You might also like
- Clinical Pharmacy ReviewDocument8 pagesClinical Pharmacy Reviewsagar dhakalNo ratings yet
- Practice of Hospital Pharmacy in Bangladesh: Current PerspectiveDocument6 pagesPractice of Hospital Pharmacy in Bangladesh: Current PerspectiveMonalia Sadia Rahman Chowdhury 1811886649No ratings yet
- Pharmacist-Participated Medication Review in Different Practice Settings: Service or Intervention? An Overview of Systematic ReviewsDocument24 pagesPharmacist-Participated Medication Review in Different Practice Settings: Service or Intervention? An Overview of Systematic ReviewsIlham FudholiNo ratings yet
- PERCEPTIONDocument5 pagesPERCEPTIONFaizaNadeemNo ratings yet
- Your Guide To A Career in Pharmacy A Comprehensive OverviewFrom EverandYour Guide To A Career in Pharmacy A Comprehensive OverviewNo ratings yet
- Comparative Analysis of Pharmaceutical Care and TR PDFDocument6 pagesComparative Analysis of Pharmaceutical Care and TR PDFNimrah MughalNo ratings yet
- NIH Public Access: Author ManuscriptDocument21 pagesNIH Public Access: Author ManuscriptranNo ratings yet
- The Impact of Doctor-Pharma Relationships On Prescribing PracticeDocument7 pagesThe Impact of Doctor-Pharma Relationships On Prescribing PracticeAbdul Wajid Nazeer CheemaNo ratings yet
- Review of Pharmaceutical Care Services Provided by The PharmacistsDocument3 pagesReview of Pharmaceutical Care Services Provided by The PharmacistsellianaeyNo ratings yet
- Lecture Notes On Clinical Pharmacy SubjeDocument155 pagesLecture Notes On Clinical Pharmacy SubjeBhavana S MNo ratings yet
- Evaluation of General Practice Pharmacists: Study Protocol To Assess Interprofessional Collaboration and Team EffectivenessDocument14 pagesEvaluation of General Practice Pharmacists: Study Protocol To Assess Interprofessional Collaboration and Team EffectivenessDELA CRUZ, JOHN RIC A.No ratings yet
- Saskatchewan pharmacists' role in prescribing drugsDocument26 pagesSaskatchewan pharmacists' role in prescribing drugsDeviselvamNo ratings yet
- Clinical Pharmacist Role in Drug Information ServiDocument9 pagesClinical Pharmacist Role in Drug Information ServiDesalegn DansaNo ratings yet
- 17 - HEPLER, C - D - Clinical Pharmacy, Pharmaceutical Care, and The Quality of Drug TherapyDocument8 pages17 - HEPLER, C - D - Clinical Pharmacy, Pharmaceutical Care, and The Quality of Drug TherapyIndra PratamaNo ratings yet
- 1744-8603-8-12Document4 pages1744-8603-8-12Bheru BhatiNo ratings yet
- Pharmacy: Pharmacy Technicians' Roles and Responsibilities in The Community Pharmacy Sector: A Welsh PerspectiveDocument21 pagesPharmacy: Pharmacy Technicians' Roles and Responsibilities in The Community Pharmacy Sector: A Welsh Perspectiveokoye geraldNo ratings yet
- Article 6yCODocument14 pagesArticle 6yCOAychluhm TatekNo ratings yet
- Pharmaceutical Care Services in Hospitals of Kuwait: Abdelmoneim Awad, Shareefa Al-Ebrahim, Eman AbahussainDocument9 pagesPharmaceutical Care Services in Hospitals of Kuwait: Abdelmoneim Awad, Shareefa Al-Ebrahim, Eman AbahussainPen KinhNo ratings yet
- Role of community pharmacies in Indian healthcareDocument18 pagesRole of community pharmacies in Indian healthcarevijju006No ratings yet
