNo ratings yet
- Artikel Insidence and Survival 2015Document4 pagesArtikel Insidence and Survival 2015rianarahmadhanyNo ratings yet
- 1.fp JurnalDocument14 pages1.fp Jurnal13 NOR HAZALINDA BINTI MUHAMADNo ratings yet
- Pendarahan PostpartumDocument8 pagesPendarahan PostpartumsulviNo ratings yet
- Jurnal ColostomyDocument8 pagesJurnal ColostomyVerticha IndahmutNo ratings yet
- Utilization and Effect of Traditional Birth Attendants Among The Pregnant Women in Kahoora Division Hoima DistrictDocument13 pagesUtilization and Effect of Traditional Birth Attendants Among The Pregnant Women in Kahoora Division Hoima DistrictKIU PUBLICATION AND EXTENSIONNo ratings yet
- Factors Associated With Postpartum Hemorrhage Maternal Death in Referral Hospitals in Senegal and Mali: A Cross-Sectional Epidemiological SurveyDocument9 pagesFactors Associated With Postpartum Hemorrhage Maternal Death in Referral Hospitals in Senegal and Mali: A Cross-Sectional Epidemiological SurveyAprina WulandariNo ratings yet
- Integration of Postpartum Healthcare Services ForDocument31 pagesIntegration of Postpartum Healthcare Services ForYulian elleNo ratings yet
- The Magnitude of Abortion Complications in KenyaDocument7 pagesThe Magnitude of Abortion Complications in KenyaNaserian SalvyNo ratings yet
- Use of Complementary and Alternative Medicine in Healthy Children and Children With Chronic Medical Conditions in GermanyDocument10 pagesUse of Complementary and Alternative Medicine in Healthy Children and Children With Chronic Medical Conditions in GermanyPaul NguyenNo ratings yet
- Winer2016 PDFDocument8 pagesWiner2016 PDFAlex AdamiteiNo ratings yet
- Keperawatan Menjelang Ajal Dan PaliatifDocument15 pagesKeperawatan Menjelang Ajal Dan PaliatifLaiLa CiracesiliakencanaNo ratings yet
- Research ArticleDocument7 pagesResearch ArticleViki AmaliaNo ratings yet
- Research ArticleDocument12 pagesResearch Articlelina ukagoNo ratings yet
- HPV Type Distribution in Invasive Cervical Cancer and High-Grade Cervical Intraepithelial Neoplasia AcDocument9 pagesHPV Type Distribution in Invasive Cervical Cancer and High-Grade Cervical Intraepithelial Neoplasia AcFeli FelNo ratings yet
- Delays in Receiving Obstetric Care and Poor Maternal Outcomes: Results From A National Multicentre Cross-Sectional StudyDocument15 pagesDelays in Receiving Obstetric Care and Poor Maternal Outcomes: Results From A National Multicentre Cross-Sectional Studykaren paredes rojasNo ratings yet
- Why Caretakers Bypass Primary Health Care Facilities For Child Care - A Case From Rural TanzaniaDocument10 pagesWhy Caretakers Bypass Primary Health Care Facilities For Child Care - A Case From Rural TanzaniajlventiganNo ratings yet
- ArticleText 78614 1 10 20191030Document7 pagesArticleText 78614 1 10 20191030Melody CyyNo ratings yet
- Guideline Implementation For Breast Healthcare in Low-Income and Middle-Income CountriesDocument23 pagesGuideline Implementation For Breast Healthcare in Low-Income and Middle-Income Countriesrubensosa16No ratings yet
- Breast Cancer Guidelines OverviewDocument23 pagesBreast Cancer Guidelines OverviewRodney MatthewsNo ratings yet
- Moving Beyond Disrespect and Abuse Addressing The Structural Dimensions of Obstetric VioleDocument10 pagesMoving Beyond Disrespect and Abuse Addressing The Structural Dimensions of Obstetric VioleMaryNo ratings yet
