Volume 8, Issue 4, April – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Juvenile Metachromatic Leucodystrophy:
A Rare Case Report
Dr.Rohit Kukade, Dr Sushant Mane, Dr. Onkar Suryavanshi , Dr. Farheena Ansari
Department of Pediatrics, Grant Government Medical College, and Sir J.J. Group of Hospitals, Mumbai
Date for Submission- 26 April 2023
Date of Acceptance- 6 May 2023
Abstract:- Metachromatic leukodystrophy (MLD), also had an unsteady gait with frequent falls which progressed to
called arylsulfatase A deficiency (ARS-A) which is a rare the inability to walk even with support. He also developed
demyelinating disease (prevalence 1:40,000, presents progressive deterioration of speech. The speech was
with neurological and psychiatric symptoms. Clinical dysarthric and slurred, with an inability to speak at the time
assessment is difficult, due to nonspecific signs and of the presentation. Comprehension was intact. The child
symptoms. We report a case of a 7-year-old male child also had difficulty swallowing solid food with continuous
who is born of 3-rd degree consanguineous marriage drooling of saliva. There was a loss of bowel and bladder
with normal developmental milestones up to 3.5 years of control. He had one episode of Generalised tonic-clonic
age presenting with complaints of progressive seizure at 2 and a half years of age. The younger sibling has
impairment of walking over 3.5 years. Juvenile form of complaints with similar semiology. The younger sister is
MLD was diagnosed by typical history, neuroimaging and currently 5 years old. She presented to us with similar
confirmed by Clinical Exome Sequencing. complaints of gradually progressive impairment in walking
since she was 4 years old, speech difficulty, difficulty in
I. INTRODUCTION swallowing food and continuous drooling of saliva.
Metachromatic leukodystrophy (MLD) is a rare On examination, the child had an apathetic look with
demyelinating disease with a prevalence of 1:40,000 , the normal vital signs, no abnormal skin pigmentation was seen.
gene is located on chromosome 22q13.33, and the patient Only cooing was present in speech. Spasticity was present in
presents with neurological and psychiatric symptoms. all 4 limbs, power was 3/5, deep tendon reflexes were
Arylsulfatase A is essential for the normal metabolism of exaggerated, and the plantar response was bilateral extensor.
sulfatides. These are important constituents of the myelin Signs of meningeal irritation were absent. Cranial nerves
sheath. Sulfatides accumulates in the central nervous system examination was normal. No significant abnormalities were
and in various other tissues, like the peripheral nervous found in other systems.
system1. Increased in the amounts of cerebroside sulfate is
thought to cause breakdown of myelin and oligodendroglia III. DIAGNOSIS
destruction. The most frequent symptom of leukodystrophy
disease is a gradual decline of the development of an infant Complete blood count, liver and renal function tests
or child who has previously developed as per age. The were normal. On Fundoscopy there was no evidence of optic
clinical features includes progressive intellectual atrophy. MRI Brain with Spectroscopy was suggestive of
deterioration with varying degrees of pyramidal and confluent hyperintensities in the periventricular and deep
cerebellar dysfunction. The course of the disease is usually white matter of bilateral frontal, parietal, occipital lobes, and
progressive and Seizures thought infrequent may also occur. posterior limb of bilateral internal capsules. There was a
Enlargement of head is a feature in certain variants. It reversal of choline and creatinine peaks at white matter
includes three types - (i) late infantile form of the disease abnormality which favors demyelinating pathology,
starting before the age of 3 years, (ii) juvenile form that suggestive of metachromatic leukodystrophy.
starts between 3 to 16 years, and (iii) adult form presenting Electroencephalography was suggestive of normal interictal
its first symptoms after the age of 16 years2. The incidence sleep patterns. There was no epileptogenic focus seen on
of MLD is reported as to be 1 per 100,000 live births in the Electroencephalography.
European population and at an even lower rate in Asia. 3.