- Pharmacy: Pharmacists Becoming Physicians: For Better or Worse?Document6 pagesPharmacy: Pharmacists Becoming Physicians: For Better or Worse?Vidho RiveraNo ratings yet
- Longitudinal Study of Good Pharmacy Practice Roles Covered at The Annual World Pharmacy Congresses 2003-2019Document14 pagesLongitudinal Study of Good Pharmacy Practice Roles Covered at The Annual World Pharmacy Congresses 2003-2019Tania MedianaNo ratings yet
- Jurnal PC 2Document22 pagesJurnal PC 2Dedi LihawaNo ratings yet
- Pharmacists and CommunicationDocument5 pagesPharmacists and CommunicationMichael BonettNo ratings yet
- The Role of Pharmacists in Developing Countries: A Case for Mixed Methods ResearchDocument8 pagesThe Role of Pharmacists in Developing Countries: A Case for Mixed Methods ResearchJvMascarinasNo ratings yet
- Multidisciplinary Team and Pharmacists Role in That TeamDocument5 pagesMultidisciplinary Team and Pharmacists Role in That TeamTimothy OgomaNo ratings yet
- Modified Pharmacy Counseling Improves Outpatient Short-Term Antibiotic Compliance in Bali ProvinceDocument10 pagesModified Pharmacy Counseling Improves Outpatient Short-Term Antibiotic Compliance in Bali ProvinceIJPHSNo ratings yet
- International Research Journal of PharmacyDocument5 pagesInternational Research Journal of PharmacyKoko DandashNo ratings yet
- Pharmacist Role in Healthcare TeamsDocument30 pagesPharmacist Role in Healthcare TeamsDes LumabanNo ratings yet
- PCB 513 - Pharmacists' Relationship With Other HealthDocument11 pagesPCB 513 - Pharmacists' Relationship With Other HealthPatrick AnthonyNo ratings yet
- Barriers To The Implementation of Pharmaceutical CDocument8 pagesBarriers To The Implementation of Pharmaceutical CRoaaNo ratings yet
- 2019 Article 816Document37 pages2019 Article 816Annafiatu zakiahNo ratings yet
- Pharmacology REPORTDocument19 pagesPharmacology REPORTPankaj SharmaNo ratings yet
- Clinical PharmacyDocument16 pagesClinical Pharmacyfike0% (1)
- Factors Affecting Prescribing BHR - Dar EselamDocument7 pagesFactors Affecting Prescribing BHR - Dar EselamWassie GetahunNo ratings yet
- Interprofessional Collaboration DDocument6 pagesInterprofessional Collaboration Dapi-628189095No ratings yet
- Article 7yCODocument11 pagesArticle 7yCOAychluhm TatekNo ratings yet
- Pharmaceutical Compounding: Recent Advances, Lessons Learned and Future PerspectivesDocument5 pagesPharmaceutical Compounding: Recent Advances, Lessons Learned and Future PerspectivesIsti IzzuddinNo ratings yet
- Pone 0241082Document12 pagesPone 0241082ochi rossyNo ratings yet
- Jurnal Konseling 1Document5 pagesJurnal Konseling 1Desi DamayantiNo ratings yet
- Inadequate Self-Care Behaviors Among Malaysian DiaDocument5 pagesInadequate Self-Care Behaviors Among Malaysian DiatikaNo ratings yet
- Regulatory Aspects of Pharmaceutical Quality System: Brief IntroductionFrom EverandRegulatory Aspects of Pharmaceutical Quality System: Brief IntroductionNo ratings yet
- Pharmacy 06 00037Document9 pagesPharmacy 06 00037Rosen AnthonyNo ratings yet
- DefinitionofcppDocument5 pagesDefinitionofcppMuhammad Baba GoniNo ratings yet
- Clinical PharmacyDocument7 pagesClinical PharmacyKabir ManchandaNo ratings yet
