You might also like
- Lost at School: Points To PonderDocument59 pagesLost at School: Points To PonderMeridyth Taylor100% (2)
- The Prevalence MotherSon IncestDocument2 pagesThe Prevalence MotherSon Incestrizal2u60% (20)
- Matthew Clayton, Andrew Williams (Editors) - The Ideal of Equality-Palgrave Macmillan (2000)Document270 pagesMatthew Clayton, Andrew Williams (Editors) - The Ideal of Equality-Palgrave Macmillan (2000)begüm çelebiNo ratings yet
- Acute Diabetic Ketoacidosis (DKA)Document21 pagesAcute Diabetic Ketoacidosis (DKA)Madhu Sudhan Pandeya0% (1)
- Diabetic KetoacidosisDocument38 pagesDiabetic KetoacidosisAwatef AbushhiwaNo ratings yet
- Glucose PDFDocument1 pageGlucose PDFjef1234321100% (1)
- Diabetic Ketoacidosis PathwayDocument22 pagesDiabetic Ketoacidosis PathwaySri Nath100% (1)
- DKA ModifiedDocument25 pagesDKA ModifiedSujit KoiralaNo ratings yet
- SOAPM Alfonso GiulianiDocument2 pagesSOAPM Alfonso GiulianiEric YoungNo ratings yet
- BIMC Adult DKA Protocol 2012Document5 pagesBIMC Adult DKA Protocol 2012djizhieeNo ratings yet
- Kasus:: Dka: Keton 5 Meq/L, Blood Glucose 250, PH 7.3, Ketonemia and Ketonuria, Serum Bicarbonate 18 Meq/L or LessDocument3 pagesKasus:: Dka: Keton 5 Meq/L, Blood Glucose 250, PH 7.3, Ketonemia and Ketonuria, Serum Bicarbonate 18 Meq/L or LessSatya WangsaNo ratings yet
- DKA Management Protocol - Docx PaulosDocument3 pagesDKA Management Protocol - Docx PaulosMiraf MesfinNo ratings yet
- Revised DKA 2015 PDFDocument6 pagesRevised DKA 2015 PDFDr AhmedNo ratings yet
- Diabetic EmergenciesDocument65 pagesDiabetic EmergenciesManmeet SNo ratings yet
- Adult: Diabetic Emergencies: Care Protocol and ChartDocument4 pagesAdult: Diabetic Emergencies: Care Protocol and ChartvladhdNo ratings yet
- Guidelines For Management of Diabetes MellitusDocument1 pageGuidelines For Management of Diabetes MellitusthapanNo ratings yet
- Dka CmeDocument32 pagesDka CmeAizura Abdul AzizNo ratings yet
- Early Symptoms: Insidious Increase in Polydipsia and PolyuriaDocument3 pagesEarly Symptoms: Insidious Increase in Polydipsia and Polyuriabes3rkerNo ratings yet
- Diabetic KetoacidosisDocument22 pagesDiabetic KetoacidosispoktaviantiNo ratings yet
- DKAPPTxDocument34 pagesDKAPPTxMuhammad FurqanNo ratings yet
- Kegawatdaruratan Bidang Ilmu Penyakit Dalam: I.Penyakit Dalam - MIC/ICU FK - UNPAD - RS DR - Hasan Sadikin BandungDocument47 pagesKegawatdaruratan Bidang Ilmu Penyakit Dalam: I.Penyakit Dalam - MIC/ICU FK - UNPAD - RS DR - Hasan Sadikin BandungEfa FathurohmiNo ratings yet
- 003 DkaDocument9 pages003 DkaMohammedNo ratings yet
- Diabetic Ketoacidosis IntanDocument60 pagesDiabetic Ketoacidosis Intandesi susantiNo ratings yet
- Diabetic Ketoacidosis2Document2 pagesDiabetic Ketoacidosis2Venkat RamanNo ratings yet
- DKA Concepts and ManagementDocument22 pagesDKA Concepts and ManagementMohammad AliNo ratings yet
