You might also like
- DL Form 2Document1 pageDL Form 2Ashutosh Shukla T8 407No ratings yet
- Form 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical FitnessDocument1 pageForm 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical FitnessPathan AlmasNo ratings yet
- Form 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical FitnessDocument1 pageForm 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical Fitnesssudarsanan janakiramanNo ratings yet
- Sik Med CompressedDocument1 pageSik Med Compressedjos riderNo ratings yet
- Transport Department. Govt of NCT of Delhi: Form 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) )Document1 pageTransport Department. Govt of NCT of Delhi: Form 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) )RahulNo ratings yet
- Form 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) Medical CertificateDocument1 pageForm 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) Medical Certificatemir rameezNo ratings yet
- Transport Department. Govt of NCT of Delhi: Form 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) )Document1 pageTransport Department. Govt of NCT of Delhi: Form 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) )Rãhûl SâïñíNo ratings yet
- Form 1-A: Certificate of Medical FitnessDocument1 pageForm 1-A: Certificate of Medical FitnessDvyesh VasavaNo ratings yet
- Transport Department. Govt of NCT of Delhi: Form 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) )Document1 pageTransport Department. Govt of NCT of Delhi: Form 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) )shivam maindolaNo ratings yet
- Form 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical FitnessDocument1 pageForm 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical FitnessVinayak ShegarNo ratings yet
- Medical Certificate: See Rules 5 (1), (3), 7, 10 (A), 14 (D) and 18 (D) )Document2 pagesMedical Certificate: See Rules 5 (1), (3), 7, 10 (A), 14 (D) and 18 (D) )Dhiraj KhajuriaNo ratings yet
- Nagarajan DeclarationDocument1 pageNagarajan DeclarationSg BalajiNo ratings yet
- Central Motor Vehicle Rules, 1989: Form 1-ADocument1 pageCentral Motor Vehicle Rules, 1989: Form 1-ADADADADGGGNo ratings yet
- Form 1 ADocument2 pagesForm 1 Ahallownfs123No ratings yet
- Form 1-A Medical Certificate 1Document1 pageForm 1-A Medical Certificate 1Niel JangirNo ratings yet
- Transport Department. Govt of NCT of Delhi: Form 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) )Document1 pageTransport Department. Govt of NCT of Delhi: Form 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) )Dhruv BhatiaNo ratings yet
- Medical Certificate: Form 1A (See Rules 5 (1), (3), 7, 10 (A), 14 (D) and 18 (D) )Document2 pagesMedical Certificate: Form 1A (See Rules 5 (1), (3), 7, 10 (A), 14 (D) and 18 (D) )Rahul RajNo ratings yet
- Form1A RemoveDocument2 pagesForm1A Removekulvender singhNo ratings yet
- Form 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical FitnessDocument1 pageForm 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical FitnessSachin SawantNo ratings yet
- Form 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical FitnessDocument1 pageForm 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical Fitnessmudra123456789No ratings yet
- Form 1aDocument1 pageForm 1aDanish MushtaqNo ratings yet
- Form 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical FitnessDocument1 pageForm 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical Fitnesspravinpurohit510No ratings yet
- Eye TestDocument2 pagesEye TestTony MartinNo ratings yet
- Form 1aDocument2 pagesForm 1aRUSH MASTERNo ratings yet
- Form 1ANDocument2 pagesForm 1ANDiby JacobNo ratings yet
- LEAFDocument1 pageLEAFChetanya VigNo ratings yet
