You might also like
- NCM 105A Nutrition and Diet Therapy Laboratory Laboratory Exercise No. 8 Macronutrients - FatsDocument6 pagesNCM 105A Nutrition and Diet Therapy Laboratory Laboratory Exercise No. 8 Macronutrients - Fatsann campos67% (3)
- Nursing Care Plan For DM PatientDocument10 pagesNursing Care Plan For DM PatientRainier Rhett Concha100% (5)
- 2018 Article 3585Document14 pages2018 Article 3585timosp1973No ratings yet
- The Effectiveness of Population-Wide, Rapid Antigen Test-Based Screening in Reducing Sars-Cov-2 Infection Prevalence in SlovakiaDocument25 pagesThe Effectiveness of Population-Wide, Rapid Antigen Test-Based Screening in Reducing Sars-Cov-2 Infection Prevalence in SlovakiaMartin ThomasNo ratings yet
- Zoonotic Ascariasis, United Kingdom: LettersDocument3 pagesZoonotic Ascariasis, United Kingdom: LettersAustine OsaweNo ratings yet
- Wabah TBC Di VietnamDocument8 pagesWabah TBC Di VietnamSatya WangsaNo ratings yet
- Global Rotavirus Illness and DeathsDocument8 pagesGlobal Rotavirus Illness and DeathsElena NazâruNo ratings yet
- React1 r9 Interim PreprintDocument22 pagesReact1 r9 Interim PreprintOB NewsNo ratings yet
- Ijmr 151 419Document5 pagesIjmr 151 419Assao BachirNo ratings yet
- Long-Term Impact of Acyclovir Suppressive Therapy On Genital and Plasma HIV RNA in Tanzanian Women: A Randomized Controlled TrialDocument14 pagesLong-Term Impact of Acyclovir Suppressive Therapy On Genital and Plasma HIV RNA in Tanzanian Women: A Randomized Controlled TrialEpi PanjaitanNo ratings yet
- Pokusne Myši - DokumentDocument25 pagesPokusne Myši - DokumenthctagsNo ratings yet
- Group 2 (FE64) - Sampling Distribution and EstimationDocument11 pagesGroup 2 (FE64) - Sampling Distribution and EstimationVũ GiangNo ratings yet
- Enhanced Surveillance of COVID-19 in Scotland: Population-Based Seroprevalence SurveillanceDocument3 pagesEnhanced Surveillance of COVID-19 in Scotland: Population-Based Seroprevalence SurveillancecamaferNo ratings yet
- New England Journal Medicine: The ofDocument11 pagesNew England Journal Medicine: The ofDevina Indah PermatasariNo ratings yet
- Transmission of Sars-Cov-2 Lineage B.1.1.7 in England: Insights From Linking Epidemiological and Genetic DataDocument37 pagesTransmission of Sars-Cov-2 Lineage B.1.1.7 in England: Insights From Linking Epidemiological and Genetic DataBearNo ratings yet
- Ciaa 1764Document16 pagesCiaa 1764Zoltán BaloghNo ratings yet
- Testis PDFDocument8 pagesTestis PDFVlatka MartinovichNo ratings yet
- Jurnal YuliaDocument8 pagesJurnal YuliaRayantiNo ratings yet
- Rotavirus Leading Cause of Childhood Diarrhea HospitalizationsDocument3 pagesRotavirus Leading Cause of Childhood Diarrhea HospitalizationsAnwar AliNo ratings yet
- 6.2 More Times Than ReportedDocument12 pages6.2 More Times Than ReportedMahmoudAboAlSamenNo ratings yet
- 8.A Case Report of Rabies With Long Incubation ImporDocument3 pages8.A Case Report of Rabies With Long Incubation ImporAndra CristianaNo ratings yet
- 1 s2.0 S1835561716301314 MainDocument7 pages1 s2.0 S1835561716301314 MainBam ManNo ratings yet
- Who - Bulletin VN PrevalenceDocument8 pagesWho - Bulletin VN PrevalenceNguyen Binh HoaNo ratings yet
- Increased Household Transmission of COVID-19 Cases Associated With SARS-CoV-2 Variant of Concern B.1.617.2: A National Casecontrol StudyDocument21 pagesIncreased Household Transmission of COVID-19 Cases Associated With SARS-CoV-2 Variant of Concern B.1.617.2: A National Casecontrol StudyChequea BoliviaNo ratings yet