Clinical Exome Sequencing was suggestive of
II. CASE heterozygous missense variation in exon 3 of TMEM106B
gene hence a diagnosis of juvenile-onset metachromatic
A 7-year-old male born of third-degree leukodystrophy was made.
consanguineous marriage through normal vaginal delivery
had normal developmental milestones up to 3 years of age.
He was admitted with us for complaints of progressive
impairment in walking over the past 3.5 years. Initially, he
IJISRT23APR1968 www.ijisrt.com 2383
Volume 8, Issue 4, April – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
of inability to sit and stand with normal pattern development
previously. Mri brain was done which was Suggestive of
demyelination consistent with MLD. Arly sulfatase enzyme
activity was tested which was decreased thus confirming the
diagnosis.5
The indexed case presented the Juvenile form of MLD
with symptom onset and progressive deterioration occurring
over the last 4 years. Symptoms of the patient include the
gradual deterioration in scholastic performance, progressive
difficulty in walking, slurring of speech, and emotional and
behavioral disturbances that relate to that of Juvenile MLD.
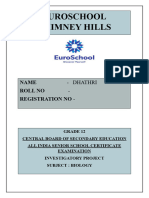
Fig 1:-T2 weighted MRI shows confluent hyperintensities in
the periventricular and deep white matter of bilateral frontal,
Metachromatic leukodystrophy manifests as symmetric
parietal, occipital lobes, and posterior limb of bilateral
confluent areas of high signal intensity in the periventricular
internal capsules.
white matter with sparing of the subcortical U fibers as seen
in T2 weighted MR imaging. 6
IV. TREATMENT
Clinical exome sequencing confirms the diagnosis of
The child was given supportive and symptomatic
metachromatic leucodystrophy.
treatment. Physiotherapy was started to prevent contractures
and maintain a normal tone. A diet chart was made and
In the case of asymptomatic late infantile and early
supplemented with calcium ,vitamin D, iron and folic acids
juvenile forms, , bone marrow or cord blood transplantation
to improve nutrition. The child was started on nasogastric
is the solution available primarily to improve
tube feeding. Baclofen added to relieve spasticity. Child was
neurocognitive functions. Here, in this case, drugs were
discharged and parents were counselled regarding the
introduced to improve the spasticity. Physiotherapy was
prognosis of the child.
initiated as a part of rehabilitation. Future treatment options
including gene therapy, and potentially enzyme
V. DISCUSSION
enhancement therapy are currently being explored 7.
Metachromatic leukodystrophy which is an autosomal
REFERENCES
recessive disorder caused because of deficiency of the
lysosomal hydrolase, Aryl sulfatase A (ARSA). It is defined
[1]. Poorthuis BJ, Wevel s RA, Kleijel WJ, Groener JE, de
by the lysosomal accumulation of sulfated glycolipids
Jong JG, van Wccly Sd, ct at. Thc fi‘cqucncy of
specifically 3-O-sulfagalactosyl-containing glycolipids. It
lysosomal storage diseases in The Netherlands.Hurn
mainly accumulates in the myelin sheaths of the central and
Genet 1999;105:151-6.
peripheral nervous system. These glycolipids accumulate in
[2]. Biffi A, Cesani M, Fumagalli F, Del Can o U, Baldoli
the lysosomes. This results in the characteristic
C, Canalc Sd, et al. Metachromatic leultodystropliy -
metachromatic staining of the tissues, hence the name of this
mutation analysis provides further evidence of
disease.
genotype-phenotype correlation. Clin Genet
2008;74:349-57.
Three different types of metachromatic leukodystrophy
[3]. Poorthuis BJ, Wevers RA, Kleijer WJ, Groener JE, de
have been recognized according to patient’s age at onset:
Jong JG, van Weely S, Niezen-Koning KE, et al. The
late infantile, juvenile, and adult 2. The juvenile type
frequency of lysosomal storage diseases in The
presents between 3-16 years. Most are affected before 10
Netherlands. Hum Genet. 1999;105(1-2):151-156.
years. The Clinical features of MLD include mental
[4]. Uddin, M. A., Islam, A., Hoque, S. K. A., & Saha, N.
deterioration, hypotonia, developmental delay, speech
(2018). Juvenile metachromatic leukodystrophy: A
abnormalities, loss of mental abilities, blindness, rigidity,
case report from Bangladesh. Journal of National
convulsions, paralysis, impaired swallowing , dementia,
Institute of Neurosciences Bangladesh, 4(2), 154–157.
poor school performance, tremors, ataxia, seizures, and
[5]. Lokhande VS, Gaur A. A Case of Infantile
dementia.
