You might also like
- Fast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeFrom EverandFast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeNo ratings yet
- Operative Management of Anastomotic Leaks After Colorectal SurgeryDocument6 pagesOperative Management of Anastomotic Leaks After Colorectal SurgeryJorge OsorioNo ratings yet
- Chua 2012Document8 pagesChua 2012Devi DaryaningsihNo ratings yet
- Management of Colorectal Anastomotic Leakage-Differences Between Salvage and Anastomotic TakedownDocument6 pagesManagement of Colorectal Anastomotic Leakage-Differences Between Salvage and Anastomotic TakedownDumitru RadulescuNo ratings yet
- Curative Resection For Esophageal Adenocarcinoma: Analysis of 100 en Bloc EsophagectomiesDocument12 pagesCurative Resection For Esophageal Adenocarcinoma: Analysis of 100 en Bloc EsophagectomiesYacine Tarik AizelNo ratings yet
- Analysis of Long-Term Survivors After Surgical Resection For Pancreatic CancerDocument5 pagesAnalysis of Long-Term Survivors After Surgical Resection For Pancreatic CancermohamedNo ratings yet
- Proof: Gynecologic OncologyDocument2 pagesProof: Gynecologic OncologyCamilaBurgosNo ratings yet
- Systematized Management of Postoperative Enterocutaneous Fistulas. A 14 Years ExperienceDocument5 pagesSystematized Management of Postoperative Enterocutaneous Fistulas. A 14 Years ExperienceYacine Tarik AizelNo ratings yet
- Agaoglu2005 2Document6 pagesAgaoglu2005 2Ngo Quang MinhNo ratings yet
- No Está Claro Dar RT A Lo Bestia Sino Se CuraDocument7 pagesNo Está Claro Dar RT A Lo Bestia Sino Se Curaouf81No ratings yet
- Diffuse Malignant Peritoneal Mesothelioma PDFDocument9 pagesDiffuse Malignant Peritoneal Mesothelioma PDFAndreeaPopescuNo ratings yet
- Etiology of ECF Predicts OutcomeDocument5 pagesEtiology of ECF Predicts OutcomeYacine Tarik AizelNo ratings yet
- CA EsofágicoDocument45 pagesCA EsofágicoValeria ValdezNo ratings yet
- Surgical technique of coccygectomy: review of 28 studiesDocument7 pagesSurgical technique of coccygectomy: review of 28 studiesDiaz RandanilNo ratings yet
- Song 2017Document8 pagesSong 2017Patricia BezneaNo ratings yet
- Long-Term Outcomes of Primary Endoscopic Resection Vs Surgery For T1Document16 pagesLong-Term Outcomes of Primary Endoscopic Resection Vs Surgery For T1ellya zalfaNo ratings yet
- Refraction ManagementDocument8 pagesRefraction ManagementRaissaNo ratings yet
- Abdominoperineal Resection For Squamous Cell Anal Carcinoma: Survival and Risk Factors For RecurrenceDocument8 pagesAbdominoperineal Resection For Squamous Cell Anal Carcinoma: Survival and Risk Factors For RecurrenceWitrisyah PutriNo ratings yet
- Chevallay 2020Document17 pagesChevallay 2020Maria PalNo ratings yet
- J HPB 2016 02 489Document2 pagesJ HPB 2016 02 489hud6427No ratings yet
- 2022 GlS. Mid-term Efficacy of Surgical Treatments for Post-hysterectomy Vaginal Vault Prolapse; A Retrospective StudyDocument11 pages2022 GlS. Mid-term Efficacy of Surgical Treatments for Post-hysterectomy Vaginal Vault Prolapse; A Retrospective StudyJoseTeodomiroQuispeRicciNo ratings yet
- Glandula SalivarDocument8 pagesGlandula SalivarporsanimedNo ratings yet
- Histopathologic Features and Clinical Outcomes in 71 Cases of Bladder DiverticulaDocument6 pagesHistopathologic Features and Clinical Outcomes in 71 Cases of Bladder DiverticulaIrma Suriani DarwisNo ratings yet
- Tabrizi An 2009Document4 pagesTabrizi An 2009Dung Tran HoangNo ratings yet
- Infections After Laparoscopic and Open Cholecystectomy: Ceftriaxone Versus Placebo A Double Blind Randomized Clinical TrialDocument6 pagesInfections After Laparoscopic and Open Cholecystectomy: Ceftriaxone Versus Placebo A Double Blind Randomized Clinical TrialvivianmtNo ratings yet
