You might also like
- Covid 19 End by ExcellDocument28 pagesCovid 19 End by ExcellDeni AriyantoNo ratings yet
- A Downscaling Approach To Compare COVID-19 Count Data From Databases Aggregated at Di Fferent Spatial ScalesDocument23 pagesA Downscaling Approach To Compare COVID-19 Count Data From Databases Aggregated at Di Fferent Spatial Scalespopov357No ratings yet
- Systematic Review of The Association Between Rotavirus Infection, or Rotavirus Vaccination and Coeliac DiseaseDocument18 pagesSystematic Review of The Association Between Rotavirus Infection, or Rotavirus Vaccination and Coeliac Diseasepopov357No ratings yet
- 2020 03 24 20042291 Full PDFDocument7 pages2020 03 24 20042291 Full PDFyuriiNo ratings yet
- Melbmodelling FullDocument23 pagesMelbmodelling FullKeith LynchNo ratings yet
- New3 PDFDocument5 pagesNew3 PDFpopov357No ratings yet
- Modeling COVID-19 Epidemics in An Excel SpreadsheeDocument15 pagesModeling COVID-19 Epidemics in An Excel SpreadsheeMagesha kumarNo ratings yet
- Effective Contact Tracing For COVID-19: A Systematic Review: Carl-Etienne - Juneau@umontreal - CaDocument25 pagesEffective Contact Tracing For COVID-19: A Systematic Review: Carl-Etienne - Juneau@umontreal - Capopov357No ratings yet
- 2020 02 28 20029272 FullDocument7 pages2020 02 28 20029272 FullMădălina CiobotariuNo ratings yet
- Spike Mutation Pipeline Reveals The Emergence of A More Transmissible Form of Sars-Cov-2Document33 pagesSpike Mutation Pipeline Reveals The Emergence of A More Transmissible Form of Sars-Cov-2AbdelkaderNo ratings yet
- Mapping A Pandemic: Sars-Cov-2 Seropositivity in The United StatesDocument18 pagesMapping A Pandemic: Sars-Cov-2 Seropositivity in The United StatesRichard MacienteNo ratings yet
- 2020 06 23 20111419v2 Full PDFDocument17 pages2020 06 23 20111419v2 Full PDFFelipe BrandãoNo ratings yet
- Age-Dependent Immune Response To The Biontech/Pfizer BNT162b2 COVID-19 VaccinationDocument15 pagesAge-Dependent Immune Response To The Biontech/Pfizer BNT162b2 COVID-19 VaccinationIoana SoraNo ratings yet
- The Infection Fatality Rate of COVID-19 Inferred From Seroprevalence DataDocument36 pagesThe Infection Fatality Rate of COVID-19 Inferred From Seroprevalence DataFelipe BrandãoNo ratings yet
- Use of Antivirals and Antibiotics For COVID-19 in Mexico City: A Real-World Multicenter Cohort StudyDocument38 pagesUse of Antivirals and Antibiotics For COVID-19 in Mexico City: A Real-World Multicenter Cohort StudyutariNo ratings yet
- Equivalency of Protection From Natural Immunity in COVID-19 Recovered Versus Fully Vaccinated Persons: A Systematic Review and Pooled AnalysisDocument30 pagesEquivalency of Protection From Natural Immunity in COVID-19 Recovered Versus Fully Vaccinated Persons: A Systematic Review and Pooled AnalysisPDFReadAndDevelopNo ratings yet
- Mathematical Predictions For Covid-19 As PDFDocument16 pagesMathematical Predictions For Covid-19 As PDFVinayaga Murthy GNo ratings yet
- Mitigation and Herd Immunity Strategy For COVID-19 Is Likely To FailDocument24 pagesMitigation and Herd Immunity Strategy For COVID-19 Is Likely To FailArt Anthony Zoilo MunioNo ratings yet
- Projecting The Impact of Sars-Cov-2 Variants On The Covid-19 Epidemic and Social Restoration in The United States: A Mathematical Modelling StudyDocument13 pagesProjecting The Impact of Sars-Cov-2 Variants On The Covid-19 Epidemic and Social Restoration in The United States: A Mathematical Modelling Studyledyz cuesta herreraNo ratings yet
- Paul Romer PandemiaDocument17 pagesPaul Romer PandemiaJesus RoblesNo ratings yet
- MainDocument37 pagesMainCarla CANo ratings yet
