0% found this document useful (0 votes)
71 views5 pagesUnderstanding Diarrhea Pathophysiology
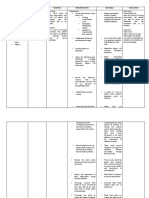
The document discusses the pathophysiology of diarrhea, including modifiable and non-modifiable risk factors, common etiologic agents, transmission routes, the invasion and destruction of the bowel wall by pathogens, and the resulting physiological effects including nausea, vomiting, fluid and electrolyte imbalance, dehydration, and increased bowel movements. It also provides a nursing care plan template addressing assessment, diagnosis, planning, intervention, rationale, and evaluation for a patient experiencing diarrhea related to excessive fluid and electrolyte loss.
Uploaded by
Hanna La MadridCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOC, PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
71 views5 pagesUnderstanding Diarrhea Pathophysiology
The document discusses the pathophysiology of diarrhea, including modifiable and non-modifiable risk factors, common etiologic agents, transmission routes, the invasion and destruction of the bowel wall by pathogens, and the resulting physiological effects including nausea, vomiting, fluid and electrolyte imbalance, dehydration, and increased bowel movements. It also provides a nursing care plan template addressing assessment, diagnosis, planning, intervention, rationale, and evaluation for a patient experiencing diarrhea related to excessive fluid and electrolyte loss.
Uploaded by
Hanna La MadridCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOC, PDF, TXT or read online on Scribd