You might also like
- Importance of Percutaneous Gastrojejunostomy (PEG-J) in Advance Parkinson Disease TreatmentDocument7 pagesImportance of Percutaneous Gastrojejunostomy (PEG-J) in Advance Parkinson Disease TreatmentRoxana AndreeaNo ratings yet
- Articol DuodopaDocument7 pagesArticol DuodopaRoxana AndreeaNo ratings yet
- 16) Facial Diplegia With ParesthesiaDocument2 pages16) Facial Diplegia With ParesthesiaRoxana AndreeaNo ratings yet
- 5) Moebius SyndromeDocument4 pages5) Moebius SyndromeRoxana AndreeaNo ratings yet
- 10) Guillain-Barre Syndrome, Neuroborreliosis, orDocument4 pages10) Guillain-Barre Syndrome, Neuroborreliosis, orRoxana AndreeaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Soccer Field Turf - FINAL - Dec - 1Document45 pagesSoccer Field Turf - FINAL - Dec - 1Yudhy NoviantoNo ratings yet
- English For Medical Research - CoursebookDocument168 pagesEnglish For Medical Research - CoursebookAndrіі DudashNo ratings yet
- Traffic Management PlanDocument2 pagesTraffic Management PlanSaifNo ratings yet
- Chemistry & SAR of QuinazolinoneDocument6 pagesChemistry & SAR of Quinazolinonebooksa2zNo ratings yet
- Siddha InstituteDocument10 pagesSiddha InstituteBala GanapathyNo ratings yet
- 2023 Haywood State of Black PA Report FINALDocument28 pages2023 Haywood State of Black PA Report FINALJohn L. MicekNo ratings yet
- الاشتريه في الوزاريات 6 اعدادي اشتر احمد 2023 كونيكاDocument132 pagesالاشتريه في الوزاريات 6 اعدادي اشتر احمد 2023 كونيكاSajad HussienNo ratings yet
- Solicitation Restroom MaintenanceDocument10 pagesSolicitation Restroom MaintenanceDarnel CayogNo ratings yet
- Fresh Air Camp Application 2010Document13 pagesFresh Air Camp Application 2010Morgan Memorial Goodwill IndustriesNo ratings yet
- sugarfilmSTS SalonDocument1 pagesugarfilmSTS SalonAlyana Mae SalonNo ratings yet
- Implementing Guidelines For The Conduct of Classes 21 22Document7 pagesImplementing Guidelines For The Conduct of Classes 21 22Ace ClarkNo ratings yet
- BS 3970-5-1990 - (2018-06-20 - 03-47-55 Am)Document16 pagesBS 3970-5-1990 - (2018-06-20 - 03-47-55 Am)Rankie ChoiNo ratings yet
- Managing Fear of Falling tcm44-37418Document15 pagesManaging Fear of Falling tcm44-37418Ioana MacarieNo ratings yet
- Handout Ms Prof. Ej FlaminianoDocument50 pagesHandout Ms Prof. Ej FlaminianoJustine Jacob BarengNo ratings yet
- SUPERVISOR: Dr. Sabar P. Siregar SP - KJDocument36 pagesSUPERVISOR: Dr. Sabar P. Siregar SP - KJPuspita PrihatiniNo ratings yet
- Communication Tools PDFDocument2 pagesCommunication Tools PDFRonaldNo ratings yet
- RevisionDocument3,216 pagesRevisionRylie RuuNo ratings yet
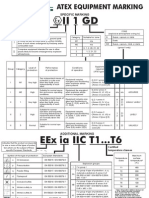
- Atex MarkingDocument1 pageAtex Markinggangotri05No ratings yet
- Handbook of Children With Special Health Care NeedsDocument443 pagesHandbook of Children With Special Health Care Needsحسين منصورNo ratings yet
- DNS - Sport III Part1Document6 pagesDNS - Sport III Part1jole000100% (1)
- Study - COMPETENCES - UDL, Gifted C, ADHD, Autism, Etc..Document10 pagesStudy - COMPETENCES - UDL, Gifted C, ADHD, Autism, Etc..angela castroNo ratings yet
- A Study On Psoriasis of Nails Severity Scoring SystemDocument4 pagesA Study On Psoriasis of Nails Severity Scoring SystemKhilyatul MufidaNo ratings yet
- Chapter 4 (Hazard Identification, Risk Assessment and Determining Control Part 1)Document33 pagesChapter 4 (Hazard Identification, Risk Assessment and Determining Control Part 1)agilaiswari manimaranNo ratings yet
- Ofw Information Sheet: Personal Data Change/s (If AnyDocument1 pageOfw Information Sheet: Personal Data Change/s (If AnyDan William BadiqueNo ratings yet
- Health and Social Care UkDocument5 pagesHealth and Social Care UkAkular AyramNo ratings yet
- Chapter 2: Population: The Cultural LandscapeDocument50 pagesChapter 2: Population: The Cultural LandscapeAlan nguyenNo ratings yet
- Week 16Document6 pagesWeek 16Sal MiahNo ratings yet
- Antiemesis NCCNDocument79 pagesAntiemesis NCCNana salazarNo ratings yet
- Antenatal Care (ANC)Document77 pagesAntenatal Care (ANC)tareNo ratings yet
- 4th Semester Mcqs of Evidence Based PracticesDocument5 pages4th Semester Mcqs of Evidence Based Practicesstudents bsn74% (19)