You might also like
- Concise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryFrom EverandConcise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryNo ratings yet
- Dental PPO30 - 2017Document2 pagesDental PPO30 - 2017SporkleNo ratings yet
- Dental PPO20 - 2017Document2 pagesDental PPO20 - 2017SporkleNo ratings yet
- Dental Plans and Rates: Bay AreaDocument6 pagesDental Plans and Rates: Bay AreaJDanaNo ratings yet
- Snap Guardian Dental Plan Summary 2022Document4 pagesSnap Guardian Dental Plan Summary 2022Samson FungNo ratings yet
- 2017 DgldmetDocument5 pages2017 DgldmetLucas FrançaNo ratings yet
- Generic Open Enrollment KitDocument22 pagesGeneric Open Enrollment KitSteve BarrowsNo ratings yet
- 2011 Delta Dental General MarketingDocument1 page2011 Delta Dental General MarketingKristieNo ratings yet
- 2020 Schedule of Benefits (SOB) - PPODocument26 pages2020 Schedule of Benefits (SOB) - PPOMonica LeeNo ratings yet
- TeamCare DentalDocument8 pagesTeamCare DentalHector FloydNo ratings yet
- Safari - Mar 11, 2019 at 11:00 PM PDFDocument1 pageSafari - Mar 11, 2019 at 11:00 PM PDFjohn jugoNo ratings yet
- Unitedhealthcare Dental Ppo Plan 2022 Summary of Benefits and CoverageDocument1 pageUnitedhealthcare Dental Ppo Plan 2022 Summary of Benefits and CoverageAdam CliftonNo ratings yet
- Benefit at A GlanceDocument2 pagesBenefit at A GlanceShiv ChauhanNo ratings yet
- Everyday Extras: Get The Same Amount Back Each Time You VisitDocument2 pagesEveryday Extras: Get The Same Amount Back Each Time You Visitfrank.wangNo ratings yet
- Health & Dental Handout JUN17Document2 pagesHealth & Dental Handout JUN17Darius YangNo ratings yet
- Premier 2000 NWDocument2 pagesPremier 2000 NWacolyteNo ratings yet
- HCF Mid ExtrasDocument3 pagesHCF Mid Extrasnoneother2No ratings yet
- Dental BS Delta 1500 PPO Benefit Summary 2018Document4 pagesDental BS Delta 1500 PPO Benefit Summary 2018deepchaitanyaNo ratings yet
- MCS Classicare (MA) Dental Coverage SummaryDocument4 pagesMCS Classicare (MA) Dental Coverage SummaryJessicaNo ratings yet
- Employee Benefits-Wellness Guide 2023-24Document30 pagesEmployee Benefits-Wellness Guide 2023-24shanzeh2609No ratings yet
- 2021 - Life, Dental, Vision PacketDocument12 pages2021 - Life, Dental, Vision PacketEberNo ratings yet
- 2021 GemPlan Summary of BenefitsDocument53 pages2021 GemPlan Summary of BenefitsRaja Churchill DassNo ratings yet
- RES000988105Document10 pagesRES000988105Leonardo MbangataNo ratings yet
- Star Out Patient Care Insurance PolicyV 1.0may2023Document37 pagesStar Out Patient Care Insurance PolicyV 1.0may2023ठाकुर सूरज राणाNo ratings yet
- Disclaimer: Trinet Is The Single-Employer Sponsor of All Its Benefit Plans. This Communication Is For Informational PurposesDocument26 pagesDisclaimer: Trinet Is The Single-Employer Sponsor of All Its Benefit Plans. This Communication Is For Informational PurposesJosh JasperNo ratings yet
- Barclays Dental Plan BenefitsDocument6 pagesBarclays Dental Plan Benefitssaksham23No ratings yet
- 2022 1027 Ahs SD 1058-1 BroDocument8 pages2022 1027 Ahs SD 1058-1 BroFernanda VargasNo ratings yet
- Gyll Aaron Insurance Verification 1654900113Document2 pagesGyll Aaron Insurance Verification 1654900113Jean Alyssa Mae CalingacionNo ratings yet
- 2010 UHC Medical Plan ComparisonDocument2 pages2010 UHC Medical Plan Comparisonapi-20618861No ratings yet
- HCF Lifestyle ExtrasDocument3 pagesHCF Lifestyle ExtrasMintNo ratings yet
- Care Freedom For DiabtiesDocument25 pagesCare Freedom For DiabtiesAgile ServicesNo ratings yet
- Brochure PDF MANHATTHAN LIFEDocument2 pagesBrochure PDF MANHATTHAN LIFEEmanuel ChirinosNo ratings yet
- Basic ExtrasDocument4 pagesBasic ExtrasDave SatterthwaiteNo ratings yet
- Vanderbilt phf-21-22Document2 pagesVanderbilt phf-21-22api-458468763No ratings yet
- Benefits HighlightsDocument1 pageBenefits HighlightsRobert AvramescuNo ratings yet
- Vision Highlight Sheet for Bugatchi Group, IncDocument3 pagesVision Highlight Sheet for Bugatchi Group, Incdayron ruizNo ratings yet