- Form 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical FitnessDocument1 pageForm 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical FitnesstsmtsghzpNo ratings yet
- c105b Medical Certificate For Service at SeaDocument1 pagec105b Medical Certificate For Service at SeaAdiNo ratings yet
- License Form 1aDocument1 pageLicense Form 1aNikhil Verma100% (1)
- Form 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical FitnessDocument1 pageForm 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical FitnessPradyumna DangewarNo ratings yet
- Printed Form1aDocument1 pagePrinted Form1aSudhanshu BhureNo ratings yet
- Form 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical FitnessDocument1 pageForm 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical FitnessAshirbad SahuNo ratings yet
- Form 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical FitnessDocument1 pageForm 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical FitnesstilakNo ratings yet
- Medical Fitness Form For Drivers LicenseDocument1 pageMedical Fitness Form For Drivers LicenseRanjithNo ratings yet
- Form 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical FitnessDocument1 pageForm 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical FitnessSarangapani KaliyamoorthyNo ratings yet
- Form-1A Medical Fitness CertificateDocument1 pageForm-1A Medical Fitness CertificatePrem SinghaniaNo ratings yet
- Driving Licence Medical Report Form Free PDFDocument2 pagesDriving Licence Medical Report Form Free PDFTimothyWartNo ratings yet
- Eye Sight Test CertificateDocument2 pagesEye Sight Test CertificateRavi Pratap SinghNo ratings yet
- Visual PDFDocument1 pageVisual PDFVikas TiwariNo ratings yet
- Dipu MedicalDocument1 pageDipu MedicalPranjit BhuyanNo ratings yet
- PDF Form 1Document1 pagePDF Form 1Alka BhadauriyaNo ratings yet
- APPLICATIONS FOR A DRIVING LICENCE AND ADDITION OF A NEW CLASS OF VEHICLE TO A DRIVING LICENCE (For Indian Citizen) PART - I.ÂDocument12 pagesAPPLICATIONS FOR A DRIVING LICENCE AND ADDITION OF A NEW CLASS OF VEHICLE TO A DRIVING LICENCE (For Indian Citizen) PART - I.ÂRahul UnnikrishnanNo ratings yet
- Adobe Scan 20-Jan-2024Document2 pagesAdobe Scan 20-Jan-2024Divyansh chaturvediNo ratings yet
- Form 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical FitnessDocument1 pageForm 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical Fitnessamit kargwalNo ratings yet
- Form 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical FitnessDocument1 pageForm 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical FitnesskawaljitNo ratings yet
- Illinois: Driver Licensing Agency Contact InformationDocument1 pageIllinois: Driver Licensing Agency Contact InformationBassam Al-HimiariNo ratings yet
- Application PDFDocument6 pagesApplication PDFRohit ChandrasekharNo ratings yet
- Form 2: Services Applying For (Please Tick Wherever Applicable)Document6 pagesForm 2: Services Applying For (Please Tick Wherever Applicable)Pradeep KumarNo ratings yet
- Transport DeptDocument28 pagesTransport DeptBooth TuckersNo ratings yet
- Medical 230831 091442Document1 pageMedical 230831 091442Ikra husnNo ratings yet
- Certificate of Medical FitnessDocument2 pagesCertificate of Medical Fitnessarivu raviNo ratings yet
- Form 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical FitnessDocument1 pageForm 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical FitnessNagaraju MuruguduNo ratings yet
- Form 1-A: Certificate of Medical FitnessDocument1 pageForm 1-A: Certificate of Medical Fitnesskavitha chinnaduraiNo ratings yet
- Form 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical FitnessDocument1 pageForm 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical FitnessChandan MohantyNo ratings yet
