You might also like
- Cosmetic Surgery An Interdisciplinary ApproachDocument1,004 pagesCosmetic Surgery An Interdisciplinary ApproachDaniel FilizzolaNo ratings yet
- Zimbabwe School Examinations Council: Physical Education, Sport & Mass Displays 4002/02Document8 pagesZimbabwe School Examinations Council: Physical Education, Sport & Mass Displays 4002/02Elton Maregere100% (7)
- Wound NoteDocument16 pagesWound NoteofasusiNo ratings yet
- 305.076.000 01 EN Bellavista Manual G6 PDFDocument162 pages305.076.000 01 EN Bellavista Manual G6 PDFanh khoa duongNo ratings yet
- SGOP cervical cancer guidelinesDocument93 pagesSGOP cervical cancer guidelinesjojolilimomo100% (2)
- Nursing Care Plan Urinary Tract Infection (UTI)Document2 pagesNursing Care Plan Urinary Tract Infection (UTI)deric95% (97)
- Apparently New Syndrome of Congenital Cataracts, Sensorineural Deafness, Down Syndrome-Like Facial Appearance, Short Stature, and Mental RetardationDocument5 pagesApparently New Syndrome of Congenital Cataracts, Sensorineural Deafness, Down Syndrome-Like Facial Appearance, Short Stature, and Mental Retardationjahfdfgsdjad asdhsajhajdkNo ratings yet
- SAMS: Provisionally Unique Multiple CongenitalDocument5 pagesSAMS: Provisionally Unique Multiple Congenitaljahfdfgsdjad asdhsajhajdkNo ratings yet
- Zimmerman-Laband Syndrome and Profound Mental RetardationDocument5 pagesZimmerman-Laband Syndrome and Profound Mental RetardationNorberto Singh Rios (Norbit)No ratings yet
- Delayed speech developmentDocument5 pagesDelayed speech developmentShakirullah KhanNo ratings yet
- Mental Retardation, Epilepsy, Short Stature, and Skeletal DysplasiaDocument3 pagesMental Retardation, Epilepsy, Short Stature, and Skeletal Dysplasiajahfdfgsdjad asdhsajhajdkNo ratings yet
- Smith 1999Document8 pagesSmith 1999smithl25No ratings yet
- Rimmer2008Document4 pagesRimmer2008Mili RiveraNo ratings yet
- Physiotherapy Treatment of Endemic Cretinism in New Guinea HighlandsDocument4 pagesPhysiotherapy Treatment of Endemic Cretinism in New Guinea Highlandsadilla kusumaNo ratings yet
- Dyscephalia Mandibulo-Oculo-Facialis SyndromeDocument5 pagesDyscephalia Mandibulo-Oculo-Facialis SyndromeReyes Ivan García CuevasNo ratings yet
- Sorge 1996Document4 pagesSorge 1996jahfdfgsdjad asdhsajhajdkNo ratings yet
- Acrofacial Dysostosis Report Confirms Rare Catania TypeDocument4 pagesAcrofacial Dysostosis Report Confirms Rare Catania TypeSergioFernandezNo ratings yet
- Mca/Mr: New Syndrome?Document3 pagesMca/Mr: New Syndrome?JoNo ratings yet
- HSS Clinical Pronostic ConsiderationDocument4 pagesHSS Clinical Pronostic ConsiderationReyes Ivan García CuevasNo ratings yet
- Loss of The N-Myc Oncogene in A Patient With A Small Interstitial Deletion of The Short Arm of ChromosomeDocument5 pagesLoss of The N-Myc Oncogene in A Patient With A Small Interstitial Deletion of The Short Arm of ChromosomeantonioopNo ratings yet
- Gracile Bone Dysplasia (American Journal of Medical Genetics, Vol. 75, Issue 1) (1998)Document6 pagesGracile Bone Dysplasia (American Journal of Medical Genetics, Vol. 75, Issue 1) (1998)mgNo ratings yet
- Plomp 1998Document7 pagesPlomp 1998dad dzd adaNo ratings yet
- Le Mire 2004Document2 pagesLe Mire 2004Fapuw ParawansaNo ratings yet
- Sibs With Anencephaly, Anophthalmia, Clefts, Omphalocele, and Polydactyly: Hydrolethalus orDocument4 pagesSibs With Anencephaly, Anophthalmia, Clefts, Omphalocele, and Polydactyly: Hydrolethalus orSarly FebrianaNo ratings yet
- Letter To The Editor: On Cognitive Variability in Velocardiofacial Syndrome: Profound Mental Retardation and AutismDocument2 pagesLetter To The Editor: On Cognitive Variability in Velocardiofacial Syndrome: Profound Mental Retardation and AutismHarshit AmbeshNo ratings yet