- Studija o Omikronu Imperial CollegeaDocument12 pagesStudija o Omikronu Imperial CollegeaIndex.hrNo ratings yet
- Imperial CollegeDocument31 pagesImperial CollegeElPaisUyNo ratings yet
- Burnett2017Document16 pagesBurnett2017Jane DDNo ratings yet
- Respiratory Syncytial Virus Infections in Children With Acute Myeloid Leukemia: A Report From The Children's Oncology GroupDocument3 pagesRespiratory Syncytial Virus Infections in Children With Acute Myeloid Leukemia: A Report From The Children's Oncology GrouperickmattosNo ratings yet
- Novitasari - Is Premigration Health Screening For Tuberculosis WorthwileDocument12 pagesNovitasari - Is Premigration Health Screening For Tuberculosis Worthwileontet28No ratings yet
- Salmonella Enterica Serovar Enteritidis, England and Wales, 1945-2011Document8 pagesSalmonella Enterica Serovar Enteritidis, England and Wales, 1945-2011Mark ReinhardtNo ratings yet
- Pertussis VaccinesDocument7 pagesPertussis VaccinesNur SulistiyaningsihNo ratings yet
- Rockson Ohene Asante 2235026 - Epidemiology Assignment by Pratap Kumar Jena SirDocument11 pagesRockson Ohene Asante 2235026 - Epidemiology Assignment by Pratap Kumar Jena SirRockson Ohene AsanteNo ratings yet
- Mclaws 2015Document11 pagesMclaws 2015Novi LatifaNo ratings yet
- 2020 - Covid 19 Seroprevalencia de Anticuerpos en El Condado de Santa Clara, CaliforniaDocument17 pages2020 - Covid 19 Seroprevalencia de Anticuerpos en El Condado de Santa Clara, Californiasimps incelNo ratings yet
- Christian HolmDocument10 pagesChristian HolmMaureen KoesnadiNo ratings yet
- D3 PDFDocument24 pagesD3 PDFpopov357No ratings yet
- Estimating Malaria Parasite Prevalence From Community Surveys in Uganda: A Comparison of Microscopy, Rapid Diagnostic Tests and Polymerase Chain ReactionDocument11 pagesEstimating Malaria Parasite Prevalence From Community Surveys in Uganda: A Comparison of Microscopy, Rapid Diagnostic Tests and Polymerase Chain Reactionibrahima1968No ratings yet
- Estimating and Modelling The Transmissibility of Middle East Respiratory Syndrome Corona Virus During The 2015 Outbreak in The Republic of KoreaDocument32 pagesEstimating and Modelling The Transmissibility of Middle East Respiratory Syndrome Corona Virus During The 2015 Outbreak in The Republic of KoreaMMNo ratings yet
- Genetic Evidence For The Association Between COVID-19 Epidemic Severity and Timing of Non-Pharmaceutical InterventionsDocument7 pagesGenetic Evidence For The Association Between COVID-19 Epidemic Severity and Timing of Non-Pharmaceutical InterventionsLaurin LibudaNo ratings yet
- Valid Chest X-Ray Scoring for TB SeverityDocument8 pagesValid Chest X-Ray Scoring for TB SeverityAlvita DewiNo ratings yet
- Tuberculosis in The Urban Poor Settlements in The PhilippinesDocument10 pagesTuberculosis in The Urban Poor Settlements in The Philippinesbibalshane16No ratings yet
- Computational Science For Engineers - Unit-III - SD With Interactions - Spread of SARS and Enzyme KineticsDocument31 pagesComputational Science For Engineers - Unit-III - SD With Interactions - Spread of SARS and Enzyme Kineticsrt.cseNo ratings yet
- 21-0965-Persisten of IgG in Children After CovidDocument7 pages21-0965-Persisten of IgG in Children After CovidERIE YUWITA SARINo ratings yet
- Biostat 2003 Farrington 621 32Document12 pagesBiostat 2003 Farrington 621 32Jennifer HuffNo ratings yet
- Mcasecsrfcampylob PDFDocument6 pagesMcasecsrfcampylob PDFTeófilo Negróss MassáiNo ratings yet
