You might also like
- Eccd ComputationDocument13 pagesEccd ComputationJoan Del Castillo Naing100% (1)
- Template SIP (Part 3)Document21 pagesTemplate SIP (Part 3)Monaoray SangcopanNo ratings yet
- Experiment 9Document6 pagesExperiment 9clairedemotica100% (1)
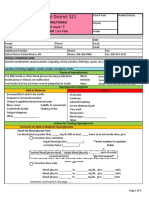
- Diabetes Hyperglycemia Emergency Care PlanDocument2 pagesDiabetes Hyperglycemia Emergency Care Planapi-405196113No ratings yet
- Oplan Kalusugan Form BDocument5 pagesOplan Kalusugan Form BEzekiel ReyesNo ratings yet
- Ok Sa Deped Form B - For SchoolsDocument5 pagesOk Sa Deped Form B - For SchoolsAna Cella Rico MarzoNo ratings yet
- Ok Sa Deped Form BDocument5 pagesOk Sa Deped Form BKhulyn Castro AlvarezNo ratings yet
- Ok Sa Deped Form BDocument5 pagesOk Sa Deped Form BLyra Lyn R BaniquidNo ratings yet
- OPLAN KALUSUGAN SA DEPED SoftDocument5 pagesOPLAN KALUSUGAN SA DEPED SoftRonnel Andres HernandezNo ratings yet
- OKD Form BDocument4 pagesOKD Form BAirene Mariel MagbanuaNo ratings yet
- DO s2018 028Document29 pagesDO s2018 028erikabeltran100% (1)
- Ok Sa Deped Form BFDocument5 pagesOk Sa Deped Form BFDaRylNo ratings yet
- DO s2018 028-Converted-1Document29 pagesDO s2018 028-Converted-1Jenie Viva AndradeNo ratings yet
- Ok Sa Deped Form CDocument4 pagesOk Sa Deped Form CMeera Joy Deboma BlancoNo ratings yet
- Revised OKD Form B - Progress Report FormDocument4 pagesRevised OKD Form B - Progress Report FormDarren CariñoNo ratings yet
- (To Be Accomplished by The School Head) : Plan Alusugan Sa DepedDocument14 pages(To Be Accomplished by The School Head) : Plan Alusugan Sa DepedIrene TorredaNo ratings yet
- Ok Sa Deped Form B (Dsfes)Document10 pagesOk Sa Deped Form B (Dsfes)Maan Bautista100% (2)
- Okd Form ADocument15 pagesOkd Form ARollyNo ratings yet
- Ok Sa Deped Form CDocument4 pagesOk Sa Deped Form CJanus SalinasNo ratings yet
- Revised OK Sa DepEd Forms 2019 1Document16 pagesRevised OK Sa DepEd Forms 2019 1Marison GerantaNo ratings yet
- Ok Sa Deped Form BDocument5 pagesOk Sa Deped Form BLei Anne Kate DimailigNo ratings yet
- Okd Ohw Report FormDocument25 pagesOkd Ohw Report FormMarilyne S RabangNo ratings yet
- Ok Sa Deped Accomplishment ReportDocument15 pagesOk Sa Deped Accomplishment ReportAnonymous YhZlC5AmNo ratings yet
- Revised OK Sa DepEd Forms 2019Document16 pagesRevised OK Sa DepEd Forms 2019Annielou OliveraNo ratings yet
- Quality Form Oplan Kalusugan Sa Deped Accomplishment Report FormDocument36 pagesQuality Form Oplan Kalusugan Sa Deped Accomplishment Report FormBulaay ZarenNo ratings yet
- Okd Form ADocument22 pagesOkd Form AJoan DalilisNo ratings yet
- Dttes Ok Sa Deped Form C-1Document4 pagesDttes Ok Sa Deped Form C-1jerome100% (2)
- SIP Annex 5 Planning Worksheet 2022Document4 pagesSIP Annex 5 Planning Worksheet 2022Maura MartinezNo ratings yet
- Quality Form Oplan Kalusugan Sa Deped Accomplishment Report FormDocument24 pagesQuality Form Oplan Kalusugan Sa Deped Accomplishment Report FormJoules Laureta Fabros GaleraNo ratings yet
- Revised Okd Form ADocument13 pagesRevised Okd Form AKhulyn Castro AlvarezNo ratings yet
- Gcu Student Teaching Evaluation of Performance StepDocument31 pagesGcu Student Teaching Evaluation of Performance Stepapi-664394070No ratings yet
- Annual Gender and DevelopmentDocument4 pagesAnnual Gender and DevelopmentCarlota Tejero100% (1)
- Quality Form Oplan Kalusugan Sa Deped Accomplishment Report FormDocument11 pagesQuality Form Oplan Kalusugan Sa Deped Accomplishment Report Formchris orlanNo ratings yet