Metachromatic Leukodystrophy. Journal of Neurology
Research. ,2015;4(5-6):138-40
A similar case was reported by Mohammad Ala Uddin
[6]. Michael V. Johnston. Neurodegenerative Disoi‘ders of
et al of a 7-year-old female child presenting with a history of
Childhood. In: Bclirman RE, Kliegiuan RM, Jcnson
progressive weakness of all 4 limbs and loss of bowel
HB, editors. Nelson Textbook of Pediatrics. 18th ed.
bladder control. Mri was done with features suggestive of
W.B. Saunders 2008;6: 592-598.
MLD. The diagnosis was confirmed after performing an
[7]. Mallikarjun K, Deepak P Bhayya, Deepesh Singh,
enzyme assay which was markedly reduced. The patient was
Tarulatha R Shyagali. Metachromatic
treated with supportive care and physiotherapy 4.
Leukodystrophy: A Rare Case Report. Journal of
Academy of Advanced Dental Research, Vol 2; Issue
Another case was reported by Vaibhav S. Lokhande of
3, September 2011.
a 2 year 6 month old male child presenting with complaints
IJISRT23APR1968 www.ijisrt.com 2384
You might also like
- Clayton Parks and Recreation: Youth Soccer Coaching ManualDocument19 pagesClayton Parks and Recreation: Youth Soccer Coaching ManualFranklin Justniano VacaNo ratings yet
- Cerebral PalsyDocument25 pagesCerebral PalsyTINTU JOSEPHNo ratings yet
- A Book of Beasts PDFDocument32 pagesA Book of Beasts PDFbrad drac100% (2)
- Neurology Multiple Choice Questions With Explanations: Volume IFrom EverandNeurology Multiple Choice Questions With Explanations: Volume IRating: 4 out of 5 stars4/5 (7)
- Newton's Second LawDocument3 pagesNewton's Second LawBHAGWAN SINGHNo ratings yet
- Amyotrophic Lateral SclerosisDocument9 pagesAmyotrophic Lateral SclerosisCaroline ItnerNo ratings yet
- Infantile, Childhood, and Adolescent Epilepsies.9Document34 pagesInfantile, Childhood, and Adolescent Epilepsies.9Silviana IlieNo ratings yet
- Emotions Influence Color Preference PDFDocument48 pagesEmotions Influence Color Preference PDFfllorinvNo ratings yet
- A Rare Cause of Pancreatic Insufficiency Johanson Blizzard SyndromeDocument3 pagesA Rare Cause of Pancreatic Insufficiency Johanson Blizzard Syndromeد نبيل عبيدNo ratings yet
- A Rare Case Report On Metachromatic Leukodystrophy Presenting With Regression of MilestoneDocument3 pagesA Rare Case Report On Metachromatic Leukodystrophy Presenting With Regression of MilestoneBIOMEDSCIDIRECT PUBLICATIONSNo ratings yet
- Van Der KnapDocument3 pagesVan Der KnapKota AnuroopNo ratings yet
- Algoritmo Diferencial de Debilidad Proximal en Paciente Con Miopatia Adquirida Por Nemalina.Document7 pagesAlgoritmo Diferencial de Debilidad Proximal en Paciente Con Miopatia Adquirida Por Nemalina.Farid Santiago Abedrabbo LombeydaNo ratings yet
- Hercules Baby - A Rare Case Presentation of Congenital MyopathyDocument4 pagesHercules Baby - A Rare Case Presentation of Congenital MyopathyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Journal of Child Neurology 11Document5 pagesJournal of Child Neurology 11NEUROLAB ESCALÓNNo ratings yet
- Approach To Floppy InfantDocument7 pagesApproach To Floppy InfantLee Chiang ShengNo ratings yet
- Psychogenic Non-Epileptic Seizures: Indian Pediatrics November 2004Document4 pagesPsychogenic Non-Epileptic Seizures: Indian Pediatrics November 2004Nico NicoNo ratings yet
- Adult LeucodystrophyDocument12 pagesAdult LeucodystrophylauraalvisNo ratings yet
- Uncommon Disorders Masquerading As Acute Flaccid Paralysis in ChildrenDocument7 pagesUncommon Disorders Masquerading As Acute Flaccid Paralysis in ChildrenAnonymous G20oAbl6p8No ratings yet