- Flattening The Curve Is Not Enough, We Need To Squash It: An Explainer Using A Simple ModelDocument14 pagesFlattening The Curve Is Not Enough, We Need To Squash It: An Explainer Using A Simple ModelThea LandichoNo ratings yet
- Preprinting The COVID-19 Pandemic: Jonathon - Coates@qmul - Ac.ukDocument42 pagesPreprinting The COVID-19 Pandemic: Jonathon - Coates@qmul - Ac.ukMinh Tú NguyễnNo ratings yet
- COVID-19 Trend in Bangladesh: Deviation From Epidemiological Model and Critical Analysis of The Possible FactorsDocument26 pagesCOVID-19 Trend in Bangladesh: Deviation From Epidemiological Model and Critical Analysis of The Possible FactorsNazmul IslamNo ratings yet
- Asymptotic Estimates of Sars-Cov-2 Infection Counts and Their Sensitivity To Stochastic PerturbationDocument11 pagesAsymptotic Estimates of Sars-Cov-2 Infection Counts and Their Sensitivity To Stochastic PerturbationenocsigalNo ratings yet
- Social Interventions Can Lower COVID-19 Deaths in Middleincome CountriesDocument22 pagesSocial Interventions Can Lower COVID-19 Deaths in Middleincome Countriesangel.paternina423No ratings yet
- Preprinting The COVID-19 Pandemic: Jonathon - Coates@qmul - Ac.ukDocument34 pagesPreprinting The COVID-19 Pandemic: Jonathon - Coates@qmul - Ac.ukCOOKNo ratings yet
- Transmission Potential of Vaccinated and Unvaccinated Persons Infected With The SARS-CoV-2 Delta Variant in A Federal Prison, July-August 2021Document27 pagesTransmission Potential of Vaccinated and Unvaccinated Persons Infected With The SARS-CoV-2 Delta Variant in A Federal Prison, July-August 2021Jim Hoft100% (1)
- Pokusne Myši - DokumentDocument25 pagesPokusne Myši - DokumenthctagsNo ratings yet
- Effacy of IvermectinDocument31 pagesEffacy of IvermectinPaul VanNo ratings yet
- Case 8Document22 pagesCase 8Muhammad HamzaNo ratings yet
- Immunological Characteristics Govern The Changing Severity of COVID-19 During The Transition To EndemicityDocument27 pagesImmunological Characteristics Govern The Changing Severity of COVID-19 During The Transition To Endemicitypopov357No ratings yet
- Modeling The Impact of Social Distancing, Testing, Contact TracingDocument31 pagesModeling The Impact of Social Distancing, Testing, Contact TracingIkmal ShahromNo ratings yet
- 2020 04 24 20078782v1 FullDocument41 pages2020 04 24 20078782v1 FullAbay SisayNo ratings yet
- 1nihpp-2020 06 10 20127589Document10 pages1nihpp-2020 06 10 20127589SANo ratings yet
- 2020 06 02 20120014v1 FullDocument15 pages2020 06 02 20120014v1 FullNATALIA BASTONo ratings yet
- Fourier Analysis Using The Number of COVID-19 Daily Deaths in The USDocument4 pagesFourier Analysis Using The Number of COVID-19 Daily Deaths in The USRenzo Antonio Condori TolentinoNo ratings yet
- Title: Decreased Sars-Cov-2 Viral Load Following VaccinationDocument12 pagesTitle: Decreased Sars-Cov-2 Viral Load Following VaccinationJared Michael BergerNo ratings yet
- Chen Et Al. (2021) Prioritizing Allocation of COVID-19 Vaccines Based On Social Contacts Increases Vaccination EffectivenessDocument44 pagesChen Et Al. (2021) Prioritizing Allocation of COVID-19 Vaccines Based On Social Contacts Increases Vaccination EffectivenessCristian Fernando Sanabria BautistaNo ratings yet
- The Impact of High Frequency Rapid Viral Antigen Screening On COVID-19 Spread and Outcomes: A Validation and Modeling StudyDocument41 pagesThe Impact of High Frequency Rapid Viral Antigen Screening On COVID-19 Spread and Outcomes: A Validation and Modeling StudyJuensNo ratings yet
- MIlls Et AlDocument24 pagesMIlls Et AlAna Carolina Pecanha Antonio AantonioNo ratings yet
- SceirdDocument9 pagesSceirdGiaWay HsuNo ratings yet