- Tin Gap AnalysisDocument10 pagesTin Gap AnalysisTinTinNo ratings yet
- Sip / Aip: Department of Education 1 Division of Davao CityDocument43 pagesSip / Aip: Department of Education 1 Division of Davao CityRiza joy Sarile100% (1)
- Progress Report: Plan Alusugan Sa DepedDocument3 pagesProgress Report: Plan Alusugan Sa DepedRosalie Dela CruzNo ratings yet
- OKsaDepEd Form C - v.3Document13 pagesOKsaDepEd Form C - v.3ayatolla ayatollaTMNo ratings yet
- Agripina Elementary School-Monitoring ToolDocument4 pagesAgripina Elementary School-Monitoring ToolLea RemorozaNo ratings yet
- Appendex H BE FORM 7 SCHOOL ACCOMPLISHMENT REPORTDocument4 pagesAppendex H BE FORM 7 SCHOOL ACCOMPLISHMENT REPORTMR. HeavyNo ratings yet
- SIP Annex 3 - Gap Analysis TemplateDocument5 pagesSIP Annex 3 - Gap Analysis Templatejovito limotNo ratings yet
- Enhanced SIP - Phase 1-Assess - (Sir Ramil)Document24 pagesEnhanced SIP - Phase 1-Assess - (Sir Ramil)EUDOLFO FLORESNo ratings yet
- Program Terminal Report - SBFPDocument3 pagesProgram Terminal Report - SBFPMannielle MeNo ratings yet
- SIP Annex 3 - Gap Analysis TemplateDocument6 pagesSIP Annex 3 - Gap Analysis TemplateJoel HinayNo ratings yet
- Ro-I Schools Division of Ilocos Norte January - December 2019Document15 pagesRo-I Schools Division of Ilocos Norte January - December 2019Louie J. UbayNo ratings yet
- Aip 2021 1Document5 pagesAip 2021 1AMALIA CAGAMPANGNo ratings yet
- I.Program Implementation Progress: ST ND RD THDocument3 pagesI.Program Implementation Progress: ST ND RD THKaren BlythNo ratings yet
- Gschs Annual-Implementation 2008-2012 EditedDocument10 pagesGschs Annual-Implementation 2008-2012 EditedTibooc EdwardNo ratings yet
- GAD Accomplishment Report For FY 2021 School TemplateDocument5 pagesGAD Accomplishment Report For FY 2021 School TemplateAPRIL VISIA SITIERNo ratings yet
- Gap (Sip)Document10 pagesGap (Sip)Patrick PelicanoNo ratings yet
- Quality Form: Ok Sa Deped - School-Based Feeding Program (SBFP) Program Terminal Report FormDocument3 pagesQuality Form: Ok Sa Deped - School-Based Feeding Program (SBFP) Program Terminal Report FormREYMAR RAMOS100% (4)
- Annex A Citizen's Charter SGNHSDocument2 pagesAnnex A Citizen's Charter SGNHSMarla MagatNo ratings yet
- Memo-SIP-NewDocument31 pagesMemo-SIP-NewVanne CandoNo ratings yet
- GAD Enclosure 1 LTES-ANNEX 2022-AccomplishmentsDocument2 pagesGAD Enclosure 1 LTES-ANNEX 2022-AccomplishmentsMay-ann Ramos Galliguez ValdezNo ratings yet
- Ecd Class ProfileDocument14 pagesEcd Class ProfileDan Sia DeiNo ratings yet
- Identify PIAsDocument25 pagesIdentify PIAsGABRIEL ANGELO G DADULANo ratings yet
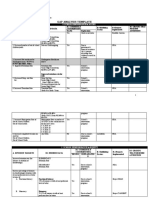
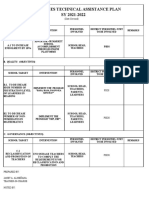
- Ta PlanDocument4 pagesTa PlanJanet AlmenanaNo ratings yet
- Annual Gender and DevelopmentDocument5 pagesAnnual Gender and DevelopmentCarlota Tejero100% (1)
- Department of Education: Annual Gender and Development (Gad) Plan and BudgetDocument6 pagesDepartment of Education: Annual Gender and Development (Gad) Plan and BudgetJaymar Padayao0% (1)
- Enclosure-1-2021-School-GAD-Accomp.-Report LTES-MAINDocument2 pagesEnclosure-1-2021-School-GAD-Accomp.-Report LTES-MAINMay-ann Ramos Galliguez ValdezNo ratings yet
- (C) Yearly - Performance - Appraisal - ReportDocument8 pages(C) Yearly - Performance - Appraisal - Reportprasad_batheNo ratings yet
- Department of Education Region VI - Western Visayas Division of Negros OccidentalDocument5 pagesDepartment of Education Region VI - Western Visayas Division of Negros OccidentalHelen Diano MontesclarosNo ratings yet
