You might also like
- 11 - Fraktur Dan DislokasiDocument47 pages11 - Fraktur Dan DislokasiCarolyn ZhouNo ratings yet
- Fracture ManagementDocument50 pagesFracture ManagementCharLes OdalNo ratings yet
- 31 & 32.fractures Maxilla MandibleDocument10 pages31 & 32.fractures Maxilla MandibleDurga VoraNo ratings yet
- Fractures: Types, Complications, and ManagementDocument26 pagesFractures: Types, Complications, and Managementsm - kardmNo ratings yet
- Fracrure DislocationDocument109 pagesFracrure DislocationgetemeselewNo ratings yet
- Principles of Fracture FIXDocument63 pagesPrinciples of Fracture FIXAndi NurcahyantiNo ratings yet
- Orthopaedic Surgery Fractures and Dislocations: Tomas Kurakovas MF LL Group 29Document13 pagesOrthopaedic Surgery Fractures and Dislocations: Tomas Kurakovas MF LL Group 29Tomas Kurakovas100% (1)
- Orthopedic NursingDocument23 pagesOrthopedic Nursinggabrielle magdaraog100% (1)
- Basics of FractureDocument12 pagesBasics of Fracturecimahmudraju100% (2)
- Fracture: Suchithra.P.V 1 Year Msc. Nursing College of Nursing AlappuzhaDocument96 pagesFracture: Suchithra.P.V 1 Year Msc. Nursing College of Nursing AlappuzhaAakash A. AgrawalNo ratings yet
- Fracture PP Ahmad Aqel 2013Document32 pagesFracture PP Ahmad Aqel 2013ahmadNo ratings yet
- MS 36Document7 pagesMS 36jefrocNo ratings yet
- Ortho Ward NotesDocument6 pagesOrtho Ward Notesboxed juiceNo ratings yet
- Comprehensive SummaryDocument37 pagesComprehensive Summaryhrg79qzwc2No ratings yet
- Traumatic InjuryDocument64 pagesTraumatic InjuryDYRAH GRACE COPAUSNo ratings yet
- Fracture: Edfran Jed A. Serino MSN 303Document34 pagesFracture: Edfran Jed A. Serino MSN 303Edfran Jed SerinoNo ratings yet
- MusculoskelealDocument32 pagesMusculoskelealEbuka AniNo ratings yet
- FractureDocument125 pagesFractureKlara Devina VanessaNo ratings yet
- Musculoskeletal Trauma GuideDocument99 pagesMusculoskeletal Trauma GuideFatt ZakiNo ratings yet
- Proses Persalinan Normal Eb1Document43 pagesProses Persalinan Normal Eb1Cici RahmaNo ratings yet
- Bahaa Motawea. #. & DislocationsDocument51 pagesBahaa Motawea. #. & DislocationsFathy AlhallagNo ratings yet
- 68 DISEASES 2nd Semsester 3rd Year 1 PDFDocument117 pages68 DISEASES 2nd Semsester 3rd Year 1 PDFJimlord GarciaNo ratings yet
- Complication of FractureDocument79 pagesComplication of FractureAhmad SyahmiNo ratings yet
- General Principles of FracturesDocument27 pagesGeneral Principles of Fracturesallthingali217No ratings yet
- Dr. Luthfi Hidayat, SP - OTDocument39 pagesDr. Luthfi Hidayat, SP - OTadystiNo ratings yet
- Principles of Bone Fracture HealingDocument62 pagesPrinciples of Bone Fracture HealingFuad AbdullahNo ratings yet
- Introduction To Fracture, Bone Healing and Complication: Prof - DR Jameel - Tahseen Mehsen Trauma and Orthopedics SurgeonDocument20 pagesIntroduction To Fracture, Bone Healing and Complication: Prof - DR Jameel - Tahseen Mehsen Trauma and Orthopedics Surgeonحسين رسول ناجيNo ratings yet
- DsdfdfsDocument33 pagesDsdfdfsmayliaNo ratings yet
- Sprain and DislocationDocument9 pagesSprain and Dislocationbhavesh jain100% (1)