- Correlates of Protection Against Symptomatic and Asymptomatic Sars-Cov-2 InfectionDocument31 pagesCorrelates of Protection Against Symptomatic and Asymptomatic Sars-Cov-2 InfectionAbasyakira RaihanNo ratings yet
- 2020 08 03 20167361v1 FullDocument28 pages2020 08 03 20167361v1 FullNovel SaputraNo ratings yet
- Optimism and Caution For An Inactivated COVID-19 Vaccine: Laura Cornelissen, Emmanuel AndréDocument2 pagesOptimism and Caution For An Inactivated COVID-19 Vaccine: Laura Cornelissen, Emmanuel AndréZahid NabiNo ratings yet
- Covidscreen: Explainable Deep Learning Framework For Differential Diagnosis of Covid-19 Using Chest X-RaysDocument22 pagesCovidscreen: Explainable Deep Learning Framework For Differential Diagnosis of Covid-19 Using Chest X-RaysKaremNo ratings yet
- Symptom Clusters in Covid19: A Potential Clinical Prediction Tool From The COVID Symptom Study AppDocument12 pagesSymptom Clusters in Covid19: A Potential Clinical Prediction Tool From The COVID Symptom Study AppAidNo ratings yet
- Burden and Prevalence of Prognostic Factors For SeDocument17 pagesBurden and Prevalence of Prognostic Factors For SeMubariz MirzayevNo ratings yet
- Estudio de Cohorte ObservacionalDocument22 pagesEstudio de Cohorte ObservacionalHARUMI DEL ROSARIO MONTALVAN VEGANo ratings yet
- Third Wave in IndiaDocument14 pagesThird Wave in IndiaGaurav BatniNo ratings yet
- Disbiose Predispoe A Covid 19lDocument44 pagesDisbiose Predispoe A Covid 19lAlexandre BernardesNo ratings yet
- Comprehensive Analysis of The Key Epidemiological Parameters To Evaluate The Impact of BCG Vaccination On COVID-19 PandemicDocument32 pagesComprehensive Analysis of The Key Epidemiological Parameters To Evaluate The Impact of BCG Vaccination On COVID-19 PandemicsushanprazNo ratings yet
- Christian HolmDocument10 pagesChristian HolmMaureen KoesnadiNo ratings yet
- UAQ Embriones Infectados y Tratados Con CLO2Document35 pagesUAQ Embriones Infectados y Tratados Con CLO2jchaiyakhomNo ratings yet
- Implications of The COVID-19 Pandemic On Eliminating Trachoma As A Public Health ProblemDocument17 pagesImplications of The COVID-19 Pandemic On Eliminating Trachoma As A Public Health ProblemZahra Kesturi RifandariNo ratings yet
- Covidx-Us - An Open-Access Benchmark Dataset of Ultrasound Imaging Data For Ai-Driven Covid-19 Analytics AuthorsDocument14 pagesCovidx-Us - An Open-Access Benchmark Dataset of Ultrasound Imaging Data For Ai-Driven Covid-19 Analytics AuthorsIshani Vajpayee (P19HSS006)No ratings yet
- A Study To Assess The Post Covid Home Quarantine Stress Level in Second Wave Among General Population in A Selected CommunityDocument3 pagesA Study To Assess The Post Covid Home Quarantine Stress Level in Second Wave Among General Population in A Selected CommunityEditor IJTSRDNo ratings yet
- Distinct Regimes of Particle and Virus Abundance eDocument10 pagesDistinct Regimes of Particle and Virus Abundance eGustavo MiguelNo ratings yet
- A 1 To 1000 Sars-Cov-2 Reinfection Proportion in Members of A Large Healthcare Provider in Israel: A Preliminary ReportDocument16 pagesA 1 To 1000 Sars-Cov-2 Reinfection Proportion in Members of A Large Healthcare Provider in Israel: A Preliminary ReportJimmy A. Camones ObregonNo ratings yet
- Beyond One Health: From Recognition to ResultsFrom EverandBeyond One Health: From Recognition to ResultsJohn A. HerrmannNo ratings yet
- Rosa Luxemburg: The Russian RevolutionDocument18 pagesRosa Luxemburg: The Russian RevolutionMartin ThomasNo ratings yet
- High Prevalence of SARS CoV 2 England Sep 2020 S Riley Et Al 26 Sep 2020Document21 pagesHigh Prevalence of SARS CoV 2 England Sep 2020 S Riley Et Al 26 Sep 2020Martin ThomasNo ratings yet