- Aip2021 Edited 1Document31 pagesAip2021 Edited 1JOSELITO AGUANo ratings yet
- Education in the Republic of South Sudan: Status and Challenges for a New SystemFrom EverandEducation in the Republic of South Sudan: Status and Challenges for a New SystemNo ratings yet
- Action-Plan AndayDocument4 pagesAction-Plan AndayJoan Del Castillo NaingNo ratings yet
- Table 1-F: Status of Identified Unaccomplished Outputs (Ppas) For The QuarterDocument2 pagesTable 1-F: Status of Identified Unaccomplished Outputs (Ppas) For The QuarterJoan Del Castillo NaingNo ratings yet
- Accom July3Document13 pagesAccom July3Joan Del Castillo NaingNo ratings yet
- Schools Division Office Camarines Norte Dagang Elementary School Paracale District Project ProposalDocument2 pagesSchools Division Office Camarines Norte Dagang Elementary School Paracale District Project ProposalJoan Del Castillo Naing100% (1)
- 1st Quarter Division Monitoring, Evaluation and Adjustment (DMEA)Document5 pages1st Quarter Division Monitoring, Evaluation and Adjustment (DMEA)Joan Del Castillo NaingNo ratings yet
- Disbursement Voucher: Juan Dela CruzDocument9 pagesDisbursement Voucher: Juan Dela CruzJoan Del Castillo NaingNo ratings yet
- Summary of Physical and Financial Accomplishment: Schools Division OfficeDocument2 pagesSummary of Physical and Financial Accomplishment: Schools Division OfficeJoan Del Castillo Naing100% (4)
- Department of Education: Republic of The PhilippinesDocument1 pageDepartment of Education: Republic of The PhilippinesJoan Del Castillo NaingNo ratings yet
- Tos-Test Mapeh 1Document6 pagesTos-Test Mapeh 1Joan Del Castillo NaingNo ratings yet
- Program of Works: Dagang Elementary SchoolDocument2 pagesProgram of Works: Dagang Elementary SchoolJoan Del Castillo Naing100% (1)
- Department of Education: Republic of The PhilippinesDocument1 pageDepartment of Education: Republic of The PhilippinesJoan Del Castillo NaingNo ratings yet
- Schools Division Office Camarines Norte Dagang Elementary School Paracale District Project ProposalDocument5 pagesSchools Division Office Camarines Norte Dagang Elementary School Paracale District Project ProposalJoan Del Castillo Naing100% (1)
- Pretest Graph ResearchDocument11 pagesPretest Graph ResearchJoan Del Castillo NaingNo ratings yet
- Abc Plus Participants: Noel - Ibis001@deped - Gov.phDocument1 pageAbc Plus Participants: Noel - Ibis001@deped - Gov.phJoan Del Castillo NaingNo ratings yet
- Post Test' Graph ResearchDocument11 pagesPost Test' Graph ResearchJoan Del Castillo NaingNo ratings yet
- ENG7Q1W1D1: Eco Athletic Field, F. Pimentel Ave.Document9 pagesENG7Q1W1D1: Eco Athletic Field, F. Pimentel Ave.Joan Del Castillo NaingNo ratings yet
- William Opcrf 2016-2017Document10 pagesWilliam Opcrf 2016-2017Joan Del Castillo NaingNo ratings yet
- Pretest Graph ResearchDocument11 pagesPretest Graph ResearchJoan Del Castillo NaingNo ratings yet
- Palmero Eldie A. Internet ResearchDocument3 pagesPalmero Eldie A. Internet ResearchJoan Del Castillo NaingNo ratings yet
- OralP Resentation AntonDocument13 pagesOralP Resentation AntonJoan Del Castillo NaingNo ratings yet
- Work and Financial Plan School-Based Feeding Program (SBFP)Document9 pagesWork and Financial Plan School-Based Feeding Program (SBFP)Joan Del Castillo Naing0% (1)
- All Types of Learners of The SchoolDocument6 pagesAll Types of Learners of The SchoolJoan Del Castillo NaingNo ratings yet