- Medical Cover Guide-2Document5 pagesMedical Cover Guide-2Temitope AdelowoNo ratings yet
- Cash Plan 100 Table+of+coverDocument8 pagesCash Plan 100 Table+of+covermuthukumaran.tdr2969No ratings yet
- Compare leading SA medical schemes' primary healthcare benefitsDocument5 pagesCompare leading SA medical schemes' primary healthcare benefitsMNQOBINo ratings yet
- Pet Care PlanDocument1 pagePet Care PlanAnonymous ZgY35hGNo ratings yet
- Day2day Care Brochure 2021Document6 pagesDay2day Care Brochure 2021hiteshmohakar15No ratings yet
- 2020 US Benefits OverviewDocument5 pages2020 US Benefits OverviewrdmNo ratings yet
- Special Care and Adultbasic: Comparison ChartDocument1 pageSpecial Care and Adultbasic: Comparison ChartjhsmalankaNo ratings yet
- Arogya - One Pager - Version 1.0 April 2020Document1 pageArogya - One Pager - Version 1.0 April 2020Ari BanerjeeNo ratings yet
- Arogya Sanjeevani - One Pager PDFDocument1 pageArogya Sanjeevani - One Pager PDFstar health Vadavalli50% (2)
- Arogya Sanjeevani Policy ParametersDocument1 pageArogya Sanjeevani Policy Parametersstar health Vadavalli0% (1)
- Compare Silver and Gold Health Insurance Plans Under 40 CharactersDocument4 pagesCompare Silver and Gold Health Insurance Plans Under 40 CharactersMitra LalNo ratings yet
- MCI One Pager Version 1.0 Oct 2020Document1 pageMCI One Pager Version 1.0 Oct 2020naval730107No ratings yet
- 2022 Steven Charles BAG - CODocument4 pages2022 Steven Charles BAG - COAlejuanchis Kamacho GarciaNo ratings yet
- Medical Aid Guide for International StudentsDocument5 pagesMedical Aid Guide for International StudentsmakjnrNo ratings yet
- 2020 Ankura Benefits GuideDocument20 pages2020 Ankura Benefits GuidegpperkNo ratings yet
- Benefits DetailDocument2 pagesBenefits DetailMJ SkyNo ratings yet
- Slater Inc Dental EnglishDocument4 pagesSlater Inc Dental Englishapi-531507901No ratings yet
- HCF Starter Extras With OpticalDocument3 pagesHCF Starter Extras With OpticalMike LatterNo ratings yet
- First Help PlanDocument1 pageFirst Help PlanIvan QuevedoNo ratings yet
- AISD - Dental - Cigna - PPO & HMO Plan Information - 2019-2020Document1 pageAISD - Dental - Cigna - PPO & HMO Plan Information - 2019-2020Jordin TumlinsonNo ratings yet
- Bon ClassicDocument12 pagesBon ClassicJonathan BorleyNo ratings yet
- Dental Plan Side-By-Side Comparison: Fast FactsDocument2 pagesDental Plan Side-By-Side Comparison: Fast FactsellenNo ratings yet
- Corporate Subscription Profile - TaskarDocument5 pagesCorporate Subscription Profile - TaskarPrasoon PalNo ratings yet
- IRIDA ANGJELI - DandHDistributing - Fall2011Document27 pagesIRIDA ANGJELI - DandHDistributing - Fall2011studentATtempleNo ratings yet
- Johnnysresume 342625865946954Document1 pageJohnnysresume 342625865946954Johnny CallananNo ratings yet
- Blood Hunter (3) Gladiator: Longtooth Shifter Chaotic Neutral 900Document3 pagesBlood Hunter (3) Gladiator: Longtooth Shifter Chaotic Neutral 900Johnny CallananNo ratings yet
- Blood Hunter (3) Gladiator: Longtooth Shifter Chaotic Neutral 2700Document3 pagesBlood Hunter (3) Gladiator: Longtooth Shifter Chaotic Neutral 2700Johnny CallananNo ratings yet
- ATF Guidance - Do I Need A License To Buy and Sell FirearmsDocument15 pagesATF Guidance - Do I Need A License To Buy and Sell Firearmspaul weich100% (1)
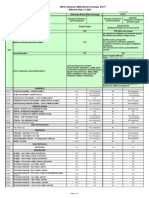
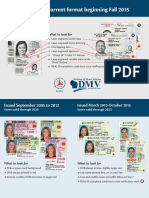
- Wisconsin's Current Format Beginning Fall 2015: What To Look ForDocument2 pagesWisconsin's Current Format Beginning Fall 2015: What To Look ForJohnny CallananNo ratings yet
- 4 Step Technique To Tame Emotional PainDocument2 pages4 Step Technique To Tame Emotional PainJohnny CallananNo ratings yet
- Culture and DevelopmentDocument16 pagesCulture and DevelopmentGrupo Chaski / Stefan Kaspar100% (1)
- Tadpole HusbandryDocument7 pagesTadpole HusbandryJohnny CallananNo ratings yet
- Policy Crime Definitions ExportDocument161 pagesPolicy Crime Definitions ExportJohnny CallananNo ratings yet