- Rectal Cancer Partial VaginectomyDocument5 pagesRectal Cancer Partial VaginectomyArham ArsyadNo ratings yet
- Article. Loop Ileostomy Morbidity. Timing of Closure Matters.2006Document7 pagesArticle. Loop Ileostomy Morbidity. Timing of Closure Matters.2006Trí Cương NguyễnNo ratings yet
- MÁS RADIOTERAPIA SI RECAÍDA y Biopsia A Todos. 310 PersonasDocument13 pagesMÁS RADIOTERAPIA SI RECAÍDA y Biopsia A Todos. 310 Personasouf81No ratings yet
- Ojmn20120100002 97302300 2 PDFDocument5 pagesOjmn20120100002 97302300 2 PDFD s.No ratings yet
- Prognostic Value and Adverse Events of Cytoreductive Surgery With Hyperthermic Intraperitoneal Chemotherapy in Primary Advanced and PlatinumDocument14 pagesPrognostic Value and Adverse Events of Cytoreductive Surgery With Hyperthermic Intraperitoneal Chemotherapy in Primary Advanced and PlatinumChris El HadiNo ratings yet
- 203 FullDocument7 pages203 FullDonNo ratings yet
- Whole Ovary TransplantationDocument7 pagesWhole Ovary Transplantationari naNo ratings yet
- Wong 2017Document9 pagesWong 2017Mely GallardoNo ratings yet
- Neoadjuvant Chemoradiotherapy Followed by Surgery VersusDocument15 pagesNeoadjuvant Chemoradiotherapy Followed by Surgery VersusRaul Matute MartinNo ratings yet
- Original ArticleDocument9 pagesOriginal ArticlePatricia BezneaNo ratings yet
- Baek 2017Document10 pagesBaek 2017witaNo ratings yet
- Pi Is 1743919113001738Document5 pagesPi Is 1743919113001738Yacine Tarik AizelNo ratings yet
- Systemic Therapy For Advanced Appendiceal Adenocarcinoma: An Analysis From The NCCN Oncology Outcomes Database For Colorectal CancerDocument8 pagesSystemic Therapy For Advanced Appendiceal Adenocarcinoma: An Analysis From The NCCN Oncology Outcomes Database For Colorectal Canceralberto cabelloNo ratings yet
- Simultaneous Versus Delayed Resection For Initially Resectable Synchronous Colorectal Cancer Liver MetastasesDocument8 pagesSimultaneous Versus Delayed Resection For Initially Resectable Synchronous Colorectal Cancer Liver MetastasesDr Shiv ChopraNo ratings yet
- Hemdan 2014Document6 pagesHemdan 2014DavorIvanićNo ratings yet
- Jco 19 00337Document13 pagesJco 19 00337alberto cabelloNo ratings yet
- AppendicitisDocument3 pagesAppendicitisRindayu Julianti NurmanNo ratings yet
- Complications of Pancreatic SurgeryDocument5 pagesComplications of Pancreatic Surgeryhenok seifeNo ratings yet
- Kim 2009Document7 pagesKim 2009stefan ursuNo ratings yet
- Fit and Fecal Calprotectin 2020Document6 pagesFit and Fecal Calprotectin 2020sashadilanNo ratings yet
- Sattar M. Hashim JPMCDocument5 pagesSattar M. Hashim JPMCprastiaNo ratings yet
- cắt bỏ u xơ và thuyên tắc mạchDocument12 pagescắt bỏ u xơ và thuyên tắc mạchTiến Nguyễn VănNo ratings yet
- 2007-03 - Intestinal Autotransplantation For Adenocarcinoma of Pancreas Involving The Mesenteric Root - Our Experience and Literature Review PDFDocument3 pages2007-03 - Intestinal Autotransplantation For Adenocarcinoma of Pancreas Involving The Mesenteric Root - Our Experience and Literature Review PDFNawzad SulayvaniNo ratings yet
- Gine 2Document9 pagesGine 2Cimpean SorinNo ratings yet
- Malignancies of The Colorectum and Anus in Solid Organ RecipientsDocument8 pagesMalignancies of The Colorectum and Anus in Solid Organ RecipientsDaniel Alfonso GamezNo ratings yet
- International Wound Journal - 2016 - Bobkiewicz - Management of Enteroatmospheric Fistula With Negative Pressure WoundDocument10 pagesInternational Wound Journal - 2016 - Bobkiewicz - Management of Enteroatmospheric Fistula With Negative Pressure WoundDiana Carolina RochaNo ratings yet