- Clinical Cases in Pediatric Peripheral NeuropathyDocument23 pagesClinical Cases in Pediatric Peripheral NeuropathyMateen ShukriNo ratings yet
- Black UrineDocument2 pagesBlack Urinejoudi.jou95No ratings yet
- Metachromatic Leukodystrophy Pediatric PresentatioDocument7 pagesMetachromatic Leukodystrophy Pediatric PresentatioMike SihombingNo ratings yet
- Congenital Toxoplasmosis Associated With Severe Intracerebral Calcification and West SyndromeDocument3 pagesCongenital Toxoplasmosis Associated With Severe Intracerebral Calcification and West SyndromeDevina Rossita HapsariNo ratings yet
- Cretinism Revisited: Brief CommunicationDocument3 pagesCretinism Revisited: Brief CommunicationFamily Medicine FK UnsyiahNo ratings yet
- Hereditary SpherocytosisDocument39 pagesHereditary SpherocytosisjoannaNo ratings yet
- Long-Term Neuropsychological Follow-Up of A Child With Klüver-Bucy SyndromeDocument4 pagesLong-Term Neuropsychological Follow-Up of A Child With Klüver-Bucy SyndromefernandogfcnsNo ratings yet
- Apparently New Syndrome of Congenital Cataracts, Sensorineural Deafness, Down Syndrome-Like Facial Appearance, Short Stature, and Mental RetardationDocument5 pagesApparently New Syndrome of Congenital Cataracts, Sensorineural Deafness, Down Syndrome-Like Facial Appearance, Short Stature, and Mental Retardationjahfdfgsdjad asdhsajhajdkNo ratings yet
- Morphometry of WS On ASDocument6 pagesMorphometry of WS On ASAdrien DuthéNo ratings yet
- Inbornerrorsofmetabolism Withmovementdisorders: Defects in Metal Transport and Neurotransmitter MetabolismDocument15 pagesInbornerrorsofmetabolism Withmovementdisorders: Defects in Metal Transport and Neurotransmitter MetabolismVadiga Ramana KumarNo ratings yet
- Letter To The Editor: On Cognitive Variability in Velocardiofacial Syndrome: Profound Mental Retardation and AutismDocument2 pagesLetter To The Editor: On Cognitive Variability in Velocardiofacial Syndrome: Profound Mental Retardation and AutismHarshit AmbeshNo ratings yet
- Manejo Dental ELADocument4 pagesManejo Dental ELAAline LoyolaNo ratings yet
- Spectrum of Mri Findings in Pediatric Epilepsy Medical and Surgical Causes of Epilepsy in Children and Its Radiological CorrelatioDocument4 pagesSpectrum of Mri Findings in Pediatric Epilepsy Medical and Surgical Causes of Epilepsy in Children and Its Radiological CorrelatioImroatul hafidzahNo ratings yet
- Kikuchi's Disease: Malathi Sathiyasekaran R. Varadharajan So. ShivbalanDocument3 pagesKikuchi's Disease: Malathi Sathiyasekaran R. Varadharajan So. Shivbalanzulfikar adiNo ratings yet
- Pediatric Nephrology: Original ArticleDocument5 pagesPediatric Nephrology: Original ArticleGréta BotyánszkiNo ratings yet
- Neonatal Lupus With ExtensiveDocument2 pagesNeonatal Lupus With ExtensiveTylerNo ratings yet
- Case 40-2021 - A 9-Year-Old - Enf - MoyamoyaDocument10 pagesCase 40-2021 - A 9-Year-Old - Enf - MoyamoyaJuan C. Salazar PajaresNo ratings yet
- Spinal DisDocument32 pagesSpinal DisAkmal Niam FirdausiNo ratings yet
- Progressive Myoclonic - Genetic Therapeutic - Lancet 2005 (Shahwan)Document10 pagesProgressive Myoclonic - Genetic Therapeutic - Lancet 2005 (Shahwan)chintanNo ratings yet
- s10038 021 00981 3Document4 pagess10038 021 00981 3Jesus HuaytaNo ratings yet
- Leukodystrophy Paper August 27thDocument7 pagesLeukodystrophy Paper August 27thZorbey TurkalpNo ratings yet
- 445 1045 1 PBDocument6 pages445 1045 1 PBAnnisa Dhiya UlhaqNo ratings yet
- Bio Investigatory ProjectDocument50 pagesBio Investigatory ProjectdhathriNo ratings yet