- Research in Social and Administrative Pharmacy: Tamara Koehler, Andrew BrownDocument6 pagesResearch in Social and Administrative Pharmacy: Tamara Koehler, Andrew BrownHarém OliveiraNo ratings yet
- Role of The Pharmacist in Antimicrobial Stewardship: Rachel Fortin, Pharmd, BcpsDocument2 pagesRole of The Pharmacist in Antimicrobial Stewardship: Rachel Fortin, Pharmd, BcpsSih AtiiNo ratings yet
- Social Pharmacy Assignment 2Document9 pagesSocial Pharmacy Assignment 2mdsahilkusugal17No ratings yet
- Introduction To Clinical PharmacyDocument32 pagesIntroduction To Clinical PharmacySuhail Ahmed SahitoNo ratings yet
- Perception of Nepalese Community Pharmacists Towards Patient Counseling and Continuing Pharmacy Education Program: A Multicentric StudyDocument7 pagesPerception of Nepalese Community Pharmacists Towards Patient Counseling and Continuing Pharmacy Education Program: A Multicentric StudySaval KhanalNo ratings yet
- The Impact of Clinical Pharmacists InterDocument7 pagesThe Impact of Clinical Pharmacists Interahmed1fkwnNo ratings yet
- Alarifi 2012Document8 pagesAlarifi 2012ekaNo ratings yet
- Re Iew Factors Affecting Rational DR G Se (RD), CO Liance and AstageDocument19 pagesRe Iew Factors Affecting Rational DR G Se (RD), CO Liance and Astagenadirakhalid143No ratings yet
- Medication AssignmentDocument5 pagesMedication Assignmentapi-525323558No ratings yet
- Curriculum Topics in PharmacyDocument7 pagesCurriculum Topics in PharmacyDonaldo Delvis DuddyNo ratings yet
- One Qualified Community Pharmacist Can Save One Community Within A NationDocument8 pagesOne Qualified Community Pharmacist Can Save One Community Within A NationHina liaquatNo ratings yet
- Clinical Pharmacy PracticeDocument5 pagesClinical Pharmacy PracticenuhaNo ratings yet
- Exploring The Knowledge and Attitude of Medical and Pharmacy Students About Generic Medicine in Lahore, PakistanDocument7 pagesExploring The Knowledge and Attitude of Medical and Pharmacy Students About Generic Medicine in Lahore, PakistanMathilda UllyNo ratings yet
- Pharmace Utical Care An Evolving Role at Community Pharmacies in PakistanDocument6 pagesPharmace Utical Care An Evolving Role at Community Pharmacies in PakistanrsbilalNo ratings yet
- Clinical PharmacyDocument16 pagesClinical Pharmacyblossoms_diyya299850% (6)
- Assessment of Appropriateness of Medical Prescriptions in Community Pharmacies and Adoption of WHO Prescribing IndicatorsDocument4 pagesAssessment of Appropriateness of Medical Prescriptions in Community Pharmacies and Adoption of WHO Prescribing IndicatorsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Literature Review of Public Relations in Public HealthcareDocument10 pagesA Literature Review of Public Relations in Public HealthcareFaizaNadeemNo ratings yet
- m2017 PDFDocument6 pagesm2017 PDFFaizaNadeemNo ratings yet
- Health Marketing QuarterlyDocument19 pagesHealth Marketing QuarterlyFaizaNadeemNo ratings yet
- 869 PDFDocument7 pages869 PDFFaizaNadeemNo ratings yet
- Public Relations & Health Care Mgt. 53-79-1-PB PDFDocument8 pagesPublic Relations & Health Care Mgt. 53-79-1-PB PDFshreyasi royNo ratings yet