- A Propensity Score Matched Analysis of Open Versus Minimally Invasive Transthoracic Esophagectomy in The NetherlandsDocument8 pagesA Propensity Score Matched Analysis of Open Versus Minimally Invasive Transthoracic Esophagectomy in The NetherlandsLuca BellaioNo ratings yet
- Acs 06 02 167Document8 pagesAcs 06 02 167MixalisKaplanisNo ratings yet
- Obstetric Anal Sphincter Injury and Anal Incontinence Following Vaginal Birth PDFDocument11 pagesObstetric Anal Sphincter Injury and Anal Incontinence Following Vaginal Birth PDFaldyNo ratings yet
- Esofago Carvical Valmasoni 2018Document9 pagesEsofago Carvical Valmasoni 2018Carlos N. Rojas PuyolNo ratings yet
- Perforacion ColonosDocument5 pagesPerforacion ColonosKeyla barriosNo ratings yet
- Management Guidelines For Penetrating Abdominal Trauma: Walter L. Biffl and Ernest E. MooreDocument9 pagesManagement Guidelines For Penetrating Abdominal Trauma: Walter L. Biffl and Ernest E. MooreArsy Mira PertiwiNo ratings yet
- Unukovych 2016Document7 pagesUnukovych 2016jdavies231No ratings yet
- Evaluating Esophagectomy Complications Using International Consensus DefinitionsDocument7 pagesEvaluating Esophagectomy Complications Using International Consensus DefinitionsPaulo RoseroNo ratings yet
- Detection of A Story CCM1 Frameshift Mutation in A Chinese Language Han Loved Ones Using Numerous Cerebral Cavernous MalformationsmqjvuDocument2 pagesDetection of A Story CCM1 Frameshift Mutation in A Chinese Language Han Loved Ones Using Numerous Cerebral Cavernous Malformationsmqjvumapmaple2No ratings yet
- Blunt: To TheDocument9 pagesBlunt: To TheOanaDavidNo ratings yet
- Nutritio 2Document1 pageNutritio 2OanaDavidNo ratings yet
- 2017 Article 135Document7 pages2017 Article 135OanaDavidNo ratings yet
- Childhood Trauma PDFDocument21 pagesChildhood Trauma PDFOanaDavidNo ratings yet
- International Journal of Surgery: Levent Kaptanoglu, Necmi Kurt, Hasan Ediz SikarDocument5 pagesInternational Journal of Surgery: Levent Kaptanoglu, Necmi Kurt, Hasan Ediz SikarOanaDavidNo ratings yet
- Medical Hypotheses: SciencedirectDocument9 pagesMedical Hypotheses: SciencedirectOanaDavidNo ratings yet
- Renal Trauma in The West of Ireland - A Regional ReviewDocument7 pagesRenal Trauma in The West of Ireland - A Regional ReviewOanaDavidNo ratings yet
- 595 2013 Article 515Document6 pages595 2013 Article 515OanaDavidNo ratings yet
- WJG 19 9003 PDFDocument10 pagesWJG 19 9003 PDFTheodore LiwonganNo ratings yet
- Multiple TraumaDocument3 pagesMultiple TraumaOanaDavidNo ratings yet
- Tomita ScoreDocument11 pagesTomita ScoreMukharradhi NanzaNo ratings yet
- Cord Candea+cecDocument122 pagesCord Candea+cecOanaDavidNo ratings yet
- Mal Leo 2014Document10 pagesMal Leo 2014OanaDavidNo ratings yet
- Blunt TraumaDocument14 pagesBlunt TraumaOanaDavidNo ratings yet
- Mcdonnell 1998Document1 pageMcdonnell 1998OanaDavidNo ratings yet
- Martinez 2007Document8 pagesMartinez 2007Yacine Tarik AizelNo ratings yet
- Atlas of Vascular Surgery and Endovascular Therapy - Anatomy and Technique 1E 2014 PDF UnitedVRG 3 PDFDocument795 pagesAtlas of Vascular Surgery and Endovascular Therapy - Anatomy and Technique 1E 2014 PDF UnitedVRG 3 PDFOanaDavid100% (3)
- Knot Tying ManualDocument50 pagesKnot Tying ManualAdriana Vick100% (1)
- Anatomic Exposure in Vascular Surgery, 3E (2013) (PDF) (UnitedVRG)Document605 pagesAnatomic Exposure in Vascular Surgery, 3E (2013) (PDF) (UnitedVRG)Rafael Castillo85% (13)
- Pharmaceutical Issues When Crushing, Opening or Splitting Oral Dosage FormsDocument7 pagesPharmaceutical Issues When Crushing, Opening or Splitting Oral Dosage FormsMohamed OmerNo ratings yet
- Ali, B.H., Al Wabel, N., Blunden, G., 2005Document8 pagesAli, B.H., Al Wabel, N., Blunden, G., 2005Herzan MarjawanNo ratings yet
- Nursing Intervention Plan for Fracture PatientDocument2 pagesNursing Intervention Plan for Fracture PatientAce Dioso TubascoNo ratings yet