- Abulia: No Will, No Way: SM Hastak, Pooja S Gorawara, NK MishraDocument6 pagesAbulia: No Will, No Way: SM Hastak, Pooja S Gorawara, NK Mishranurul ilmiNo ratings yet
- Autism Spectrum Disorders: Dr.R.G.Enoch MD Psychiatry Ii Yr GMKMCH, SalemDocument100 pagesAutism Spectrum Disorders: Dr.R.G.Enoch MD Psychiatry Ii Yr GMKMCH, Salemام اسامة السيايدةNo ratings yet
- Kulkarni 2004Document3 pagesKulkarni 2004AlfirahmatikaNo ratings yet
- Pediatric Movement Disorders: Five New ThingsDocument8 pagesPediatric Movement Disorders: Five New ThingsAndrea PederziniNo ratings yet
- Abstract: X-Linked Dystonia-Parkinsonism (XDP), or LubagDocument7 pagesAbstract: X-Linked Dystonia-Parkinsonism (XDP), or LubagKaila AbeledaNo ratings yet
- KetogenikDocument7 pagesKetogeniksari rezekiNo ratings yet
- Epilepsy and Electroencephalogram Evolution in YWHAG Gene MutationDocument8 pagesEpilepsy and Electroencephalogram Evolution in YWHAG Gene MutationGiselle Costa Daniel HonoratoNo ratings yet
- A Case Report of Obsessive-Compulsive DisorderDocument6 pagesA Case Report of Obsessive-Compulsive DisorderfonsoalNo ratings yet
- Thanatophoric Dysplasia: A Rare Entity: Oman Medical Journal May 2011Document3 pagesThanatophoric Dysplasia: A Rare Entity: Oman Medical Journal May 2011Atria DewiNo ratings yet
- Crum Rine 2001Document12 pagesCrum Rine 2001FabsscribNo ratings yet
- Progressive Increase of The Mutated Mitochondria1 DNA Fraction in Kearns-Sayre SyndromeDocument6 pagesProgressive Increase of The Mutated Mitochondria1 DNA Fraction in Kearns-Sayre SyndromeGréta BotyánszkiNo ratings yet
- Failure To ThriveDocument3 pagesFailure To ThrivefernandoNo ratings yet
- 2 2011Document4 pages2 2011Galaleldin AliNo ratings yet
- A Child With Myoclonus-Dystonia (DYT11) Misdiagnosed As Atypical Opsoclonus Myoclonus SyndromeDocument3 pagesA Child With Myoclonus-Dystonia (DYT11) Misdiagnosed As Atypical Opsoclonus Myoclonus SyndromeStephen AttardNo ratings yet
- CNS OsceDocument36 pagesCNS Oscebrajendra singhNo ratings yet
- Rett SyndromeDocument55 pagesRett SyndromeSnezana MihajlovicNo ratings yet
- Loss of The N-Myc Oncogene in A Patient With A Small Interstitial Deletion of The Short Arm of ChromosomeDocument5 pagesLoss of The N-Myc Oncogene in A Patient With A Small Interstitial Deletion of The Short Arm of ChromosomeantonioopNo ratings yet
- Amyotrophic Lateral Sclerosis A.: Excellent History But Was This Copy-Pasted?Document8 pagesAmyotrophic Lateral Sclerosis A.: Excellent History But Was This Copy-Pasted?Allan CastroNo ratings yet
- Clinicopathological Case Conference:: A 17 Year Old With Progressive Gait Difficulty and A Complex Family HistoryDocument3 pagesClinicopathological Case Conference:: A 17 Year Old With Progressive Gait Difficulty and A Complex Family HistoryChoi SpeaksNo ratings yet
- Menkes Kinky Hair Disease (Menkes Syndrome) - A Case ReportDocument5 pagesMenkes Kinky Hair Disease (Menkes Syndrome) - A Case ReportTannov SiregarNo ratings yet
- Abulia: No Will, No Way: SM Hastak, Pooja S Gorawara, NK MishraDocument5 pagesAbulia: No Will, No Way: SM Hastak, Pooja S Gorawara, NK MishraSaikat Prasad DattaNo ratings yet
- Filipa 2017Document5 pagesFilipa 2017Eleni KotanidouNo ratings yet
- Childhood Seized: Linguistic Considerations of the Effects of Epilepsy on Cognition in Children with Benign Childhood EpilepsyFrom EverandChildhood Seized: Linguistic Considerations of the Effects of Epilepsy on Cognition in Children with Benign Childhood EpilepsyNo ratings yet