- EarthquakeDocument1 pageEarthquakeFaizaNadeemNo ratings yet
- Khan 2013Document5 pagesKhan 2013FaizaNadeemNo ratings yet
- How Hospitals Use Social Media and Opportunities for Future EngagementDocument14 pagesHow Hospitals Use Social Media and Opportunities for Future EngagementFaizaNadeemNo ratings yet
- Sindhi culture explored through language, dress, music and nationalismDocument4 pagesSindhi culture explored through language, dress, music and nationalismFaizaNadeemNo ratings yet
- Ethical Issues in Mandatory Smallpox VaccinationDocument2 pagesEthical Issues in Mandatory Smallpox VaccinationFaizaNadeemNo ratings yet
- Coordination and Managerial CommunicationDocument18 pagesCoordination and Managerial CommunicationFaizaNadeemNo ratings yet
- Socializing, Orienting and Developing Employees: PART II: Training and DevelopmentDocument18 pagesSocializing, Orienting and Developing Employees: PART II: Training and DevelopmentFaizaNadeemNo ratings yet
- 869 PDFDocument7 pages869 PDFFaizaNadeemNo ratings yet
- Cureent ScenarioDocument6 pagesCureent Scenarionadiyya husnaNo ratings yet
- Semester Project Fall 2016: National University of Computer and Emerging Sciences Fundamentals of ManagementDocument39 pagesSemester Project Fall 2016: National University of Computer and Emerging Sciences Fundamentals of ManagementFaizaNadeem0% (1)
- About Raja Zia Ul HAQDocument5 pagesAbout Raja Zia Ul HAQFaizaNadeemNo ratings yet
- LIPOSOMESDocument53 pagesLIPOSOMESAlicia GarciaNo ratings yet
- 2720 9349 1 PBDocument5 pages2720 9349 1 PBEngr: Sarmad HussainNo ratings yet
- 36 SelfMedicationSurveyDocument5 pages36 SelfMedicationSurveyFaizaNadeemNo ratings yet
- Ethics 0993Document13 pagesEthics 0993FaizaNadeemNo ratings yet
- Pre Formulation StudiesDocument48 pagesPre Formulation StudiesFaizaNadeemNo ratings yet
- SDGs BookletDocument21 pagesSDGs BookletFabolos 9No ratings yet
- Risks of Self-Medication PracticesDocument28 pagesRisks of Self-Medication PracticesFaizaNadeemNo ratings yet
- Drug Utilization ReviewDocument7 pagesDrug Utilization ReviewFaizaNadeemNo ratings yet
- Dexamethasonetab PDFDocument8 pagesDexamethasonetab PDFFaizaNadeemNo ratings yet
- Islamic Practices in Daily LifeDocument15 pagesIslamic Practices in Daily LifeXee JayNo ratings yet
- Session Guide Sampling To Study Drug UseDocument7 pagesSession Guide Sampling To Study Drug UseFaizaNadeemNo ratings yet
- 2020 End Year 6 PenulisanDocument8 pages2020 End Year 6 PenulisanZulhillmi ZainuddinNo ratings yet
- Preparation of Starch Nanoparticles in A New Ionic Liquid-in-Oil MicroemulsionDocument12 pagesPreparation of Starch Nanoparticles in A New Ionic Liquid-in-Oil MicroemulsionPaula NancyNo ratings yet
- Providing Shelter and Safety: A Proposed Evacuation and Rehabilitation Center for Masbate CityDocument62 pagesProviding Shelter and Safety: A Proposed Evacuation and Rehabilitation Center for Masbate CityBenjamae MaqueNo ratings yet
- Water For Injections BP: What Is in This Leaflet?Document2 pagesWater For Injections BP: What Is in This Leaflet?Mohamed OmerNo ratings yet
- DL420 15c SpecificationsDocument4 pagesDL420 15c Specificationsesteban muñozNo ratings yet