- Bone FractureDocument10 pagesBone Fractureraphael chidiebereNo ratings yet
- Bone Healing 1Document42 pagesBone Healing 1bran makmornNo ratings yet
- 2 Principles-Of-FracturesDocument94 pages2 Principles-Of-Fracturesbyanfqha1No ratings yet
- MSK Radiology Imaging Techniques and FindingsDocument54 pagesMSK Radiology Imaging Techniques and FindingsDewa ayu NarheswariNo ratings yet
- 1 Introduction and AssessmentDocument45 pages1 Introduction and AssessmentMaria Lynne ParambitaNo ratings yet
- Bone FractureDocument16 pagesBone FractureMurad KurdiNo ratings yet
- Nursing Management: Musculoskeletal Trauma and Orthopedic SurgeryDocument25 pagesNursing Management: Musculoskeletal Trauma and Orthopedic SurgeryDeannahTampusNo ratings yet
- Fractures and Dislocation: ArnadiDocument30 pagesFractures and Dislocation: ArnadiNizai Rama DeswiraNo ratings yet
- Open and Closed Fractures - 2018 EnglishDocument49 pagesOpen and Closed Fractures - 2018 EnglishЕлена КовбасаNo ratings yet
- FractureDocument27 pagesFractureAkio OzaragaNo ratings yet
- Case Study On Normal Vaginal DeliveryDocument40 pagesCase Study On Normal Vaginal DeliveryPabhat Kumar100% (1)
- A Closed Fracture Does Not Penetrate The SkinDocument5 pagesA Closed Fracture Does Not Penetrate The SkinIvan Liquiran Avenado100% (1)
- Orthopedic EmergenciesDocument75 pagesOrthopedic EmergenciesAlex beharuNo ratings yet
- s-Malunion and nonunionDocument75 pagess-Malunion and nonunionshahnazroeentanmailNo ratings yet
- Fractures: Pathophysiology and EtiologyDocument5 pagesFractures: Pathophysiology and EtiologyHafid JuniorNo ratings yet
- Ilizarov PresentationDocument50 pagesIlizarov PresentationSolomon Sekar100% (1)
- Diagnostic Imaging - 5 - Fractures-Subluxation-Dislocations - Prof - Dr.İsmet TAMERDocument33 pagesDiagnostic Imaging - 5 - Fractures-Subluxation-Dislocations - Prof - Dr.İsmet TAMERAly MssreNo ratings yet
- (Open) Fractures: Potchefstroom Hopital OrthopedicsDocument9 pages(Open) Fractures: Potchefstroom Hopital OrthopedicsUhuebor DavidNo ratings yet
- FIX - Fracture and DislocationDocument80 pagesFIX - Fracture and DislocationWildan Hilmi AnsoriNo ratings yet
- Musculoskeletal Injuries: Fractures and Joint Injuries GuideDocument69 pagesMusculoskeletal Injuries: Fractures and Joint Injuries GuideHeru ChrisNo ratings yet
- Penanganan FrakturDocument78 pagesPenanganan FrakturelizabethmargarethNo ratings yet
- تروما محاضرة 1Document58 pagesتروما محاضرة 1202003339No ratings yet
- Fractures: Ns. Frengki Apryanto, S.Kep., M.Kep Medical/Surgical VII: MusculoskeletalDocument35 pagesFractures: Ns. Frengki Apryanto, S.Kep., M.Kep Medical/Surgical VII: MusculoskeletaldesyNo ratings yet
- Fractures: Ns. Frengki Apryanto, S.Kep., M.Kep Medical/Surgical VII: MusculoskeletalDocument35 pagesFractures: Ns. Frengki Apryanto, S.Kep., M.Kep Medical/Surgical VII: Musculoskeletaldesy100% (1)
- Types and Treatment of FracturesDocument68 pagesTypes and Treatment of FracturesokaciaNo ratings yet
- Fracture Case AbstractDocument27 pagesFracture Case AbstractMaribel Briones JuanNo ratings yet