- Age Groups That Sustain Resurging COVID-19 M Monod Et Al 17 Sep 2020Document35 pagesAge Groups That Sustain Resurging COVID-19 M Monod Et Al 17 Sep 2020Martin ThomasNo ratings yet
- Furloughing A Adams-Prassl Et Al 17 Aug 2020Document47 pagesFurloughing A Adams-Prassl Et Al 17 Aug 2020Martin ThomasNo ratings yet
- Distancing and Covid-19 N Jones Et Al 25 Aug 2020Document6 pagesDistancing and Covid-19 N Jones Et Al 25 Aug 2020Martin ThomasNo ratings yet
- Response To COVID-19 in South Korea - N - Ferguson - Et - Al - 29 - May - 2020Document16 pagesResponse To COVID-19 in South Korea - N - Ferguson - Et - Al - 29 - May - 2020Martin ThomasNo ratings yet
- Lessons From Easing Covid Restrictions E Han Et Al 24 Sep 2020 PDFDocument10 pagesLessons From Easing Covid Restrictions E Han Et Al 24 Sep 2020 PDFMartin ThomasNo ratings yet
- Step Course Booklet 2019 20Document82 pagesStep Course Booklet 2019 20Martin ThomasNo ratings yet
- Coronavirus Infection Survey UK ONS 13 Nov 2020Document23 pagesCoronavirus Infection Survey UK ONS 13 Nov 2020Martin ThomasNo ratings yet
- Normal Risk and Dangers of Covid19 D Spiegelhalter 9 Sep 2020Document7 pagesNormal Risk and Dangers of Covid19 D Spiegelhalter 9 Sep 2020Martin ThomasNo ratings yet
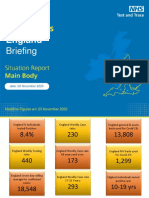
- Coronavirus England Briefing 26 November 2020 NHS Test&TraceDocument79 pagesCoronavirus England Briefing 26 November 2020 NHS Test&TraceMartin ThomasNo ratings yet
- Trade Unions Yesterday, Today, and TomorrowDocument8 pagesTrade Unions Yesterday, Today, and TomorrowMartin ThomasNo ratings yet
- The Effectiveness of Population-Wide, Rapid Antigen Test-Based Screening in Reducing Sars-Cov-2 Infection Prevalence in SlovakiaDocument25 pagesThe Effectiveness of Population-Wide, Rapid Antigen Test-Based Screening in Reducing Sars-Cov-2 Infection Prevalence in SlovakiaMartin ThomasNo ratings yet
- Anti-Semitism and Anti-Muslim Racism in EuropeDocument12 pagesAnti-Semitism and Anti-Muslim Racism in EuropeMartin ThomasNo ratings yet
- Morality, Revolution, The Bolsheviks, and UsDocument8 pagesMorality, Revolution, The Bolsheviks, and UsMartin ThomasNo ratings yet
- Nine Years On From The Crash of 2008: The New Left, The New Right, and The Resilience of NeoliberalismDocument29 pagesNine Years On From The Crash of 2008: The New Left, The New Right, and The Resilience of NeoliberalismMartin ThomasNo ratings yet
- Marxists and National QuestionsDocument22 pagesMarxists and National QuestionsMartin ThomasNo ratings yet
- Four Missing Years: A Review of Thomas Twiss's "Trotsky and The Problem of Soviet Bureaucracy"Document15 pagesFour Missing Years: A Review of Thomas Twiss's "Trotsky and The Problem of Soviet Bureaucracy"Martin ThomasNo ratings yet
- Left AntisemitismDocument28 pagesLeft AntisemitismMartin Thomas100% (1)
- Marxists, The Labour Movement, and The Labour PartyDocument35 pagesMarxists, The Labour Movement, and The Labour PartyMartin ThomasNo ratings yet
- Fact Sheet On Some Left Governments From The 1970s To 2018Document2 pagesFact Sheet On Some Left Governments From The 1970s To 2018Martin ThomasNo ratings yet
- Workers' Liberty: Marx'S CapitalDocument8 pagesWorkers' Liberty: Marx'S CapitalMartin ThomasNo ratings yet
- Emmy Noether: The Mother of Modern AlgebraDocument5 pagesEmmy Noether: The Mother of Modern AlgebraMartin ThomasNo ratings yet
- Maclaurin Series Via GraphsDocument34 pagesMaclaurin Series Via GraphsMartin ThomasNo ratings yet
- 160822jeff Rickertt Ernie Lane V2Document5 pages160822jeff Rickertt Ernie Lane V2Martin ThomasNo ratings yet
- Workers' Guide To IrelandDocument20 pagesWorkers' Guide To IrelandMartin ThomasNo ratings yet
- Fate PDFDocument487 pagesFate PDFMartin ThomasNo ratings yet