- PDS AttachmentDocument1 pagePDS AttachmentJoan Del Castillo NaingNo ratings yet
- DLL - Mapeh 4 - Q1 - W3Document5 pagesDLL - Mapeh 4 - Q1 - W3Joan Del Castillo NaingNo ratings yet
- Biology Class PowerpointDocument50 pagesBiology Class PowerpointBruh OofNo ratings yet
- GP Information Prescriptions - Healthy KidneyDocument1 pageGP Information Prescriptions - Healthy Kidneyleft vouzouNo ratings yet
- CarbohydratesDocument41 pagesCarbohydratesStrange Me100% (3)
- Australian Dietary Guidelines and Infant Feeding GuidelinesDocument1 pageAustralian Dietary Guidelines and Infant Feeding GuidelinesVladimir VladNo ratings yet
- Dietitian Notes (NCP)Document4 pagesDietitian Notes (NCP)Kazmanie KamaruzamanNo ratings yet
- STA255 - Statistical Theory: Assignment #1 (/36 Marks)Document4 pagesSTA255 - Statistical Theory: Assignment #1 (/36 Marks)Tom QiNo ratings yet
- Carotid Artery Disease: Causes, Symptoms, Tests, and TreatmentDocument6 pagesCarotid Artery Disease: Causes, Symptoms, Tests, and TreatmentVijay Baskar SNo ratings yet
- Revised - Syllabi of BSC Catering Science & Hotel ManagementDocument62 pagesRevised - Syllabi of BSC Catering Science & Hotel ManagementBoseNo ratings yet
- The Benefits of ExerciseDocument21 pagesThe Benefits of ExerciseJay R BayaniNo ratings yet
- Renal Anatomy and PhysiologyDocument38 pagesRenal Anatomy and PhysiologyCamille EspinosaNo ratings yet
- Chapter 4 Presentation, Interpretation, Analysis of DataDocument9 pagesChapter 4 Presentation, Interpretation, Analysis of DataTiphanie KangNo ratings yet
- Pre-Employment Medical Examinations (PEME) Centres: The Importance of PEMEDocument3 pagesPre-Employment Medical Examinations (PEME) Centres: The Importance of PEMEDrago DragicNo ratings yet
- Asuhan Pranikah PDFDocument57 pagesAsuhan Pranikah PDFDessy PratiwiNo ratings yet
- DM 1 and 2 PathophysiologyDocument1 pageDM 1 and 2 PathophysiologyApril Rose ParconNo ratings yet
- cs3 QuestionsDocument3 pagescs3 Questionsapi-251084195No ratings yet
- Research PaperDocument23 pagesResearch Paperapi-4919048650% (1)
- RenegadeStrong2015 2 PDFDocument26 pagesRenegadeStrong2015 2 PDFdondon_boyNo ratings yet
- Case Eop Group A Year 3 MbbsDocument7 pagesCase Eop Group A Year 3 MbbsKalaivaany RamachandranNo ratings yet
- Swain 2006Document7 pagesSwain 2006GorkaBuesaNo ratings yet
- Elc 030 (Week 2)Document21 pagesElc 030 (Week 2)ahmad mukhlisNo ratings yet
- Coronary Artery Disease (CAD) : Considerations in The ElderlyDocument15 pagesCoronary Artery Disease (CAD) : Considerations in The ElderlyAnonymous IzSqe3LDdNo ratings yet
- Writing An Argumentative Thesis StatementDocument3 pagesWriting An Argumentative Thesis StatementElba DuarteNo ratings yet
- Banned Drugs in IndiaDocument2 pagesBanned Drugs in IndiaSweta KulkarniNo ratings yet
- Growth Hormone Responses To Sub-Maximal and Sprint Exercise: Keith StokesDocument14 pagesGrowth Hormone Responses To Sub-Maximal and Sprint Exercise: Keith StokesganduaffNo ratings yet
- Comp Rev Food Sci Food Safe - 2022 - Nimbkar - Medium Chain Triglycerides MCT State of The Art On Chemistry SynthesisDocument25 pagesComp Rev Food Sci Food Safe - 2022 - Nimbkar - Medium Chain Triglycerides MCT State of The Art On Chemistry SynthesisProduction DepartmentNo ratings yet
- Children With DiabetesDocument104 pagesChildren With DiabetesArmand VeleanoviciNo ratings yet
- IBSe FinalDocument24 pagesIBSe FinaledyyantoNo ratings yet
- The Science Behind Crème CaramelDocument21 pagesThe Science Behind Crème CaramelAnonymous y9uQsPCuWNo ratings yet