- Cervical Cancer in The Pregnant PopulationDocument15 pagesCervical Cancer in The Pregnant PopulationLohayne ReisNo ratings yet
- Manchester Experience 2021Document10 pagesManchester Experience 2021Sara HossamNo ratings yet
- 265 Full PDFDocument8 pages265 Full PDFNurul Rezki Fitriani AzisNo ratings yet
- Breast Cancer JournalDocument14 pagesBreast Cancer JournalYASSER ALATAWINo ratings yet
- Psychiatry Research: A A B BDocument6 pagesPsychiatry Research: A A B BLady HeruNo ratings yet
- Journal of Psychiatric ResearchDocument9 pagesJournal of Psychiatric ResearchLady HeruNo ratings yet
- 10 1371@journal Pmed 1002924Document16 pages10 1371@journal Pmed 1002924Lady HeruNo ratings yet
- Applied Nursing Research 48 (2019) 68-74Document7 pagesApplied Nursing Research 48 (2019) 68-74Lady HeruNo ratings yet
- Marguerite 2017Document6 pagesMarguerite 2017Lady HeruNo ratings yet
- Bademli 2016Document6 pagesBademli 2016Lady HeruNo ratings yet
- Coping With StressDocument1 pageCoping With StresslindaNo ratings yet
- Body Shame BumilDocument7 pagesBody Shame BumilLady HeruNo ratings yet
- Archives of Psychiatric Nursing: Kerime Bademli, Zekiye Çetinkaya DumanDocument5 pagesArchives of Psychiatric Nursing: Kerime Bademli, Zekiye Çetinkaya DumanLady HeruNo ratings yet
- Body Shame BB Over Weight PD Wanita-1 PDFDocument9 pagesBody Shame BB Over Weight PD Wanita-1 PDFLady HeruNo ratings yet
- Coplan Et Al-2018-Social DevelopmentDocument15 pagesCoplan Et Al-2018-Social DevelopmentLady HeruNo ratings yet
- Durand-Texte 2018 J. Phys.: Conf. Ser. 1149 012008Document9 pagesDurand-Texte 2018 J. Phys.: Conf. Ser. 1149 012008Lady HeruNo ratings yet
- 13th International Conference On Vibration Measurements by Laser and Noncontact TechniquesDocument3 pages13th International Conference On Vibration Measurements by Laser and Noncontact TechniquesLady HeruNo ratings yet
- Body Shame BumilDocument7 pagesBody Shame BumilLady HeruNo ratings yet
- 1 s2.0 S0262885613001790 MainDocument7 pages1 s2.0 S0262885613001790 MainLady HeruNo ratings yet
- Body Shame BB Over Weight PD Wanita-1 PDFDocument9 pagesBody Shame BB Over Weight PD Wanita-1 PDFLady HeruNo ratings yet
- 1 s2.0 S0262885613001790 MainDocument7 pages1 s2.0 S0262885613001790 MainLady HeruNo ratings yet
- Smith Nielsen, J.a Implementation of the Alarm Distress Baby Scale as a Universal Screening Instrument in Primary Care Feasibility Acceptability and Predictors of Professionals Adherence to GuidelinesArticle 2018Document10 pagesSmith Nielsen, J.a Implementation of the Alarm Distress Baby Scale as a Universal Screening Instrument in Primary Care Feasibility Acceptability and Predictors of Professionals Adherence to GuidelinesArticle 2018Lady HeruNo ratings yet
- Isn't RestraintDocument13 pagesIsn't RestraintLady HeruNo ratings yet
- Herbert - Nyirenda 1590992698 ADocument39 pagesHerbert - Nyirenda 1590992698 ADavid LyeluNo ratings yet
- Breast Surgery Indications and TechniquesDocument302 pagesBreast Surgery Indications and TechniquesLasha OsepaishviliNo ratings yet
- Rubrics NCP NCM 103 SL Funda VSDocument1 pageRubrics NCP NCM 103 SL Funda VSJohn TacordaJrNo ratings yet
- Big Data Security and Privacy in Healthcare: A Review Big Data Security and Privacy in Healthcare: A ReviewDocument8 pagesBig Data Security and Privacy in Healthcare: A Review Big Data Security and Privacy in Healthcare: A ReviewDalene EvangelioNo ratings yet