- Fryburg 1996Document4 pagesFryburg 1996q79uwsp608wafhq4mNo ratings yet
- Brief Clinical Report: The Floating Harbor Syndrome With Cardiac Septa1 DefectDocument3 pagesBrief Clinical Report: The Floating Harbor Syndrome With Cardiac Septa1 DefectSarly FebrianaNo ratings yet
- Sammito1988Document7 pagesSammito1988Aling AyenNo ratings yet
- Cla Eys 1997Document6 pagesCla Eys 1997jahfdfgsdjad asdhsajhajdkNo ratings yet
- Dental management of ALS patientDocument4 pagesDental management of ALS patientAline LoyolaNo ratings yet
- 495 FullDocument2 pages495 Fulltigtigrai49No ratings yet
- Hutchinson-Gilford Progeria Syndrome: Net CaseDocument4 pagesHutchinson-Gilford Progeria Syndrome: Net Casesario indriayaniNo ratings yet
- Teebi 1996Document4 pagesTeebi 1996JohnnyNo ratings yet
- Complete Trisomy 17p Syndrome in A Girl With Der (14) T (14 17) (p11.2 p11.2)Document8 pagesComplete Trisomy 17p Syndrome in A Girl With Der (14) T (14 17) (p11.2 p11.2)AldunIdhunNo ratings yet
- Three-Generation Family With Resemblance to Townes-Brocks Syndrome and Goldenhar SpectrumDocument6 pagesThree-Generation Family With Resemblance to Townes-Brocks Syndrome and Goldenhar SpectrumAndjela RoganovicNo ratings yet
- Human Kluver-Bucy: SyndromeDocument6 pagesHuman Kluver-Bucy: SyndromeFlorencia RubioNo ratings yet
- Beighton 1972Document7 pagesBeighton 1972fabielfabulosoNo ratings yet
- AMS PublishedDocument4 pagesAMS PublishedAyanawNo ratings yet
- Severe Facial Clefting, Limbic Dermoid, Hypoplasia of The Corpus Callosum, and Multiple Skin AppendagesDocument2 pagesSevere Facial Clefting, Limbic Dermoid, Hypoplasia of The Corpus Callosum, and Multiple Skin AppendagesJoNo ratings yet
- Final Case Report FinalDocument7 pagesFinal Case Report FinalPawan JarwalNo ratings yet
- Labrune 1997Document6 pagesLabrune 1997dad dzd adaNo ratings yet
- Ajmg A 34257 PDFDocument3 pagesAjmg A 34257 PDFdtf1007No ratings yet
- Tsukahara 1997Document5 pagesTsukahara 1997Narjes Sharif AskariNo ratings yet
- Al Ghamdi1997Document5 pagesAl Ghamdi1997JohnnyNo ratings yet
- Band Heterotopia in Zellweger Syndrome (Cerebro-Hepato Renal Syndrome)Document1 pageBand Heterotopia in Zellweger Syndrome (Cerebro-Hepato Renal Syndrome)ZazzZaffaNo ratings yet
- Archdisch01563 0108Document6 pagesArchdisch01563 0108jharmandoNo ratings yet
- Three Cases of Familial Clavicular HypoplasiaDocument4 pagesThree Cases of Familial Clavicular HypoplasiaSabrina JonesNo ratings yet
- Phenotypic Analysis of A Case of "3MC Syndrome" With Review of LiteratureDocument3 pagesPhenotypic Analysis of A Case of "3MC Syndrome" With Review of LiteratureBOHR International Journal of Current Research in Optometry and Ophthalmology (BIJCROO)No ratings yet
- Slowly Generahed: Progressive Aphasia Without DementiaDocument7 pagesSlowly Generahed: Progressive Aphasia Without Dementiajonas1808No ratings yet
- Confirmation of The Colobomatous Macrophthalmia With Microcornea SyndromeDocument3 pagesConfirmation of The Colobomatous Macrophthalmia With Microcornea SyndromeJeje SulivanNo ratings yet
- Facial Paralysis Causes and TreatmentsDocument4 pagesFacial Paralysis Causes and TreatmentsAlmeiliana Arruanpasau'No ratings yet
- Juvenile Metachromatic Leucodystrophy A Rare Case ReportDocument2 pagesJuvenile Metachromatic Leucodystrophy A Rare Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Autosomal Dominant Microcephaly With Normal Intelligence, Short Palpebral Fissures, and Digital AnomaliesDocument6 pagesAutosomal Dominant Microcephaly With Normal Intelligence, Short Palpebral Fissures, and Digital Anomaliesjahfdfgsdjad asdhsajhajdkNo ratings yet