- HSRCDocument53 pagesHSRCAbhishek Kumar SharmaNo ratings yet
- Healthmedicinet Com II 2014 JunDocument320 pagesHealthmedicinet Com II 2014 JunHeal ThmedicinetNo ratings yet
- Oral SurgeryDocument40 pagesOral Surgeryshekinah echavezNo ratings yet
- IELTS Listening Practice Test 69Document17 pagesIELTS Listening Practice Test 69Daniel perez100% (3)
- 7 Types of Stretching ExercisesDocument11 pages7 Types of Stretching ExercisesCzarina RimallaNo ratings yet
- CystolithiasisDocument7 pagesCystolithiasisRaul Nocete100% (1)
- ICF and Guidelines - ComPsych v.2022Document5 pagesICF and Guidelines - ComPsych v.2022JAY JOB TabiNo ratings yet
- Landmark Trials Genitourinary CompilationDocument55 pagesLandmark Trials Genitourinary CompilationBhanuNo ratings yet
- Pilot Study of The Effectiveness of Butterfly Technique of SCENAR Therapy On Heart Rate VariabilityDocument7 pagesPilot Study of The Effectiveness of Butterfly Technique of SCENAR Therapy On Heart Rate VariabilityParallaxsterNo ratings yet
- The - Erlangen - Test - of - Activities - of - Daily - Living - in ADocument3 pagesThe - Erlangen - Test - of - Activities - of - Daily - Living - in Akwstas79No ratings yet
- Benefits of CuminDocument14 pagesBenefits of CumindhiraniaNo ratings yet
- Press-Kit iMuco-Gingival Recessions Version 2.0Document13 pagesPress-Kit iMuco-Gingival Recessions Version 2.0carcuacNo ratings yet
- Local Anaesthetic AgentsDocument21 pagesLocal Anaesthetic AgentsSuresh KumarNo ratings yet
- Airway ExamDocument7 pagesAirway ExamCharmaine LingdasNo ratings yet
- Review of Literature on Prevalence Studies of Diabetes and Prediabetes in IndiaDocument39 pagesReview of Literature on Prevalence Studies of Diabetes and Prediabetes in Indiapatan ShabanaNo ratings yet
- NEW Tugas Dr. Ahmad Ridwan, MO, MSC 2Document36 pagesNEW Tugas Dr. Ahmad Ridwan, MO, MSC 2dr.rinanovitriani94No ratings yet
- Homework Week 2Document3 pagesHomework Week 2Niki100% (2)
- Desmopressin Full Prescribing Information, Dosage & Side Effects MIMS - Com IndonesiaDocument2 pagesDesmopressin Full Prescribing Information, Dosage & Side Effects MIMS - Com IndonesiayokiduarsaNo ratings yet
- Accepted Manuscript: Complementary Therapies in MedicineDocument24 pagesAccepted Manuscript: Complementary Therapies in MedicineAndrea BarresiNo ratings yet
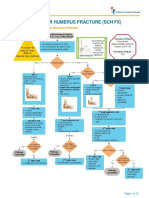
- Fracture Supracondylar HumerusDocument12 pagesFracture Supracondylar HumeruskemsNo ratings yet
- Disinfection by Sodium Hypochlorite. Dialysis Applications (2007)Document168 pagesDisinfection by Sodium Hypochlorite. Dialysis Applications (2007)Popoviciu SimonaNo ratings yet
- Psych - Chapters 11, 12, 13, and 14 Test Study GuideDocument5 pagesPsych - Chapters 11, 12, 13, and 14 Test Study Guidejustinaw1024No ratings yet
- Retrospective Study of Cholangiocarcinomas Diagnosed in The Hospital of Fuenlabrada in The Period 20062016Document3 pagesRetrospective Study of Cholangiocarcinomas Diagnosed in The Hospital of Fuenlabrada in The Period 20062016Riya CassendraNo ratings yet
- SpirulinaDocument57 pagesSpirulinaMarcus Gibson100% (4)
- 2019 Complication After Epilepsy Surgery AChA InfarctDocument7 pages2019 Complication After Epilepsy Surgery AChA InfarctSafitri MuhlisaNo ratings yet
- Drug To Drug InteractionDocument47 pagesDrug To Drug InteractionMannan SokaNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (17)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Algorithms to Live By: The Computer Science of Human DecisionsFrom EverandAlgorithms to Live By: The Computer Science of Human DecisionsRating: 4.5 out of 5 stars4.5/5 (722)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)