- Guidelines in The Treatment of Hyper Osmolar Non Ketotic Coma (Honk)Document4 pagesGuidelines in The Treatment of Hyper Osmolar Non Ketotic Coma (Honk)picassowaffleNo ratings yet
- Dka ProtocolDocument3 pagesDka ProtocolRed DevilNo ratings yet
- Hyperglycemia, HHS, DKADocument30 pagesHyperglycemia, HHS, DKAFirdausNo ratings yet
- Diabetic Ketoacidosis (D.K.A) Beaumont Hospital Protocol: DiagnosisDocument1 pageDiabetic Ketoacidosis (D.K.A) Beaumont Hospital Protocol: Diagnosislouglee9174100% (1)
- Dka-Hhs Topic DiscussionDocument2 pagesDka-Hhs Topic Discussionapi-648401824No ratings yet
- DKA Protocol TGDocument11 pagesDKA Protocol TGabelNo ratings yet
- Diabetic Ketoacidosis (DKA) - Presentation Slide EditedDocument22 pagesDiabetic Ketoacidosis (DKA) - Presentation Slide EditedTerence Chin0% (1)
- Diabetic KetoasidosisDocument33 pagesDiabetic KetoasidosisGrace UlyNo ratings yet
- New Format MasterDocument34 pagesNew Format MasterMuhammad FurqanNo ratings yet
- Diabetic Ketoacidosis (Dka) & Hyperosmolar Hyperglycemic Syndrome (HHS)Document54 pagesDiabetic Ketoacidosis (Dka) & Hyperosmolar Hyperglycemic Syndrome (HHS)Beyene FelekeNo ratings yet
- Clinical Order Set DKA AdultDocument2 pagesClinical Order Set DKA AdultBashar Al-HamaidehNo ratings yet
- DKA AssignmentDocument4 pagesDKA AssignmentHisham ShahinNo ratings yet
- สำเนา draft1 - DKA 1Document42 pagesสำเนา draft1 - DKA 1teddypor100% (1)
- Ketosis DMDocument33 pagesKetosis DMtiaNo ratings yet
- IvfDocument16 pagesIvfJohnRev Fundal Lopez LorenzoNo ratings yet
- Seminar Presentation On Management of Diabetic Ketoacidosis BY:Kelil Kedir (CII)Document34 pagesSeminar Presentation On Management of Diabetic Ketoacidosis BY:Kelil Kedir (CII)Meraol HusseinNo ratings yet
- Pediatric Diabetic Ketoacidosis (DKA) Algorithm (Page 1-ED) : DKA Diagnosed DKA Not DiagnosedDocument2 pagesPediatric Diabetic Ketoacidosis (DKA) Algorithm (Page 1-ED) : DKA Diagnosed DKA Not Diagnosedrolland_arrizaNo ratings yet
- Comer Emergency Department (ED) Clinical Guidelines: Diabetic Ketoacidosis (DKA) - Moderately Severe To SevereDocument6 pagesComer Emergency Department (ED) Clinical Guidelines: Diabetic Ketoacidosis (DKA) - Moderately Severe To SevereChristelle Malaluan CalumpitNo ratings yet
- ED Module 4Document26 pagesED Module 4Washi AkunNo ratings yet
- Laki-Laki, 21 Tahun Dengan Ketoasidosis DiabetikumDocument66 pagesLaki-Laki, 21 Tahun Dengan Ketoasidosis DiabetikumAnonymous gudRSKNo ratings yet
- Diabetic Ketoacidosis Acute Management: A State of Absolute Insulin BankruptcyDocument24 pagesDiabetic Ketoacidosis Acute Management: A State of Absolute Insulin BankruptcyGwEn LimNo ratings yet
- Dka Dan HHS: Oleh: Tri Adiatmoko Hervi LaksariDocument20 pagesDka Dan HHS: Oleh: Tri Adiatmoko Hervi Laksarisunaryo lNo ratings yet
- Dr. Ashraf Hussein Ismail E.R Consultant, PSHDocument17 pagesDr. Ashraf Hussein Ismail E.R Consultant, PSHAshraf HusseinNo ratings yet
- Acute Complication of Diabetes Mellitus: Laksmi SasiariniDocument43 pagesAcute Complication of Diabetes Mellitus: Laksmi SasiariniClararida RiawanNo ratings yet