- Occupational Exposure and Tuberculosis Among Medical Residents in A High-Burden Setting: An Open-Cohort StudyDocument14 pagesOccupational Exposure and Tuberculosis Among Medical Residents in A High-Burden Setting: An Open-Cohort StudyWisnu Syahputra SuryanullahNo ratings yet
- 16 PDFDocument4 pages16 PDFDessy P HariyantiNo ratings yet
- 2020 Bidirectional Association Between Tuberculosis and SarcoidosisDocument8 pages2020 Bidirectional Association Between Tuberculosis and SarcoidosisLCCNo ratings yet
- Antibody Acquisition Models: A New Tool For Serological Surveillance of Malaria Transmission IntensityDocument18 pagesAntibody Acquisition Models: A New Tool For Serological Surveillance of Malaria Transmission IntensityTrhy Rahyou MarbaniatyNo ratings yet
- Coronavirus Infection Survey UK ONS 13 Nov 2020Document23 pagesCoronavirus Infection Survey UK ONS 13 Nov 2020Martin ThomasNo ratings yet
- DEATH STATISTICS - IFR 0.23% - Infection Fatality Rate of COVID-19 - John P A IoannidisDocument37 pagesDEATH STATISTICS - IFR 0.23% - Infection Fatality Rate of COVID-19 - John P A IoannidisPeter100% (1)
- Paper Inggris NEWDocument21 pagesPaper Inggris NEWYolanda Edith P. NababanNo ratings yet
- Effect of Early Antiretroviral TherapyDocument16 pagesEffect of Early Antiretroviral TherapyAryo Damar DjatiNo ratings yet
- The Incidence and Prevalence of Systemic Lupus Erythematosus in The UK, 1999 - 2012Document6 pagesThe Incidence and Prevalence of Systemic Lupus Erythematosus in The UK, 1999 - 2012Bagus MahendraNo ratings yet
- 90532100Document5 pages90532100Devi PuspasariNo ratings yet
- Age-Related Differences in Hospitalization Rates, Clinical Presentation, and Outcomes Among Older Adults Hospitalized With Influenza-U.S. Influenza Hospitalization Surveillance NetworkDocument8 pagesAge-Related Differences in Hospitalization Rates, Clinical Presentation, and Outcomes Among Older Adults Hospitalized With Influenza-U.S. Influenza Hospitalization Surveillance NetworkTony RobertsNo ratings yet
- BMC Public Health: Risk Factors For Pulmonary Tuberculosis: A Clinic-Based Case Control Study in The GambiaDocument7 pagesBMC Public Health: Risk Factors For Pulmonary Tuberculosis: A Clinic-Based Case Control Study in The Gambiapuskesmas beloNo ratings yet
- 9-Article Buckle PDFDocument9 pages9-Article Buckle PDFMuhammad Agus ListinNo ratings yet
- Typhoid fever disease burden and antimicrobial resistance in five Asian countriesDocument4 pagesTyphoid fever disease burden and antimicrobial resistance in five Asian countriesPutu SuartiniNo ratings yet
- HCW Vs Adult Influenza IncidenceDocument9 pagesHCW Vs Adult Influenza Incidencereza_adrian_2No ratings yet
- Beyond One Health: From Recognition to ResultsFrom EverandBeyond One Health: From Recognition to ResultsJohn A. HerrmannNo ratings yet
- SARS-CoV-2 Viral Outbreak Investigation: Laboratory PerspectiveFrom EverandSARS-CoV-2 Viral Outbreak Investigation: Laboratory PerspectiveNo ratings yet
- Furloughing A Adams-Prassl Et Al 17 Aug 2020Document47 pagesFurloughing A Adams-Prassl Et Al 17 Aug 2020Martin ThomasNo ratings yet
- Response To COVID-19 in South Korea - N - Ferguson - Et - Al - 29 - May - 2020Document16 pagesResponse To COVID-19 in South Korea - N - Ferguson - Et - Al - 29 - May - 2020Martin ThomasNo ratings yet
- Normal Risk and Dangers of Covid19 D Spiegelhalter 9 Sep 2020Document7 pagesNormal Risk and Dangers of Covid19 D Spiegelhalter 9 Sep 2020Martin ThomasNo ratings yet