- Loshkajian 1997Document6 pagesLoshkajian 1997Ali AmokraneNo ratings yet
- Complete Absence of Rib Ossification, Micrognathia and Ear Anomalies: Extreme Expression of Cerebro-Costo-Mandibular Syndrome?Document4 pagesComplete Absence of Rib Ossification, Micrognathia and Ear Anomalies: Extreme Expression of Cerebro-Costo-Mandibular Syndrome?Anonymous 0vDTRVnNo ratings yet
- Lerone 1997Document4 pagesLerone 1997Narjes Sharif AskariNo ratings yet
- Johnson 1996Document11 pagesJohnson 1996Ali AmokraneNo ratings yet
- Metabolic Genetic DiseasesDocument77 pagesMetabolic Genetic DiseasesZNo ratings yet
- Pina Neto1996Document3 pagesPina Neto1996smithl25No ratings yet
- (Sici) 1096 8628 (19981228) 80:5 454::aid Ajmg4 3.0.co 2 o PDFDocument5 pages(Sici) 1096 8628 (19981228) 80:5 454::aid Ajmg4 3.0.co 2 o PDFJaymel MaigueNo ratings yet
- Algoritmo diferencial de debilidad proximal en paciente con miopatia adquirida por nemalina.Document7 pagesAlgoritmo diferencial de debilidad proximal en paciente con miopatia adquirida por nemalina.Farid Santiago Abedrabbo LombeydaNo ratings yet
- Five New Cases and Review of Nine Previously Published CasesDocument8 pagesFive New Cases and Review of Nine Previously Published CasesBogdan SoptereanNo ratings yet
- Molecular and Clinical Aspects of Angelman SyndromeDocument13 pagesMolecular and Clinical Aspects of Angelman SyndromeAndres AngelettiNo ratings yet
- Presbycusis: J. R. Kearns, MDDocument5 pagesPresbycusis: J. R. Kearns, MDnick_mdNo ratings yet
- 0.3 MG 3 Times A Day HairDocument6 pages0.3 MG 3 Times A Day Hairlakshay kumarNo ratings yet
- Slavo Tine K 1996Document6 pagesSlavo Tine K 1996jahfdfgsdjad asdhsajhajdkNo ratings yet
- Walter 1996Document7 pagesWalter 1996jahfdfgsdjad asdhsajhajdkNo ratings yet
- Stockton 1997Document5 pagesStockton 1997jahfdfgsdjad asdhsajhajdkNo ratings yet
- Tons Gard 1997Document7 pagesTons Gard 1997jahfdfgsdjad asdhsajhajdkNo ratings yet
- Letter To The Editor: Not A New Seckel-Like Syndrome But Ear-Patella-Short Stature SyndromeDocument1 pageLetter To The Editor: Not A New Seckel-Like Syndrome But Ear-Patella-Short Stature Syndromejahfdfgsdjad asdhsajhajdkNo ratings yet
- Short Stature in A Mother and Daughter With Terminal Deletion of Xp22.3Document4 pagesShort Stature in A Mother and Daughter With Terminal Deletion of Xp22.3jahfdfgsdjad asdhsajhajdkNo ratings yet
- Silverman 1996Document10 pagesSilverman 1996jahfdfgsdjad asdhsajhajdkNo ratings yet
- Sorge 1996Document4 pagesSorge 1996jahfdfgsdjad asdhsajhajdkNo ratings yet
- Loss of The N-Myc Oncogene in A Patient With A Small Interstitial Deletion of The Short Arm of ChromosomeDocument5 pagesLoss of The N-Myc Oncogene in A Patient With A Small Interstitial Deletion of The Short Arm of ChromosomeantonioopNo ratings yet
- Autosomal Dominant Microcephaly With Normal Intelligence, Short Palpebral Fissures, and Digital AnomaliesDocument6 pagesAutosomal Dominant Microcephaly With Normal Intelligence, Short Palpebral Fissures, and Digital Anomaliesjahfdfgsdjad asdhsajhajdkNo ratings yet
- Reish 1996Document5 pagesReish 1996jahfdfgsdjad asdhsajhajdkNo ratings yet
- Reish 1996Document5 pagesReish 1996jahfdfgsdjad asdhsajhajdkNo ratings yet
- Familial Spastic Paraparesis: Evaluation of LocusDocument11 pagesFamilial Spastic Paraparesis: Evaluation of LocusBruno MotaNo ratings yet
- Ishikawa 1996Document6 pagesIshikawa 1996jahfdfgsdjad asdhsajhajdkNo ratings yet
- Inomata 1998Document3 pagesInomata 1998jahfdfgsdjad asdhsajhajdkNo ratings yet
- Ehara 1997Document9 pagesEhara 1997jahfdfgsdjad asdhsajhajdkNo ratings yet
