You might also like
- COPD 2 Management and Nursing CareDocument4 pagesCOPD 2 Management and Nursing CareAyman Nabil100% (1)
- Ensaio Clínico de Terapia Manual No Tratamento Da Condromalácia PatelarDocument4 pagesEnsaio Clínico de Terapia Manual No Tratamento Da Condromalácia PatelarLeticia ZaniniiNo ratings yet
- Journal of Carcinogenesis and Mutagenesis Research: Chemotherapy Pumps: Preparation and CounselingDocument5 pagesJournal of Carcinogenesis and Mutagenesis Research: Chemotherapy Pumps: Preparation and CounselingmochkurniawanNo ratings yet
- Injection TechniquesDocument7 pagesInjection TechniquesLheo AngelesNo ratings yet
- Tucker 2018Document8 pagesTucker 2018kosikevinonuNo ratings yet
- The Safe Use of Syringe Driver in Palliative CareDocument3 pagesThe Safe Use of Syringe Driver in Palliative CarecohenserbanNo ratings yet
- Comprehensive Geriatric Assessment For Older AdultsDocument3 pagesComprehensive Geriatric Assessment For Older Adultsdasty brownNo ratings yet
- Advances in Medical Nutrition TherapyDocument12 pagesAdvances in Medical Nutrition TherapyKabomed QANo ratings yet
- Parenteral KNPDocument126 pagesParenteral KNPHely PatelNo ratings yet
- 10 1089@jwh 2018 7391Document4 pages10 1089@jwh 2018 7391iqlimaikkeNo ratings yet
- Principles and Essential Techniques: Feline Gastrointestinal SurgeryDocument9 pagesPrinciples and Essential Techniques: Feline Gastrointestinal SurgeryKmii TspNo ratings yet
- The 2011 Infusion Nursing Standards of PracticeDocument12 pagesThe 2011 Infusion Nursing Standards of PracticeSugeng PrakosoNo ratings yet
- Mini-Nutritional Assessment (MNA) Is Useful For Assessing The Nutritional Status of Patients With Chronic Obstructive Pulmonary Disease: A Cross-Sectional StudyDocument8 pagesMini-Nutritional Assessment (MNA) Is Useful For Assessing The Nutritional Status of Patients With Chronic Obstructive Pulmonary Disease: A Cross-Sectional Studypanda louisNo ratings yet
- Safe Injection and Infusion Practices TraningDocument4 pagesSafe Injection and Infusion Practices TraningPRADIPNo ratings yet
- Avent Et Al-2011-Internal Medicine JournalDocument9 pagesAvent Et Al-2011-Internal Medicine JournalAgil Wahyu WicaksonoNo ratings yet
- The SUP-ICU Trial: Does It Confirm or Condemn The Practice of Stress Ulcer Prophylaxis?Document6 pagesThe SUP-ICU Trial: Does It Confirm or Condemn The Practice of Stress Ulcer Prophylaxis?Valentina Vasco YepesNo ratings yet
- Update On Nonantibiotic Therapies For Acute Gastroenteritis: ReviewDocument7 pagesUpdate On Nonantibiotic Therapies For Acute Gastroenteritis: ReviewKartikaa YantiiNo ratings yet
- NEC JA 16 p199Document7 pagesNEC JA 16 p199de la rosaNo ratings yet
- Chamberlain College of Nursing: Name: DateDocument6 pagesChamberlain College of Nursing: Name: DategabrielNo ratings yet
- The Role of Nurses in The Resuscitation of In-Hospital Cardiac ArrestsDocument5 pagesThe Role of Nurses in The Resuscitation of In-Hospital Cardiac ArrestsVerghese George MNo ratings yet
- Medicines Administration 1 Understanding Routes of AdministrationDocument3 pagesMedicines Administration 1 Understanding Routes of AdministrationJosa Camille BungayNo ratings yet
- TIVA Pocket Reference 2nd Edition (June 2013)Document42 pagesTIVA Pocket Reference 2nd Edition (June 2013)Charlene TanNo ratings yet
- Diaz Et Al 2019 Choosing a Mouse Model of Venous ThrombosisDocument8 pagesDiaz Et Al 2019 Choosing a Mouse Model of Venous Thrombosismudhra143No ratings yet