- Kat CoverDocument4 pagesKat CoverJohnny CallananNo ratings yet
- Kat CoverDocument4 pagesKat CoverJohnny CallananNo ratings yet
- Conditional Offer of EmploymentDocument2 pagesConditional Offer of EmploymentJohnny CallananNo ratings yet
- Column FootingDocument57 pagesColumn Footingnuwan01100% (7)
- Waste Management in Vienna. MA 48Document12 pagesWaste Management in Vienna. MA 484rtttt4ttt44No ratings yet
- Packaging Materials and Handling Technique: Dr. Ranjeet SinghDocument48 pagesPackaging Materials and Handling Technique: Dr. Ranjeet Singharon demagiba100% (1)
- Jean NouvelDocument1 pageJean Nouvelc.sioson.540553No ratings yet
- Mec 323Document68 pagesMec 323VINAY B.SNo ratings yet
- GypsumDocument79 pagesGypsumMansi GirotraNo ratings yet
- Mechanical Design of Turine EginesDocument51 pagesMechanical Design of Turine EginessriniNo ratings yet
- Final Nasir GlassDocument57 pagesFinal Nasir GlassShuvo Taufiq Ahmed100% (2)
- Assignment in English Plus Core 11 Full CircleDocument76 pagesAssignment in English Plus Core 11 Full CircleRitu Maan68% (38)
- Logicroof V-RP enDocument1 pageLogicroof V-RP enCristina DogariNo ratings yet
- LEEA-036 (B) - Academy ITS Practical Training Courses Jan - June 2020 Version 1 October 2019Document18 pagesLEEA-036 (B) - Academy ITS Practical Training Courses Jan - June 2020 Version 1 October 2019kaito kurabaNo ratings yet
- Practical 7 - Angiosperms Marking Guide Exercise 1: Class DicotyledonsDocument3 pagesPractical 7 - Angiosperms Marking Guide Exercise 1: Class DicotyledonsDitiro Maletsanake50% (2)
- Belazo Elastomeric Roof PaintDocument2 pagesBelazo Elastomeric Roof PaintrumahsketchNo ratings yet
- Understanding Revit Architecture - BeginnersDocument56 pagesUnderstanding Revit Architecture - BeginnersBudega100% (95)
- Quest The Last RemnantDocument67 pagesQuest The Last Remnantding suheNo ratings yet
- A Drop of Blood: Casting Time Range Components Duration Casting Time Range Components DurationDocument6 pagesA Drop of Blood: Casting Time Range Components Duration Casting Time Range Components DurationCristobal RencoretNo ratings yet
- Line Pack Presentation - Dec 2018Document7 pagesLine Pack Presentation - Dec 2018Goran JakupovićNo ratings yet
- Medical Terminology TermsDocument28 pagesMedical Terminology TermsNikka Moreen DagdagNo ratings yet
- Exercitii AdjectivDocument3 pagesExercitii AdjectivFirma GSCNo ratings yet
- Principles of Marketing - Product, Service and Experience DifferencesDocument26 pagesPrinciples of Marketing - Product, Service and Experience DifferencesVivien Leigh LopezNo ratings yet
- management of burns readingDocument28 pagesmanagement of burns readinghimanshugupta811997No ratings yet
- Essay Writing-PTEDocument13 pagesEssay Writing-PTEAnita GajjarNo ratings yet
- Fi & EiDocument3 pagesFi & EiPrasanna S Kulkarni100% (1)
- Dog Cake Recipe For Dozer's Birthday! - RecipeTin EatsDocument36 pagesDog Cake Recipe For Dozer's Birthday! - RecipeTin EatsZyreen Kate CataquisNo ratings yet
- Bathymetry and Its Applications PDFDocument158 pagesBathymetry and Its Applications PDFArseni MaximNo ratings yet
- Ahmed Ali Alshehri Mobile 00966-508-217284 Address: P.O.Box 70132 Zipcode:31952 Riyadh Street, Al-Khobar, Saudi ArabiaDocument9 pagesAhmed Ali Alshehri Mobile 00966-508-217284 Address: P.O.Box 70132 Zipcode:31952 Riyadh Street, Al-Khobar, Saudi ArabiaShah KhalidNo ratings yet
- 3 Sample Warranty: Sun Control Window FilmDocument1 page3 Sample Warranty: Sun Control Window FilmJanan AhmadNo ratings yet
- Flow Forming PresentatiionDocument24 pagesFlow Forming PresentatiionSrinivas Ds100% (1)
- Flange Insulation Sets: Technical SpecificationDocument6 pagesFlange Insulation Sets: Technical SpecificationNor Azlan AwangNo ratings yet
- Pres. Quirino Treasured Child School, Inc.: Grade 8-St. Joseph & ST MatthewDocument2 pagesPres. Quirino Treasured Child School, Inc.: Grade 8-St. Joseph & ST MatthewChristian jade QuijanoNo ratings yet