- UNSG Report On Safety Security Humanitarian PersonnelDocument25 pagesUNSG Report On Safety Security Humanitarian PersonnelInterAction100% (1)
- Rotation: Medical Intensive Care Unit (South Campus) For Interns and ResidentsDocument6 pagesRotation: Medical Intensive Care Unit (South Campus) For Interns and ResidentsHashimIdreesNo ratings yet
- 3M Bio-Acoustic Simulator User Manual (053-012 Rev D)Document21 pages3M Bio-Acoustic Simulator User Manual (053-012 Rev D)rodrigocornejo81No ratings yet
- SanCoP7 AgendaDocument2 pagesSanCoP7 AgendaNicolaGreeneNo ratings yet
- Project 3 - Gas Turbine Tutorial - ChemCad Draft - 01 15 2020Document58 pagesProject 3 - Gas Turbine Tutorial - ChemCad Draft - 01 15 2020Daniel Andres Canro CalderónNo ratings yet
- BiostastisticDocument2 pagesBiostastisticاحمد ماجد زبنNo ratings yet
- MINDFULNESS CALENDARDocument1 pageMINDFULNESS CALENDARNiccy McOrrieNo ratings yet
- Shandong Lingong Wheel Loader LG956l Operation & Maintenance Manual Final 10.3.23Document130 pagesShandong Lingong Wheel Loader LG956l Operation & Maintenance Manual Final 10.3.23mliugong94% (16)
- Intro To GymnasticsDocument69 pagesIntro To GymnasticsMichaela Celerio50% (2)
- InfraTapp - Infra Tapp - Manual ENGDocument64 pagesInfraTapp - Infra Tapp - Manual ENGEliaNo ratings yet
- RN and LPN Scope of Practice GuideDocument6 pagesRN and LPN Scope of Practice Guidejenn1722No ratings yet
- REBA Employee Assessment Worksheet: A. Neck, Trunk and Leg AnalysisDocument1 pageREBA Employee Assessment Worksheet: A. Neck, Trunk and Leg AnalysisAgni JayantiNo ratings yet
- BW Mc2 XWHM y Na ManualDocument23 pagesBW Mc2 XWHM y Na ManualSatyasrinivas PulavarthiNo ratings yet
- Megawin: Numerical Over Current & Earth Fault RelayDocument16 pagesMegawin: Numerical Over Current & Earth Fault Relaynaran19794735100% (5)
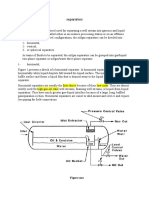
- Separators: Figure OneDocument8 pagesSeparators: Figure OneMohamed Moder100% (1)
- Indian Pharmacopiea 2007Document73 pagesIndian Pharmacopiea 2007Deepak ShahNo ratings yet
- Hepatitis Learning GuideDocument71 pagesHepatitis Learning Guidequimico clinico 27100% (10)
- Ramial Chipped Wood - A Basic Tool For Regenerating SoilsDocument15 pagesRamial Chipped Wood - A Basic Tool For Regenerating SoilsmrmiscNo ratings yet
- Derivatives and Risk ManagementDocument17 pagesDerivatives and Risk ManagementDeepak guptaNo ratings yet
- Color Me VeganDocument272 pagesColor Me VeganBela Luísa Novo100% (1)
- 342Mass&HeatModule (3) Soln071118 OlefinPlantDocument12 pages342Mass&HeatModule (3) Soln071118 OlefinPlantmanuelNo ratings yet
- May 4-22 Culinary 1 Lesson Plans PDFDocument4 pagesMay 4-22 Culinary 1 Lesson Plans PDFesefsdfsfNo ratings yet
- Mutual harm: The potential and risks of using allelopathic chemicals in agricultureDocument11 pagesMutual harm: The potential and risks of using allelopathic chemicals in agricultureMinh Anh NguyễnNo ratings yet
- NAVAL Hot Tapping Tool User GuideDocument19 pagesNAVAL Hot Tapping Tool User GuidemarconelucenapereiraNo ratings yet
- CSC 101-CSC 111 - Introduction To Computer Science - Lecture 1Document23 pagesCSC 101-CSC 111 - Introduction To Computer Science - Lecture 1CODE100% (1)