- Review of "Against The Troika"Document2 pagesReview of "Against The Troika"Martin ThomasNo ratings yet
- Fate PDFDocument487 pagesFate PDFMartin ThomasNo ratings yet
- Atty. SungaDocument22 pagesAtty. SungaKris MercadoNo ratings yet
- M.D. (Acu) SyllabusDocument5 pagesM.D. (Acu) SyllabusS Ve SuriyaNo ratings yet
- AnatomyDocument4 pagesAnatomySureen PaduaNo ratings yet
- Ganendra Art House: 8 Lorong 16/7B, 46350 Petaling Jaya, Selangor, MalaysiaDocument25 pagesGanendra Art House: 8 Lorong 16/7B, 46350 Petaling Jaya, Selangor, MalaysiaFiorela Estrella VentocillaNo ratings yet
- Appellate BriefDocument3 pagesAppellate Briefelan de noir100% (1)
- Practical Auditing by Empleo 2022 Chapter 4 Receivables Related RevenuesDocument55 pagesPractical Auditing by Empleo 2022 Chapter 4 Receivables Related RevenuesDarence IndayaNo ratings yet
- Periyava Times Apr 2017 2 PDFDocument4 pagesPeriyava Times Apr 2017 2 PDFAnand SNo ratings yet
- Novena To ST JudeDocument2 pagesNovena To ST JudeBeatrice Mae ChuaNo ratings yet
- C.V FinalDocument4 pagesC.V Finalcastillo_leoNo ratings yet
- Oracle® Inventory: Consigned Inventory From Supplier Process Guide Release 12.1Document76 pagesOracle® Inventory: Consigned Inventory From Supplier Process Guide Release 12.1Guillermo ToddNo ratings yet
- Caning Should Not Be Allowed in Schools TodayDocument2 pagesCaning Should Not Be Allowed in Schools TodayHolyZikr100% (2)
- McDonald's RecipeDocument18 pagesMcDonald's RecipeoxyvilleNo ratings yet
- SCAM (Muet)Document6 pagesSCAM (Muet)Muhammad FahmiNo ratings yet
- Accomplishment and Narrative Report OctDocument4 pagesAccomplishment and Narrative Report OctGillian Bollozos-CabuguasNo ratings yet
- Voith QB III 1011 eDocument22 pagesVoith QB III 1011 evoithNo ratings yet
- Espiloy COT DLP Math 5 Q2Document7 pagesEspiloy COT DLP Math 5 Q2Adeline Rose B. Espiloy100% (3)
- CONCEPT DESIGN ALUM C.W SCHUCO ANDALUSIA Rev01.10.03.222Document118 pagesCONCEPT DESIGN ALUM C.W SCHUCO ANDALUSIA Rev01.10.03.222MoustafaNo ratings yet
- Presentation On Online Car Rental Management System: Presented byDocument41 pagesPresentation On Online Car Rental Management System: Presented byNikhilesh K100% (2)
- Mark Magazine#64Document197 pagesMark Magazine#64Андрей КанищевNo ratings yet
- Finance Management Individual AssDocument33 pagesFinance Management Individual AssDevan MoroganNo ratings yet
- Deed of Donation BicycleDocument2 pagesDeed of Donation BicycleCharlemagne PapioNo ratings yet
- Grade 12 Mathematical Literacy: Question Paper 1 MARKS: 150 TIME: 3 HoursDocument53 pagesGrade 12 Mathematical Literacy: Question Paper 1 MARKS: 150 TIME: 3 HoursOfentse MothapoNo ratings yet
- English IODocument6 pagesEnglish IOAarav MathurNo ratings yet
- Kaulachara (Written by Guruji and Posted 11/3/10)Document4 pagesKaulachara (Written by Guruji and Posted 11/3/10)Matt Huish100% (1)
- Courtney Loper-ResumeDocument2 pagesCourtney Loper-Resumeapi-354618234No ratings yet
- Design and Construction of A Variable Frequency Drive Industrial ApplicationsDocument9 pagesDesign and Construction of A Variable Frequency Drive Industrial ApplicationsMarc TcheukabaNo ratings yet
- Manonmaniam Sundaranar University: B.B.A. - Ii YearDocument61 pagesManonmaniam Sundaranar University: B.B.A. - Ii YearLovely Dhanaa4848No ratings yet
- Comprehension QuestionsDocument6 pagesComprehension Questionsapi-245567970No ratings yet
- Yuphaphann Hoonchamlong - Thai Language and Culture For Beginners Volume 1Document293 pagesYuphaphann Hoonchamlong - Thai Language and Culture For Beginners Volume 1Ion SystemsNo ratings yet
- Supplementary Cause List - 16.10.2023Document7 pagesSupplementary Cause List - 16.10.2023Aamir BhatNo ratings yet