- Diabetic Ketoacidosis (DKA) : BackgroundDocument7 pagesDiabetic Ketoacidosis (DKA) : BackgroundLeoNo ratings yet
- Diabetic KetoacidosisDocument10 pagesDiabetic Ketoacidosisagar agarNo ratings yet
- Diabetic Emergencies Case StudiesDocument32 pagesDiabetic Emergencies Case StudiesLamria Maloni Siahaan0% (1)
- Type 1 Diabetes Mellitus and Diabetic Ketoacidosis (Pediatrics)Document26 pagesType 1 Diabetes Mellitus and Diabetic Ketoacidosis (Pediatrics)Sheharyar AjmalNo ratings yet
- Kad HHS 2019Document35 pagesKad HHS 2019Friska RamadayantiNo ratings yet
- Nursing Care Plan: Fluid Volume Deficit R/T Active Fluid Loss (Increased Urine Output)Document9 pagesNursing Care Plan: Fluid Volume Deficit R/T Active Fluid Loss (Increased Urine Output)Gayu Patel100% (2)
- Nursing Care Plan: Fluid Volume Deficit R/T Active Fluid Loss (Increased Urine Output)Document9 pagesNursing Care Plan: Fluid Volume Deficit R/T Active Fluid Loss (Increased Urine Output)Gayu Patel0% (1)
- Nursing Care Plan: Fluid Volume Deficit R/T Active Fluid Loss (Increased Urine Output)Document9 pagesNursing Care Plan: Fluid Volume Deficit R/T Active Fluid Loss (Increased Urine Output)ghellersNo ratings yet
- Diabetic Ketoacidosis: Clinical Features and Management: - DR Sanjay Kalra, D.M. (Aiims)Document26 pagesDiabetic Ketoacidosis: Clinical Features and Management: - DR Sanjay Kalra, D.M. (Aiims)Siti RahmahNo ratings yet
- Dka NewDocument37 pagesDka NewMuhammad FurqanNo ratings yet
- Diabetic Emergencies: 1. Diabetic Ketoacidosis 2. Hyperglycemic Hyperosmolar State 3. HypoglycemiaDocument24 pagesDiabetic Emergencies: 1. Diabetic Ketoacidosis 2. Hyperglycemic Hyperosmolar State 3. HypoglycemiachooNo ratings yet
- Shelly DKADocument18 pagesShelly DKARizkyastari OnnyNo ratings yet
- Management of Anesthesia: Diabetes MellitusDocument29 pagesManagement of Anesthesia: Diabetes MellitusHari PrasadNo ratings yet
- Diabetic Nephropathy, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDiabetic Nephropathy, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Understanding Basics of EKG: by Alula A. (R III)Document37 pagesUnderstanding Basics of EKG: by Alula A. (R III)sky nutsNo ratings yet
- Cardiology Handbook Gondar University Hospital: Management GuidelinesDocument42 pagesCardiology Handbook Gondar University Hospital: Management Guidelinessky nutsNo ratings yet
- Management Protocol of Septic Shock: DiagnosisDocument3 pagesManagement Protocol of Septic Shock: Diagnosissky nutsNo ratings yet
- Pneumonia Management ProtocolDocument2 pagesPneumonia Management Protocolsky nuts100% (1)
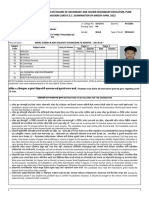
- Maharashtra State Board of Secondary and Higher Secondary Education, Pune Admission Card H.S.C. Examination of March-April 2022Document3 pagesMaharashtra State Board of Secondary and Higher Secondary Education, Pune Admission Card H.S.C. Examination of March-April 2022PANKAJ WANDHARENo ratings yet