- Form 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical FitnessDocument1 pageForm 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical Fitnesssttkems.whatsappNo ratings yet
- Central Motor Vehicle Rules, 1989: Form 1-ADocument1 pageCentral Motor Vehicle Rules, 1989: Form 1-Avimal kothariNo ratings yet
- Form 1Document3 pagesForm 1Shruti TimmapurNo ratings yet
- Form 1-A: Certificate of Medical FitnessDocument1 pageForm 1-A: Certificate of Medical Fitnesspranay bhute100% (1)
- Almansoori Inspection Services: Lifting Equipment Thorough Examination ReportDocument4 pagesAlmansoori Inspection Services: Lifting Equipment Thorough Examination ReportRanjithNo ratings yet
- Department of Transportation Medical Reference for ExaminersFrom EverandDepartment of Transportation Medical Reference for ExaminersNo ratings yet
- Neha Maruti SuzukiDocument85 pagesNeha Maruti SuzukiShobhitShankhalaNo ratings yet
- The Tapescript-Electric CarsDocument2 pagesThe Tapescript-Electric CarsCarmen Nebreda QuintanaNo ratings yet
- Transfer Izusu DimaxDocument61 pagesTransfer Izusu DimaxArmando Useda100% (1)
- Manual Baja DB30 Racer Mini BikeDocument33 pagesManual Baja DB30 Racer Mini Bikemcswain99No ratings yet
- Hybrid Vehicle DrivetrainDocument16 pagesHybrid Vehicle DrivetrainRamesh BiradarNo ratings yet
- Spare Parts Catalog: 6 WG 210 Material Number: 4657.056.136 Current Date: 28.01.2019Document80 pagesSpare Parts Catalog: 6 WG 210 Material Number: 4657.056.136 Current Date: 28.01.2019Костя ДолинськийNo ratings yet
- N122 Text 2Document6 pagesN122 Text 2doodoobuttfartNo ratings yet
- Dynapac Cp2100 t3 Spare Parts CatalogueDocument20 pagesDynapac Cp2100 t3 Spare Parts Cataloguekevin100% (56)
- Farana ChecklistDocument1 pageFarana ChecklistJayendra NaiduNo ratings yet
- P-C Produkt-Katalog 2020 - LUB2097EDocument76 pagesP-C Produkt-Katalog 2020 - LUB2097ECAT CYLINDERNo ratings yet
- AraiDocument2 pagesAraiRanjit Kumar TANo ratings yet
- Gmax Service ManualDocument157 pagesGmax Service ManualBenny Kaysen SørensenNo ratings yet
- 6 Finisor de Asfalt Pe Senile Volvo Abg9820 47542Document6 pages6 Finisor de Asfalt Pe Senile Volvo Abg9820 47542Farkas Pal100% (1)
- GX30G Non EU (150113) - ??Document2 pagesGX30G Non EU (150113) - ??ggpetNo ratings yet
- Bolter 88 - ReseminDocument4 pagesBolter 88 - ReseminDonald MendozaNo ratings yet
- 1156 - TBCB - PRODUCT SHEET - Sumitomo PLT - Enhance LX2 - 1120Document2 pages1156 - TBCB - PRODUCT SHEET - Sumitomo PLT - Enhance LX2 - 1120Khalid RabbaniNo ratings yet
- RSNAV Installation ManualDocument21 pagesRSNAV Installation ManualDorin ValentinNo ratings yet
- DriftingDocument268 pagesDriftingRidho Satya Amanda100% (1)
- Free Go Kart PlansDocument28 pagesFree Go Kart PlansOsy OsyNo ratings yet
- B1 Apply Boost Valve Kit: Toyota/Lexus U760E, U760FDocument1 pageB1 Apply Boost Valve Kit: Toyota/Lexus U760E, U760FossoskiNo ratings yet
- Hermann Göring Assault Gun Battery: Tank CompanyDocument2 pagesHermann Göring Assault Gun Battery: Tank CompanyWojciech OlaszekNo ratings yet
- Riding MowerDocument68 pagesRiding Mowerfmpeb1No ratings yet
- 2001 Jaguar S-Type Drivers HandbookDocument5 pages2001 Jaguar S-Type Drivers Handbookyosemite_g3No ratings yet
- B810 PDFDocument384 pagesB810 PDFДмитрий100% (3)
- Cat Caminhao ArticuladoDocument2 pagesCat Caminhao ArticuladoTom SouzaNo ratings yet
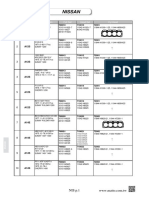
- NISSAN Engine Gasket Catalog 20190722Document25 pagesNISSAN Engine Gasket Catalog 20190722Anjas Sihombing100% (2)
- vx0202 C Commercial Vehicle CrossingDocument1 pagevx0202 C Commercial Vehicle Crossingshelvin.swamyNo ratings yet
- BYD and Its "Green City Solution"Document32 pagesBYD and Its "Green City Solution"tong kok hooi100% (1)
- Dominar 250 Bs6 Rev 07 Aug 22Document98 pagesDominar 250 Bs6 Rev 07 Aug 22Hiten Motors100% (1)