- Tooth Implant Supported Prosthesis: A Literature ReviewDocument8 pagesTooth Implant Supported Prosthesis: A Literature ReviewTung Thanh NguyenNo ratings yet
- International Journal of Nursing Studies: Qi Lu, Jan Mårtensson, Yue Zhao, Linda JohanssonDocument8 pagesInternational Journal of Nursing Studies: Qi Lu, Jan Mårtensson, Yue Zhao, Linda JohanssonAbdul HadiNo ratings yet
- Report of Medicare Multispeciality Hospital and Trauma CentreDocument5 pagesReport of Medicare Multispeciality Hospital and Trauma CentremuskanNo ratings yet
- Review Article UDC 616.8-009:616.31Document7 pagesReview Article UDC 616.8-009:616.31Bernarda MrakNo ratings yet
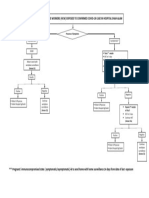
- Management of Healthcare Workers (HCW) Exposed To Confirmed Covid-19 Case in Hospital Shah AlamDocument1 pageManagement of Healthcare Workers (HCW) Exposed To Confirmed Covid-19 Case in Hospital Shah AlamNurhafizah IbrahimNo ratings yet
- Clarion Technologies: at A GlanceDocument7 pagesClarion Technologies: at A GlanceChetan PrasadNo ratings yet
- Process RecordingsDocument4 pagesProcess RecordingsJayakrishnan P KripNo ratings yet
- 27 Invisalign em 10 Minutos Com Renato MussaDocument60 pages27 Invisalign em 10 Minutos Com Renato MussaDiego LopezNo ratings yet
- History/ Exam: Ending The Admission AssessmentDocument5 pagesHistory/ Exam: Ending The Admission AssessmentLyons SchimttNo ratings yet
- Reviewer in Health Assessment (Lecture) - Battery Examination 2019Document4 pagesReviewer in Health Assessment (Lecture) - Battery Examination 2019zebzeb STEMA50% (2)
- Case ConceptualizationDocument18 pagesCase ConceptualizationKrishno RaeNo ratings yet
- Advance ProgramDocument100 pagesAdvance ProgrambibNo ratings yet
- Introduction 2 AyushDocument58 pagesIntroduction 2 Ayushsumaiya choudharyNo ratings yet
- FDA Guidance - CGMP For Clinical TrialsDocument42 pagesFDA Guidance - CGMP For Clinical TrialsNelson Alejandro Fierro100% (1)
- Fieldtrip Permission and Medical FormDocument3 pagesFieldtrip Permission and Medical Formapi-357287502No ratings yet
- Nurses Handbook Health AssessmentDocument3 pagesNurses Handbook Health Assessmentphoebjaetan0% (1)
- 34 Ms Surgery LogbookDocument111 pages34 Ms Surgery LogbookMohamedHossam50% (2)
- Health Education LM Week 1 and 2Document8 pagesHealth Education LM Week 1 and 2Joice LenteriaNo ratings yet
- Neonatal Pain Assessment EvidenceDocument4 pagesNeonatal Pain Assessment EvidenceDewi MaharaniNo ratings yet
- Assess Appropriateness For Clinical Condition. Heart Rate Typically 50/min If BradyarrhythmiaDocument1 pageAssess Appropriateness For Clinical Condition. Heart Rate Typically 50/min If BradyarrhythmiaatikaNo ratings yet
- Letter of Intent Rmvega DvsDocument2 pagesLetter of Intent Rmvega DvsZele VegaNo ratings yet
- Sedación Consenso Alemania 2018 PDFDocument76 pagesSedación Consenso Alemania 2018 PDFAnnison Hector Ramos BravoNo ratings yet
- Community Dentistry Flashcards - QuizletDocument14 pagesCommunity Dentistry Flashcards - QuizletRMNo ratings yet
- Government of Odisha Health & Family Welfare DepartmentDocument3 pagesGovernment of Odisha Health & Family Welfare DepartmentPlacement Cell TISS. SENo ratings yet
- National Drug PolicyDocument4 pagesNational Drug PolicySiva PrasadNo ratings yet
- FNCPDocument2 pagesFNCPMa. Alexis DiezmoNo ratings yet