- 10 1002@sici1096-86281997061370@3333@@aid-Ajmg243 0 Co2-L PDFDocument1 page10 1002@sici1096-86281997061370@3333@@aid-Ajmg243 0 Co2-L PDFjahfdfgsdjad asdhsajhajdkNo ratings yet
- Dig Ilio 1997Document3 pagesDig Ilio 1997jahfdfgsdjad asdhsajhajdkNo ratings yet
- Cla Eys 1997Document6 pagesCla Eys 1997jahfdfgsdjad asdhsajhajdkNo ratings yet
- 10 1002/ (Sici) 1096-8628 (19971219) 73:3 - 279::aid-Ajmg10 - 3 0 Co 2-g PDFDocument7 pages10 1002/ (Sici) 1096-8628 (19971219) 73:3 - 279::aid-Ajmg10 - 3 0 Co 2-g PDFNaesilla LiemNo ratings yet
- King 1997Document3 pagesKing 1997jahfdfgsdjad asdhsajhajdkNo ratings yet
- Cerumen ImpactionDocument9 pagesCerumen Impactionnnennachidera2002No ratings yet
- Meda QantasDocument12 pagesMeda QantasAviasiNo ratings yet
- Antibiotic Sensitivity TestDocument10 pagesAntibiotic Sensitivity TestJ.A. LauronNo ratings yet
- Pediatric Nursing Course OutlineDocument6 pagesPediatric Nursing Course OutlineDaryl Adrian RecaidoNo ratings yet
- Curriculum Vita1Document2 pagesCurriculum Vita1rajalashmiNo ratings yet
- The Fate of a BurgerDocument2 pagesThe Fate of a BurgerE ZeeNo ratings yet
- National Dengue Prevention Program OverviewDocument39 pagesNational Dengue Prevention Program OverviewkentNo ratings yet
- Tissue Response Under HyperpressureDocument8 pagesTissue Response Under HyperpressureCristhiane Rodrigues MaryNo ratings yet
- International Journal of Pharmaceutical Science Invention (IJPSI)Document6 pagesInternational Journal of Pharmaceutical Science Invention (IJPSI)inventionjournalsNo ratings yet
- Lilly's Donanemab Significantly Slowed Cognitive and Functional Decline in Phase 3 Study of Early Alzheimer's DiseaseDocument3 pagesLilly's Donanemab Significantly Slowed Cognitive and Functional Decline in Phase 3 Study of Early Alzheimer's DiseaseAna Cecília RizzuttiNo ratings yet
- Hervita - Depression and Anxiety Disorder Management in IndonesiaDocument30 pagesHervita - Depression and Anxiety Disorder Management in IndonesiaPrissilma TaniaNo ratings yet
- 2021 - СРРРРРРС - 3 Course - GM - EnglDocument17 pages2021 - СРРРРРРС - 3 Course - GM - EnglAiganym AmanovaNo ratings yet
- Forensic PsychiatryDocument5 pagesForensic PsychiatrySheba Dan de WiseNo ratings yet
- Demonstration On Chest Physiotherapy DefinitionDocument3 pagesDemonstration On Chest Physiotherapy Definitiondileep0% (1)
- Leann Li ResumeDocument2 pagesLeann Li Resumeapi-660140781No ratings yet
- Preliminaries of Reading and Writing For Academic and Professional PurposesDocument2 pagesPreliminaries of Reading and Writing For Academic and Professional PurposesMarielle RumbaoaNo ratings yet
- Causes of Status EpilepticusDocument12 pagesCauses of Status EpilepticusSergio MouraNo ratings yet
- MAPEH VI Lesson on ImmunizationDocument3 pagesMAPEH VI Lesson on ImmunizationEsteban JuanNo ratings yet
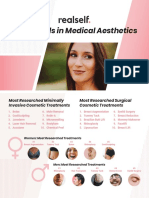
- RealSelf YearInReview OneSheetDocument2 pagesRealSelf YearInReview OneSheetDominico Adityo RaharjoNo ratings yet
- Department of Molecular Biology. Covid 19 Test Name Result Unit Bio. Ref. Range MethodDocument4 pagesDepartment of Molecular Biology. Covid 19 Test Name Result Unit Bio. Ref. Range Methodsourabhshrivastava80No ratings yet
- Random Blood Sugar Test AssignmentDocument1 pageRandom Blood Sugar Test AssignmentmadamcloudnineNo ratings yet
- CV DrmuneerDocument5 pagesCV DrmuneeridrisgaroodNo ratings yet
- Physiologic Changes in Pregnancy: 1. UterusDocument14 pagesPhysiologic Changes in Pregnancy: 1. UterusNiña Ricci MtflcoNo ratings yet
- No Proof of COVID19 Causality - Is This The Crime of The Century - Principia Scientific IntlDocument13 pagesNo Proof of COVID19 Causality - Is This The Crime of The Century - Principia Scientific IntlDMDONo ratings yet