- Study Assessing Viability of Installing 20kw Solar Power For The Electrical & Electronic Engineering Department Rufus Giwa Polytechnic OwoDocument6 pagesStudy Assessing Viability of Installing 20kw Solar Power For The Electrical & Electronic Engineering Department Rufus Giwa Polytechnic OwoInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Blockchain Based Decentralized ApplicationDocument7 pagesBlockchain Based Decentralized ApplicationInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Unmasking Phishing Threats Through Cutting-Edge Machine LearningDocument8 pagesUnmasking Phishing Threats Through Cutting-Edge Machine LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Cyber Security Awareness and Educational Outcomes of Grade 4 LearnersDocument33 pagesCyber Security Awareness and Educational Outcomes of Grade 4 LearnersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- An Industry That Capitalizes Off of Women's Insecurities?Document8 pagesAn Industry That Capitalizes Off of Women's Insecurities?International Journal of Innovative Science and Research TechnologyNo ratings yet
- Factors Influencing The Use of Improved Maize Seed and Participation in The Seed Demonstration Program by Smallholder Farmers in Kwali Area Council Abuja, NigeriaDocument6 pagesFactors Influencing The Use of Improved Maize Seed and Participation in The Seed Demonstration Program by Smallholder Farmers in Kwali Area Council Abuja, NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Smart Health Care SystemDocument8 pagesSmart Health Care SystemInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Insights Into Nipah Virus: A Review of Epidemiology, Pathogenesis, and Therapeutic AdvancesDocument8 pagesInsights Into Nipah Virus: A Review of Epidemiology, Pathogenesis, and Therapeutic AdvancesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Parastomal Hernia: A Case Report, Repaired by Modified Laparascopic Sugarbaker TechniqueDocument2 pagesParastomal Hernia: A Case Report, Repaired by Modified Laparascopic Sugarbaker TechniqueInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Visual Water: An Integration of App and Web To Understand Chemical ElementsDocument5 pagesVisual Water: An Integration of App and Web To Understand Chemical ElementsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Smart Cities: Boosting Economic Growth Through Innovation and EfficiencyDocument19 pagesSmart Cities: Boosting Economic Growth Through Innovation and EfficiencyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Compact and Wearable Ventilator System For Enhanced Patient CareDocument4 pagesCompact and Wearable Ventilator System For Enhanced Patient CareInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Impact of Silver Nanoparticles Infused in Blood in A Stenosed Artery Under The Effect of Magnetic Field Imp. of Silver Nano. Inf. in Blood in A Sten. Art. Under The Eff. of Mag. FieldDocument6 pagesImpact of Silver Nanoparticles Infused in Blood in A Stenosed Artery Under The Effect of Magnetic Field Imp. of Silver Nano. Inf. in Blood in A Sten. Art. Under The Eff. of Mag. FieldInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Predict The Heart Attack Possibilities Using Machine LearningDocument2 pagesPredict The Heart Attack Possibilities Using Machine LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Air Quality Index Prediction Using Bi-LSTMDocument8 pagesAir Quality Index Prediction Using Bi-LSTMInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Relationship Between Teacher Reflective Practice and Students Engagement in The Public Elementary