You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- OrderSets EcwDocument7 pagesOrderSets EcwbinduNo ratings yet
- Saba Dawood KhanDocument9 pagesSaba Dawood KhanSaba DawoodNo ratings yet
- 36.in The Case of Dangerous Goods Indicate Hazard Class/Div:Flash Point Containers Detail As Per Attached SheetDocument1 page36.in The Case of Dangerous Goods Indicate Hazard Class/Div:Flash Point Containers Detail As Per Attached SheetSaba DawoodNo ratings yet
- Marketing Research: Name: Saba Dawood Khan SP 17 - BBA-037Document4 pagesMarketing Research: Name: Saba Dawood Khan SP 17 - BBA-037Saba DawoodNo ratings yet
- Brand ManagementDocument5 pagesBrand ManagementSaba DawoodNo ratings yet
- 5th NAT 2014 FinalDocument1 page5th NAT 2014 FinalSaba DawoodNo ratings yet
- My Self: Saba Dawood KhanDocument2 pagesMy Self: Saba Dawood KhanSaba DawoodNo ratings yet
- Fee Challan: Comsats University Islamabad Abbottabad CampusDocument1 pageFee Challan: Comsats University Islamabad Abbottabad CampusSaba DawoodNo ratings yet
- Salomon V A Salomon & Co LTD: Saba KhanDocument10 pagesSalomon V A Salomon & Co LTD: Saba KhanSaba DawoodNo ratings yet
- Ports in The Fight Against COVID-19 - UNCTADDocument7 pagesPorts in The Fight Against COVID-19 - UNCTADNathalia HijuelosNo ratings yet
- Danish Study Shows No Benefit To Overall Mortality From mRNA VaccinesDocument13 pagesDanish Study Shows No Benefit To Overall Mortality From mRNA VaccinesJun KedNo ratings yet
- Everyone Wore Masks During The 1918 Flu Pandemic AND It Didn't HelpDocument4 pagesEveryone Wore Masks During The 1918 Flu Pandemic AND It Didn't HelpJusticeNo ratings yet
- Carlil v. Carbolic Smoke Ball CompanyDocument9 pagesCarlil v. Carbolic Smoke Ball CompanyBhumika M ShahNo ratings yet
- Pediatric ICD-10-CM Coding Tip Sheet: Overview of Key Chapter Updates For Pediatric and Top 25 CodesDocument4 pagesPediatric ICD-10-CM Coding Tip Sheet: Overview of Key Chapter Updates For Pediatric and Top 25 CodesAmerican Aesthetic MCNo ratings yet
- ARTICLE Zakialevel - DoxDocument12 pagesARTICLE Zakialevel - DoxZakia AmreenNo ratings yet
- Public Health 101 SeriesDocument58 pagesPublic Health 101 SeriesKiki Ari LarasNo ratings yet
- Influenza: DR.T .V.R Ao MDDocument81 pagesInfluenza: DR.T .V.R Ao MDtummalapalli venkateswara raoNo ratings yet
- Coronavirus COVID 19 - Immunity Modulation in Indian Context March 2020 English & Hindi VersionDocument3 pagesCoronavirus COVID 19 - Immunity Modulation in Indian Context March 2020 English & Hindi VersionLeo AudeNo ratings yet
- 1.2 Geometric Sequences: Example: A Flu EpidemicDocument1 page1.2 Geometric Sequences: Example: A Flu EpidemicreacharunkNo ratings yet
- Injection Site and Needle Size Vaccine Dose RouteDocument1 pageInjection Site and Needle Size Vaccine Dose RouteDoc JT BylnNo ratings yet
- Impact On Employee Workplace Organization of Covid 19Document90 pagesImpact On Employee Workplace Organization of Covid 19salmanNo ratings yet
- A Bad Case of StripesDocument2 pagesA Bad Case of StripesRadhika RathoreNo ratings yet
- Flu and COVID Vaccine Clinic Compilation Flyer 2023 V2Document1 pageFlu and COVID Vaccine Clinic Compilation Flyer 2023 V2WDIV/ClickOnDetroitNo ratings yet
- (Nakakaranas Ka Ba NG?) Masakit Lumunok) : Health Declaration TemperatureDocument1 page(Nakakaranas Ka Ba NG?) Masakit Lumunok) : Health Declaration TemperatureNatividad Jo Ann CuadroNo ratings yet
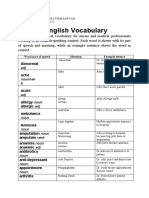
- Medical English Vocabulary: Abnormal AcheDocument8 pagesMedical English Vocabulary: Abnormal AcheRoby FirmansyahNo ratings yet
- Cytokine StormDocument1 pageCytokine StormLNo ratings yet
- Jose Rizal University: "Spanish Flu"Document17 pagesJose Rizal University: "Spanish Flu"Jericho DupayaNo ratings yet
- Chronology 2020Document12 pagesChronology 2020Watertown Daily TimesNo ratings yet
- Microbiology Research ProposalDocument5 pagesMicrobiology Research Proposalapi-547677741No ratings yet
- Vaccine Storage LabelsDocument17 pagesVaccine Storage LabelsNessax33No ratings yet
- The Autobiography of The Other Lady GagaDocument7 pagesThe Autobiography of The Other Lady GagaElenear De OcampoNo ratings yet
- Nov 4 09-Commencement1Document2 pagesNov 4 09-Commencement1kshaneNo ratings yet
- Medical Certificate For TravelDocument5 pagesMedical Certificate For TravelAugust Cherry MabbyNo ratings yet
- EHSA Dan Globalisasi Risiko KesehatanDocument77 pagesEHSA Dan Globalisasi Risiko KesehatanRian PuspitasariNo ratings yet
- Cyient-BCP - PandemicEvent - Annexure-6 - Candidate Declaration FormDocument2 pagesCyient-BCP - PandemicEvent - Annexure-6 - Candidate Declaration FormManoj EmmidesettyNo ratings yet
- Compound Exercise 2Document4 pagesCompound Exercise 2Hesty ZebuaNo ratings yet
- Mckinsey Briefing NoteDocument12 pagesMckinsey Briefing NoteGONE RAJASHEKERNo ratings yet
- Journal Reading: Anxiety Worry and Perceived Stress Due To Covid 19 PandemiDocument8 pagesJournal Reading: Anxiety Worry and Perceived Stress Due To Covid 19 PandemiAulia LatifahNo ratings yet