- Lessons From Easing Covid Restrictions E Han Et Al 24 Sep 2020 PDFDocument10 pagesLessons From Easing Covid Restrictions E Han Et Al 24 Sep 2020 PDFMartin ThomasNo ratings yet
- Coronavirus Infection Survey UK ONS 13 Nov 2020Document23 pagesCoronavirus Infection Survey UK ONS 13 Nov 2020Martin ThomasNo ratings yet
- Distancing and Covid-19 N Jones Et Al 25 Aug 2020Document6 pagesDistancing and Covid-19 N Jones Et Al 25 Aug 2020Martin ThomasNo ratings yet
- Rosa Luxemburg: The Russian RevolutionDocument18 pagesRosa Luxemburg: The Russian RevolutionMartin ThomasNo ratings yet
- Age Groups That Sustain Resurging COVID-19 M Monod Et Al 17 Sep 2020Document35 pagesAge Groups That Sustain Resurging COVID-19 M Monod Et Al 17 Sep 2020Martin ThomasNo ratings yet
- The COVID-19 Herd Immunity Threshold Is Not Low Fox Et Al 1 Dec 2020Document17 pagesThe COVID-19 Herd Immunity Threshold Is Not Low Fox Et Al 1 Dec 2020Martin ThomasNo ratings yet
- Step Course Booklet 2019 20Document82 pagesStep Course Booklet 2019 20Martin ThomasNo ratings yet
- Marxists and National QuestionsDocument22 pagesMarxists and National QuestionsMartin ThomasNo ratings yet
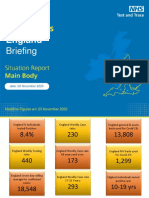
- Coronavirus England Briefing 26 November 2020 NHS Test&TraceDocument79 pagesCoronavirus England Briefing 26 November 2020 NHS Test&TraceMartin ThomasNo ratings yet
- Anti-Semitism and Anti-Muslim Racism in EuropeDocument12 pagesAnti-Semitism and Anti-Muslim Racism in EuropeMartin ThomasNo ratings yet
- Trade Unions Yesterday, Today, and TomorrowDocument8 pagesTrade Unions Yesterday, Today, and TomorrowMartin ThomasNo ratings yet
- Morality, Revolution, The Bolsheviks, and UsDocument8 pagesMorality, Revolution, The Bolsheviks, and UsMartin ThomasNo ratings yet
- Four Missing Years: A Review of Thomas Twiss's "Trotsky and The Problem of Soviet Bureaucracy"Document15 pagesFour Missing Years: A Review of Thomas Twiss's "Trotsky and The Problem of Soviet Bureaucracy"Martin ThomasNo ratings yet
- Workers' Liberty: Marx'S CapitalDocument8 pagesWorkers' Liberty: Marx'S CapitalMartin ThomasNo ratings yet
- Workers' Guide To IrelandDocument20 pagesWorkers' Guide To IrelandMartin ThomasNo ratings yet
- Fact Sheet On Some Left Governments From The 1970s To 2018Document2 pagesFact Sheet On Some Left Governments From The 1970s To 2018Martin ThomasNo ratings yet
- Left Antisemitism: Pseudo-Emancipatory BigotryDocument28 pagesLeft Antisemitism: Pseudo-Emancipatory BigotryMartin Thomas100% (1)
- Marxists, The Labour Movement, and The Labour PartyDocument35 pagesMarxists, The Labour Movement, and The Labour PartyMartin ThomasNo ratings yet
- Nine Years On From The Crash of 2008: The New Left, The New Right, and The Resilience of NeoliberalismDocument29 pagesNine Years On From The Crash of 2008: The New Left, The New Right, and The Resilience of NeoliberalismMartin ThomasNo ratings yet
- Emmy Noether: The Mother of Modern AlgebraDocument5 pagesEmmy Noether: The Mother of Modern AlgebraMartin ThomasNo ratings yet
- Fate PDFDocument487 pagesFate PDFMartin ThomasNo ratings yet
- Review of "Against The Troika"Document2 pagesReview of "Against The Troika"Martin ThomasNo ratings yet
- 160822jeff Rickertt Ernie Lane V2Document5 pages160822jeff Rickertt Ernie Lane V2Martin ThomasNo ratings yet
- Maclaurin Series Via GraphsDocument34 pagesMaclaurin Series Via GraphsMartin ThomasNo ratings yet
- Fate PDFDocument487 pagesFate PDFMartin ThomasNo ratings yet