- PicotDocument8 pagesPicotapi-259267079No ratings yet
- SMP 3510 Heller Chapter34Document48 pagesSMP 3510 Heller Chapter34Ari DewiyantiNo ratings yet
- The Use of Smart Pumps and InformaticsDocument13 pagesThe Use of Smart Pumps and Informaticsapi-489685873No ratings yet
- Mobilization of Intensive Care Patients: A Multidisciplinary Practical Guide For CliniciansDocument10 pagesMobilization of Intensive Care Patients: A Multidisciplinary Practical Guide For CliniciansAsmaa GamalNo ratings yet
- Treatment Injury Case Study PDF Format TemplateDocument2 pagesTreatment Injury Case Study PDF Format TemplateASAD ULLAHNo ratings yet
- ACOG Practice Bulletin No 199 Use Of.67Document17 pagesACOG Practice Bulletin No 199 Use Of.67YtyNo ratings yet
- PS Solution7 PDFDocument3 pagesPS Solution7 PDFHerrySetiawanNo ratings yet
- Complementary and Alternative Medicine For Chronic Musculoskeletal PainDocument6 pagesComplementary and Alternative Medicine For Chronic Musculoskeletal PainDewi MurdaahNo ratings yet
- TIVA Paediatrics 2016 Booklet 1st EditionDocument28 pagesTIVA Paediatrics 2016 Booklet 1st EditionDoctorSajid BuzdarNo ratings yet
- 6759 25186 1 PBDocument8 pages6759 25186 1 PBPatricio LimaNo ratings yet
- Identify: Candidates CareDocument10 pagesIdentify: Candidates CareJHNo ratings yet
- Artigo TriagemDocument9 pagesArtigo TriagemTaiana CardosoNo ratings yet
- Standards of Medical Care in Diabetesd2019: 7. Diabetes TechnologyDocument53 pagesStandards of Medical Care in Diabetesd2019: 7. Diabetes TechnologyDanny Cumpa CapuñayNo ratings yet
- Ni Hms 765238Document18 pagesNi Hms 765238isabel pangNo ratings yet
- PicotDocument8 pagesPicotapi-259267079No ratings yet
- UIA 38 Safety PACUDocument5 pagesUIA 38 Safety PACUMelissa CadenaNo ratings yet
- 10 1111@anae 15291Document13 pages10 1111@anae 15291Ili RamosNo ratings yet
- BivalirudineDocument8 pagesBivalirudineGUSTAVOCRUZSUAREZ3845No ratings yet
- Paediatric Total Intravenous Anaesthesia BJA 2016Document5 pagesPaediatric Total Intravenous Anaesthesia BJA 2016RicardoNo ratings yet
- 2008 Intravenous Therapy, A Guide To Good PracticeDocument6 pages2008 Intravenous Therapy, A Guide To Good PracticeDaniela MéndezNo ratings yet
- FASTDRUGDELIVERYSYSTEMDocument11 pagesFASTDRUGDELIVERYSYSTEMGoal TargetNo ratings yet
- Antibiotic Stewardship Program (ASP) in Palliative Care: Antibiotics, To Give or Not To GiveDocument8 pagesAntibiotic Stewardship Program (ASP) in Palliative Care: Antibiotics, To Give or Not To GiveUriel EnriquezNo ratings yet
- Guiding Principles To Ensure Injection Device SecurityDocument2 pagesGuiding Principles To Ensure Injection Device SecurityAmeng GosimNo ratings yet
- The Impact of Frequent Injections For Hematopoietic Growth Factor Support On Patients Receiving Chemotherapy An Observational StudyDocument6 pagesThe Impact of Frequent Injections For Hematopoietic Growth Factor Support On Patients Receiving Chemotherapy An Observational StudyRachel CalditoNo ratings yet
- AntibioticsDocument17 pagesAntibioticsnainggolan Debora15No ratings yet
- Administering Drugs Via Enteral Feeding TubesDocument2 pagesAdministering Drugs Via Enteral Feeding TubesJohn Angelo BautistaNo ratings yet
- National Medication Safety Guidelines Manual: June 2013Document29 pagesNational Medication Safety Guidelines Manual: June 2013enik praNo ratings yet