- Fracture: Group 1Document29 pagesFracture: Group 1Louisse Angeli AbucejoNo ratings yet
- Bone Healing ModuleDocument7 pagesBone Healing ModuleIceKing233No ratings yet
- College of Nursing Adult Nursing Academic Year Lec. Waleed IbrahimDocument6 pagesCollege of Nursing Adult Nursing Academic Year Lec. Waleed Ibrahimمحمد سعد طه احمدNo ratings yet
- Principles of FractureDocument14 pagesPrinciples of Fracturezen.maree6No ratings yet
- Reduction, Relocation and Splinting in Emergency Room (RASER)From EverandReduction, Relocation and Splinting in Emergency Room (RASER)No ratings yet
- Obsessive-Compulsive Disorder (OCD)Document16 pagesObsessive-Compulsive Disorder (OCD)Yousef A. MehdawiNo ratings yet
- Hemodynamic Disorders II: Components of Normal HemostasisDocument129 pagesHemodynamic Disorders II: Components of Normal HemostasisYousef A. MehdawiNo ratings yet
- Cushing's Disease: Pathobiology, Diagnosis, and ManagementDocument14 pagesCushing's Disease: Pathobiology, Diagnosis, and ManagementYousef A. MehdawiNo ratings yet
- Chapter 15 ANSDocument40 pagesChapter 15 ANSYousef A. MehdawiNo ratings yet
- فلسطينية الفصل الثانيDocument35 pagesفلسطينية الفصل الثانيYousef A. MehdawiNo ratings yet
- Antimycobacterial Drugs GuideDocument14 pagesAntimycobacterial Drugs GuideYousef A. Mehdawi100% (1)
- Obsessive-Compulsive Disorder (OCD)Document16 pagesObsessive-Compulsive Disorder (OCD)Yousef A. MehdawiNo ratings yet
- Postpartum ToolkitDocument27 pagesPostpartum ToolkitYousef A. MehdawiNo ratings yet
- Homework-Medication (4) ScenarioDocument7 pagesHomework-Medication (4) ScenarioYousef A. MehdawiNo ratings yet
- Marriage and Divorce: An-Najah National UniversityDocument13 pagesMarriage and Divorce: An-Najah National UniversityYousef A. MehdawiNo ratings yet
- Nutrition and PregnancyDocument3 pagesNutrition and PregnancyYousef A. MehdawiNo ratings yet
- Postpartum ToolkitDocument27 pagesPostpartum ToolkitYousef A. MehdawiNo ratings yet
- Ethical Principles: Miss Samah IshtiehDocument99 pagesEthical Principles: Miss Samah IshtiehYousef A. MehdawiNo ratings yet
- Ethical Principles: Miss Samah IshtiehDocument99 pagesEthical Principles: Miss Samah IshtiehYousef A. MehdawiNo ratings yet
- Early Years and Childcare Safeguarding AuditDocument4 pagesEarly Years and Childcare Safeguarding AuditEarly Years Careers100% (1)
- Development Team: Analytical Chemistry PolarographyDocument18 pagesDevelopment Team: Analytical Chemistry PolarographyKanchanNo ratings yet
- CapecitabineDocument8 pagesCapecitabineLisa MarieNo ratings yet
- Different Surgical Modalities For Management of Postburn FL Exion Contracture of The ElbowDocument6 pagesDifferent Surgical Modalities For Management of Postburn FL Exion Contracture of The ElbowMadhuchandra HirehalliNo ratings yet
- Biomechinics PDFDocument8 pagesBiomechinics PDFImran KhanNo ratings yet
- STM - Merck Case AnswersDocument2 pagesSTM - Merck Case AnswersreetayanNo ratings yet