- Questions and AnswerDocument5 pagesQuestions and AnswerPatricia Camille Ponce JonghunNo ratings yet
- Psychological Test in Counselling (New)Document35 pagesPsychological Test in Counselling (New)Shiek LukmanNo ratings yet
- ADMISSIONDocument28 pagesADMISSIONDewi AyuNo ratings yet
- 05 ING B1 Comprension - Textos Escritos 22 23Document4 pages05 ING B1 Comprension - Textos Escritos 22 23BeatrizNo ratings yet
- Performance & Compensation ManagementDocument2 pagesPerformance & Compensation ManagementHijab FatimaNo ratings yet
- H2SO4 PekatDocument6 pagesH2SO4 PekatAnonymous SuC1rG72CNo ratings yet
- key đề thi hk2 khối 12 tự ôn tậpDocument17 pageskey đề thi hk2 khối 12 tự ôn tậpNgọc Khuê TrầnNo ratings yet
- Urban Mobility in Kathmandu: Status and TrendsDocument8 pagesUrban Mobility in Kathmandu: Status and TrendsAdwait LimayeNo ratings yet
- Holmes, A. G., Tuin, M. P., & Turner, S. L. (2021) - Competence and Competency in Higher EducationDocument14 pagesHolmes, A. G., Tuin, M. P., & Turner, S. L. (2021) - Competence and Competency in Higher Educationnadine.galinoNo ratings yet
- Company and Soft Tissue Regeneration ProductsDocument51 pagesCompany and Soft Tissue Regeneration ProductsPaulus LagadanNo ratings yet
- Asepsis GlovingDocument6 pagesAsepsis GlovingJeonoh FloridaNo ratings yet
- Fitness GuideDocument14 pagesFitness GuideĪt'sme VīkkyNo ratings yet
- NCfIH Fast Facts Respiratory Syncytial VirusDocument6 pagesNCfIH Fast Facts Respiratory Syncytial VirusIndiana Family to FamilyNo ratings yet
- Physical Education: Quarter 2 - Module 1 Active Recreation (Fitness)Document13 pagesPhysical Education: Quarter 2 - Module 1 Active Recreation (Fitness)쓰레기한국 팝No ratings yet
- EVALUATE Match Each Subfield of Psychology With The Issues or Questions Posed BelowDocument2 pagesEVALUATE Match Each Subfield of Psychology With The Issues or Questions Posed BelowAlexandra TorresNo ratings yet
- Kids Screen AdictionDocument3 pagesKids Screen AdictionNisal RukshanNo ratings yet
- M - Medications: Discharge PlanningDocument4 pagesM - Medications: Discharge Planningalynnavictoria100% (4)
- Manual For PGIMSDocument15 pagesManual For PGIMSAnanya SharmaNo ratings yet
- Nasopharyngeal AngiofibromaDocument51 pagesNasopharyngeal Angiofibromakamal saudNo ratings yet
- Dela Rosa 2A MCN-Module 04Document4 pagesDela Rosa 2A MCN-Module 04Atsu MiyaNo ratings yet
- Cognitive Learning TheoryDocument40 pagesCognitive Learning Theoryexia89No ratings yet
- Benefits of HijamaDocument3 pagesBenefits of HijamaBateria MeaNo ratings yet
- The Big Idea: WORKBOOK: The Three Rings - The REAL Secret To Long-Lasting SuccessDocument18 pagesThe Big Idea: WORKBOOK: The Three Rings - The REAL Secret To Long-Lasting SuccessAndré LuizNo ratings yet
- Jaundice PDFDocument7 pagesJaundice PDFSib AsuncionNo ratings yet
- Business ObjectiveDocument29 pagesBusiness ObjectiveRahul KumarNo ratings yet