- The Etiology of Glomerulonephritis: Roles of Infection and AutoimmunityDocument10 pagesThe Etiology of Glomerulonephritis: Roles of Infection and AutoimmunityCarlos DominguezNo ratings yet
- Neuromuscular and Nervous System Q OnlyDocument11 pagesNeuromuscular and Nervous System Q OnlyWenzy CruzNo ratings yet
- Effects of common illegal drugsDocument4 pagesEffects of common illegal drugsKaren DacasinNo ratings yet
- Project Writing Group 2Document1 pageProject Writing Group 2fariyiinNo ratings yet
- Samuel Christian College: "Aerobic, Muscle and Bone Strengthening Activities"Document18 pagesSamuel Christian College: "Aerobic, Muscle and Bone Strengthening Activities"Julie ArcillaNo ratings yet
- Oral Glucose Tolerance TestDocument29 pagesOral Glucose Tolerance TestAhmedmmhNo ratings yet
- Lymphatic System and Body Defenses 1cdnedlio N Marieb Chapter 12 The LymphaticDocument39 pagesLymphatic System and Body Defenses 1cdnedlio N Marieb Chapter 12 The LymphaticOlalekan OyekunleNo ratings yet
- FNCP of ArthritisDocument3 pagesFNCP of ArthritisRaymond Carl GragasinNo ratings yet
- Case Scenario 2 PDFDocument7 pagesCase Scenario 2 PDFChristelle Ann FarralesNo ratings yet
- New Jaundice Poster 2Document1 pageNew Jaundice Poster 2Ruthie DzidziNo ratings yet
- Drrr-Grade 11 - Module1 - J. TabonesDocument19 pagesDrrr-Grade 11 - Module1 - J. TabonesShrl TabonesNo ratings yet
- Nur Jamal SKDocument54 pagesNur Jamal SKshjzjxhxnajsjdNo ratings yet
- Small Bowel: Carcinoid Tumors/Neuroendocrine Tumors: Resident Teaching Conference Sept 5, 2012 Clark D. KensingerDocument32 pagesSmall Bowel: Carcinoid Tumors/Neuroendocrine Tumors: Resident Teaching Conference Sept 5, 2012 Clark D. KensingerMia DangaNo ratings yet
- Massive Male Plus Supplement Review - Ingredients & BenefitsDocument4 pagesMassive Male Plus Supplement Review - Ingredients & BenefitsRakibNo ratings yet
- Drug Alcohol AwarenessDocument59 pagesDrug Alcohol AwarenessCharlotte VertudazoNo ratings yet
- Yatharth Jain - The Black Death MagazineDocument7 pagesYatharth Jain - The Black Death MagazineYatharth JainNo ratings yet
- PAR-Q+ Physical Activity Readiness QuestionnaireDocument2 pagesPAR-Q+ Physical Activity Readiness QuestionnaireMarilyn GalvoNo ratings yet
- Body Revolution Syllabus DraftDocument4 pagesBody Revolution Syllabus Draftapi-508557357No ratings yet
- Rheumatic Fever Is AnDocument7 pagesRheumatic Fever Is AnHamza SaeedNo ratings yet
- Case StudyDocument43 pagesCase StudyAlanoud AlTuwaijriNo ratings yet
- BIOL S302F - Natural Defense and ImmunityDocument68 pagesBIOL S302F - Natural Defense and ImmunityLo Yuen ChanNo ratings yet
- Anticholinesterases: Kanav Bhanot Roll No. 5Document14 pagesAnticholinesterases: Kanav Bhanot Roll No. 5Vivek PandeyNo ratings yet
- Ozone Therapy and Uv Blood Irradiation: What It Helps TreatDocument8 pagesOzone Therapy and Uv Blood Irradiation: What It Helps TreatsumanNo ratings yet
- OPEN MAGAZINE - Latest PDFDocument68 pagesOPEN MAGAZINE - Latest PDFMit AdhvaryuNo ratings yet
- 4 1 1 Student Response Sheet Pathblood (Revised 2 2 15)Document5 pages4 1 1 Student Response Sheet Pathblood (Revised 2 2 15)api-281824634No ratings yet
- Big Five Personality Test Results (MIT LAUNCH)Document2 pagesBig Five Personality Test Results (MIT LAUNCH)Meow100% (1)
- MOA - Miror & Doctor (May, 2023)Document6 pagesMOA - Miror & Doctor (May, 2023)The Crazy SiblingsNo ratings yet
- WHO - Weekly Epidemiological Update On COVID-19 - 22 February 2022Document26 pagesWHO - Weekly Epidemiological Update On COVID-19 - 22 February 2022Adam ForgieNo ratings yet