- Effectiveness of Breathing Exercise On Reducing Pain Perception and State Anxiety Among Primi ParturientsDocument8 pagesEffectiveness of Breathing Exercise On Reducing Pain Perception and State Anxiety Among Primi ParturientsPutra SpNo ratings yet
- The Prevention of Women & Children Repression Act 2000: A Study of Implementation Process From 2003 To 2013Document9 pagesThe Prevention of Women & Children Repression Act 2000: A Study of Implementation Process From 2003 To 2013Md. Abdul KarimNo ratings yet
- NAVAL Hot Tapping Tool User GuideDocument19 pagesNAVAL Hot Tapping Tool User GuidemarconelucenapereiraNo ratings yet
- Conveying Water Distribution SEODocument90 pagesConveying Water Distribution SEOmichelghanemNo ratings yet
- Emerging Foodborne Enteric Bacterial Pathogens: A ReviewDocument11 pagesEmerging Foodborne Enteric Bacterial Pathogens: A ReviewAngelica Alejandra De La Torre AnayaNo ratings yet
- Implementation of Swachh Bharat in MysoreDocument13 pagesImplementation of Swachh Bharat in MysoreDipyaman ChoudhuryNo ratings yet
- Yoga & Diet To Prevent DepressionDocument5 pagesYoga & Diet To Prevent DepressionDietician Mrunmayee DixitNo ratings yet
- Kristeva On Melanie Klein's "Oresteia"Document6 pagesKristeva On Melanie Klein's "Oresteia"danthetoasterNo ratings yet
- (IJCST-V11I6P5) :A.E.E. El-Alfi, M. E. A. Awad, F. A. A. KhalilDocument9 pages(IJCST-V11I6P5) :A.E.E. El-Alfi, M. E. A. Awad, F. A. A. KhalilEighthSenseGroupNo ratings yet
- Dowell's Price List 18.3.2022Document26 pagesDowell's Price List 18.3.2022Sunil WadekarNo ratings yet
- LV CB Catalogue PDFDocument260 pagesLV CB Catalogue PDFBoobesh Kumar SekarNo ratings yet
- Physics Investigatory Project Class 12Document12 pagesPhysics Investigatory Project Class 12shivanginirai7No ratings yet
- General Conditions of Contracts For NLNG 2018Document28 pagesGeneral Conditions of Contracts For NLNG 2018AF Dowell MirinNo ratings yet
- Papers Traducir CompletoDocument12 pagesPapers Traducir CompletoJuan Jesus Barreda TalaveraNo ratings yet
- Appendix VIII - Civil and Structural Scope of WorkDocument140 pagesAppendix VIII - Civil and Structural Scope of WorkjaganrajNo ratings yet
- Main Receiving Station PDFDocument8 pagesMain Receiving Station PDFPrakash Kumar0% (1)
- Rocket Motor Head-end Structural AnalysisDocument83 pagesRocket Motor Head-end Structural AnalysisRudra Sai SandeepNo ratings yet
- Comparing Food with Comparative AdjectivesDocument4 pagesComparing Food with Comparative AdjectivesLuisito GonzalezNo ratings yet
- 311970536Document1 page311970536Codrut RadantaNo ratings yet
- TECHNICAL DATA SHEET of RUST CONVERTERDocument1 pageTECHNICAL DATA SHEET of RUST CONVERTERArmando AballeNo ratings yet
- Fujitsu GeneralDocument51 pagesFujitsu GeneralZubair DarNo ratings yet
- Sound Level MeterDocument11 pagesSound Level MeterFityatal HasanahNo ratings yet
- Ramial Chipped Wood - A Basic Tool For Regenerating SoilsDocument15 pagesRamial Chipped Wood - A Basic Tool For Regenerating SoilsmrmiscNo ratings yet
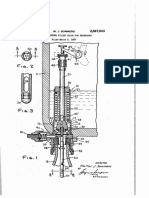
- Counter-pressure filler valve for beveragesDocument3 pagesCounter-pressure filler valve for beveragesbimalishaNo ratings yet