SchoolDocument31 pagesThe Relationship Between Teacher Reflective Practice and Students Engagement in The Public Elementary SchoolInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Parkinson's Detection Using Voice Features and Spiral DrawingsDocument5 pagesParkinson's Detection Using Voice Features and Spiral DrawingsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Investigating Factors Influencing Employee Absenteeism: A Case Study of Secondary Schools in MuscatDocument16 pagesInvestigating Factors Influencing Employee Absenteeism: A Case Study of Secondary Schools in MuscatInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Implications of Adnexal Invasions in Primary Extramammary Paget's Disease: A Systematic ReviewDocument6 pagesImplications of Adnexal Invasions in Primary Extramammary Paget's Disease: A Systematic ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Keywords:-Ibadhy Chooranam, Cataract, Kann Kasam,: Siddha Medicine, Kann NoigalDocument7 pagesKeywords:-Ibadhy Chooranam, Cataract, Kann Kasam,: Siddha Medicine, Kann NoigalInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- An Analysis On Mental Health Issues Among IndividualsDocument6 pagesAn Analysis On Mental Health Issues Among IndividualsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Harnessing Open Innovation For Translating Global Languages Into Indian LanuagesDocument7 pagesHarnessing Open Innovation For Translating Global Languages Into Indian LanuagesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Utilization of Date Palm (Phoenix Dactylifera) Leaf Fiber As A Main Component in Making An Improvised Water FilterDocument11 pagesThe Utilization of Date Palm (Phoenix Dactylifera) Leaf Fiber As A Main Component in Making An Improvised Water FilterInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Making of Object Recognition Eyeglasses For The Visually Impaired Using Image AIDocument6 pagesThe Making of Object Recognition Eyeglasses For The Visually Impaired Using Image AIInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Advancing Healthcare Predictions: Harnessing Machine Learning For Accurate Health Index PrognosisDocument8 pagesAdvancing Healthcare Predictions: Harnessing Machine Learning For Accurate Health Index PrognosisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Diabetic Retinopathy Stage Detection Using CNN and Inception V3Document9 pagesDiabetic Retinopathy Stage Detection Using CNN and Inception V3International Journal of Innovative Science and Research TechnologyNo ratings yet
- The Impact of Digital Marketing Dimensions On Customer SatisfactionDocument6 pagesThe Impact of Digital Marketing Dimensions On Customer SatisfactionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Terracing As An Old-Style Scheme of Soil Water Preservation in Djingliya-Mandara Mountains - CameroonDocument14 pagesTerracing As An Old-Style Scheme of Soil Water Preservation in Djingliya-Mandara Mountains - CameroonInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Dense Wavelength Division Multiplexing (DWDM) in IT Networks: A Leap Beyond Synchronous Digital Hierarchy (SDH)Document2 pagesDense Wavelength Division Multiplexing (DWDM) in IT Networks: A Leap Beyond Synchronous Digital Hierarchy (SDH)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Formulation and Evaluation of Poly Herbal Body ScrubDocument6 pagesFormulation and Evaluation of Poly Herbal Body ScrubInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Marriage and Divorce Conflicts in The International PerspectiveDocument33 pagesMarriage and Divorce Conflicts in The International PerspectiveAnjani kumarNo ratings yet
