You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Minimally Invasive ProceduresDocument35 pagesMinimally Invasive ProceduresAlex Pieces100% (2)
- Pathophysiology (Cervical Cancer) Case StudyDocument7 pagesPathophysiology (Cervical Cancer) Case StudyRosalie Valdez Espiritu100% (2)
- Attention Deficit Hyperactivity DisorderDocument8 pagesAttention Deficit Hyperactivity DisorderShinjiNo ratings yet
- Buletin de Analize Medicale: (Ssehjjdw)Document6 pagesBuletin de Analize Medicale: (Ssehjjdw)Moise GeorgeNo ratings yet
- New Clinical Rotation Balaji 2016 2017Document22 pagesNew Clinical Rotation Balaji 2016 2017rama joy100% (1)
- Tooth MobilityDocument47 pagesTooth Mobilityc4rm3LNo ratings yet
- Oral Radiology Principles and Interpretation 7th Ed PDFDocument14 pagesOral Radiology Principles and Interpretation 7th Ed PDFLaura Victoria Alvarez RodriguezNo ratings yet
- 002 POS Format 1Document9 pages002 POS Format 1Roland Philip GoNo ratings yet
- VestibuloplastyDocument57 pagesVestibuloplastyArWiny Wulandari HipiNo ratings yet
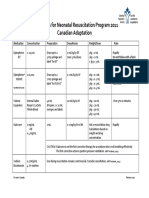
- Medications For Neonatal Resuscitation Program 2011 Canadian AdaptationDocument1 pageMedications For Neonatal Resuscitation Program 2011 Canadian AdaptationrubymayNo ratings yet
- Adequacy of PerfusionDocument11 pagesAdequacy of PerfusionLaiba SiddiqueNo ratings yet
- AnticoagulantsDocument9 pagesAnticoagulantszanyarfaraidwn99No ratings yet
- Swine FluDocument32 pagesSwine FluSajan Varghese100% (1)
- Cardiac GlycosidesDocument8 pagesCardiac GlycosidesShan Sicat100% (1)
- Cenforceshops Com ...Document2 pagesCenforceshops Com ...davidssmith325No ratings yet
- Drugs Used in Otology and Their FormulationsDocument4 pagesDrugs Used in Otology and Their FormulationsAnish RajNo ratings yet
- Chemical Burn 3Document4 pagesChemical Burn 3Yeni PuspitasariNo ratings yet
- Obstetric Outpatient: Friday, April 20 2018Document14 pagesObstetric Outpatient: Friday, April 20 2018Riyan W. PratamaNo ratings yet
- ECMO For COVID 19 Updated 2021 Guidelines From.98326Document42 pagesECMO For COVID 19 Updated 2021 Guidelines From.98326risanataliasiburianNo ratings yet
- Sample of MMDSTDocument32 pagesSample of MMDSTBeverly PatriarcaNo ratings yet
- Effects of Food Habits On Menstrual Cycle Among Adolescent GirlsDocument10 pagesEffects of Food Habits On Menstrual Cycle Among Adolescent GirlsDon Baraka DanielNo ratings yet
- CAGAY NHS-ARH-2022-reportDocument4 pagesCAGAY NHS-ARH-2022-reportAda RicanaNo ratings yet
- Improvement of Pregnant Women Visit in Puskesmas As An Effect of Using Ultrasound in Pregnancy ExaminationDocument12 pagesImprovement of Pregnant Women Visit in Puskesmas As An Effect of Using Ultrasound in Pregnancy ExaminationKharinaNo ratings yet
- Bacterial KeratitisDocument31 pagesBacterial KeratitisMuhammad Rehan SarfrazNo ratings yet
- Lange2010 Article TheHistoryOfAttentionDeficitHy PDFDocument15 pagesLange2010 Article TheHistoryOfAttentionDeficitHy PDFBilly James St JohnNo ratings yet
- Pathophysiology and Etiology of PCP: HIV InfectionDocument20 pagesPathophysiology and Etiology of PCP: HIV InfectionJehan Sendix100% (1)
- אנדוDocument111 pagesאנדוLiav KfirNo ratings yet
- Burn GuidelineDocument7 pagesBurn GuidelinegreenNo ratings yet
- 5 Sore ThroatDocument45 pages5 Sore ThroatNurul Wandasari SNo ratings yet
- Cardiogenic Shock: BY Dr. M L Patel MD Associate Professor Deptt. of MedicineDocument19 pagesCardiogenic Shock: BY Dr. M L Patel MD Associate Professor Deptt. of MedicineDurgesh PushkarNo ratings yet