- EntropyDocument38 pagesEntropyPreshanth_Jaga_2224No ratings yet
- Worksheet For Mathematics For ManagementDocument3 pagesWorksheet For Mathematics For Managementabel shimeles100% (1)
- Chapter 101-160Document297 pagesChapter 101-160Dipankar BoruahNo ratings yet
- Speech VP SaraDocument2 pagesSpeech VP SaraStephanie Dawn MagallanesNo ratings yet
- The Impact of Climatic and Cultural Factors On Openings in Traditional Houses in MaharashtraDocument14 pagesThe Impact of Climatic and Cultural Factors On Openings in Traditional Houses in Maharashtracoldflame81No ratings yet
- Telesis Events - Construction Contract Essentials - WorkbookDocument52 pagesTelesis Events - Construction Contract Essentials - WorkbookassmonkeysNo ratings yet
- Characters: Philadelphia Here I Come! by Brian FrielDocument4 pagesCharacters: Philadelphia Here I Come! by Brian FrielDominic LenihanNo ratings yet
- Chapter 7: Identifying and Understanding ConsumersDocument3 pagesChapter 7: Identifying and Understanding ConsumersDyla RafarNo ratings yet
- Nursing Informatics: Sanil VargheseDocument55 pagesNursing Informatics: Sanil VarghesePalwasha KhanNo ratings yet
- Energizing Your ScalesDocument3 pagesEnergizing Your ScalesjohnNo ratings yet
- Hapter 2: Theoretical FrameworkDocument18 pagesHapter 2: Theoretical FrameworkMohamed HamzaNo ratings yet
- Remarkings AirportsDocument1 pageRemarkings AirportsJuan Jose CaleroNo ratings yet
- Soal Respi 2010Document41 pagesSoal Respi 2010Joseph ThanaNo ratings yet
- World War I Almanac Almanacs of American WarsDocument561 pagesWorld War I Almanac Almanacs of American WarsMatheus Benedito100% (1)
- Leverage My PptsDocument34 pagesLeverage My PptsMadhuram SharmaNo ratings yet
- Gullivers TravelDocument3 pagesGullivers TravelRanen Das MishukNo ratings yet
- Analysis of Effectiveness of Heat Exchanger Shell and Tube Type One Shell Two Tube Pass As Cooling OilDocument6 pagesAnalysis of Effectiveness of Heat Exchanger Shell and Tube Type One Shell Two Tube Pass As Cooling OilHendrik V SihombingNo ratings yet
- Noorul Islam Centre For Higher Education Noorul Islam University, Kumaracoil M.E. Biomedical Instrumentation Curriculum & Syllabus Semester IDocument26 pagesNoorul Islam Centre For Higher Education Noorul Islam University, Kumaracoil M.E. Biomedical Instrumentation Curriculum & Syllabus Semester Iisaac RNo ratings yet
- Chapter 14Document4 pagesChapter 14Rafael Costa SampaioNo ratings yet
- CPN Project TopicsDocument1 pageCPN Project TopicsvirginNo ratings yet
- Schemes and Tropes HandoutDocument6 pagesSchemes and Tropes HandoutJohn LukezicNo ratings yet
- Accounting Volume 1 Canadian 8th Edition Horngren Solutions ManualDocument25 pagesAccounting Volume 1 Canadian 8th Edition Horngren Solutions ManualElizabethBautistadazi100% (43)
- Description of Medical Specialties Residents With High Levels of Workplace Harassment Psychological Terror in A Reference HospitalDocument16 pagesDescription of Medical Specialties Residents With High Levels of Workplace Harassment Psychological Terror in A Reference HospitalVictor EnriquezNo ratings yet
- Case Study Method: Dr. Rana Singh MBA (Gold Medalist), Ph. D. 98 11 828 987Document33 pagesCase Study Method: Dr. Rana Singh MBA (Gold Medalist), Ph. D. 98 11 828 987Belur BaxiNo ratings yet
- Universal Declaration of Human Rights - United NationsDocument12 pagesUniversal Declaration of Human Rights - United NationsSafdar HussainNo ratings yet