- Anaesthesia - 2023 - Kinsella - Handling injectable medications in anaesthesiaDocument10 pagesAnaesthesia - 2023 - Kinsella - Handling injectable medications in anaesthesia177ervNo ratings yet
- ReferenceDocument11 pagesReferenceElfa Rizky KhafifahNo ratings yet
- Art. ENFit Enteral Nutrition ConnectionsDocument4 pagesArt. ENFit Enteral Nutrition Connectionscarlos enriqueNo ratings yet
- Organization Practices and Utilization Patterns of Intermediate Care Units Across the United StatesDocument4 pagesOrganization Practices and Utilization Patterns of Intermediate Care Units Across the United StatesJHNo ratings yet
- Syringes As Medical Devices: January 2017Document13 pagesSyringes As Medical Devices: January 2017Mahakaal KaalNo ratings yet
- EAUN15 Guideline Intravesical InstillationDocument90 pagesEAUN15 Guideline Intravesical InstillationRafael RojasNo ratings yet
- The Vortex Approach: Management of the Unanticipated Difficult AirwayFrom EverandThe Vortex Approach: Management of the Unanticipated Difficult AirwayRating: 5 out of 5 stars5/5 (1)
- Experience of Clinical Management for Pregnant Women and Newborns with Novel Coronavirus PneumoniaDocument5 pagesExperience of Clinical Management for Pregnant Women and Newborns with Novel Coronavirus PneumoniaDian NoveraNo ratings yet
- Mulisah PDFDocument7 pagesMulisah PDFMulisahNo ratings yet
- Li 2016Document5 pagesLi 2016nurharyanti darmaningtyasNo ratings yet
- Early Childhood Research Quarterly: Clancy Blair, Rachel D. Mckinnon, M. Paula DaneriDocument10 pagesEarly Childhood Research Quarterly: Clancy Blair, Rachel D. Mckinnon, M. Paula DaneriDian NoveraNo ratings yet
- JurnalDocument5 pagesJurnalDian NoveraNo ratings yet
- Early Childhood Research Quarterly: Clancy Blair, Rachel D. Mckinnon, M. Paula DaneriDocument10 pagesEarly Childhood Research Quarterly: Clancy Blair, Rachel D. Mckinnon, M. Paula DaneriDian NoveraNo ratings yet
- 3208 5876 1 SMDocument21 pages3208 5876 1 SMnirna maiziaNo ratings yet
- Canadian Journal of Psychiatry Aug 2006 51, 9 ProquestDocument1 pageCanadian Journal of Psychiatry Aug 2006 51, 9 ProquestDian NoveraNo ratings yet
- VIP 32 Hybrid VentDocument8 pagesVIP 32 Hybrid VentsagarNo ratings yet
- Determination of Atenolol in Pharmaceutical Dosages by Fourier Transform Infrared Spectrometry (FTIR)Document11 pagesDetermination of Atenolol in Pharmaceutical Dosages by Fourier Transform Infrared Spectrometry (FTIR)Geovas GomezNo ratings yet
- Su1 Assessment U01Document14 pagesSu1 Assessment U01Cristian Seas ArceNo ratings yet
- CB4 BBC Interviews EXTRA UnitDocument1 pageCB4 BBC Interviews EXTRA UnitCristianNo ratings yet
- All Creatures Great and SmallDocument4 pagesAll Creatures Great and SmallsaanviranjanNo ratings yet
- Map Project Rubric 2018Document2 pagesMap Project Rubric 2018api-292774341No ratings yet
- Retrenchment StrategiesDocument3 pagesRetrenchment StrategiesSABRI AKBAL MOHAMED HASSAN100% (3)
- Introduction to Globalization ExplainedDocument27 pagesIntroduction to Globalization ExplainedMichael Ron DimaanoNo ratings yet
- European Journal of Internal MedicineDocument4 pagesEuropean Journal of Internal Medicinesamer battatNo ratings yet
- Management Theory and Practice: Methods of Performance AppraisalDocument3 pagesManagement Theory and Practice: Methods of Performance AppraisalRadha maiNo ratings yet
- F FS1 Activity 3 EditedDocument15 pagesF FS1 Activity 3 EditedRayshane Estrada100% (1)
- Nitobond SBR (Latex)Document4 pagesNitobond SBR (Latex)Samarakoon Banda100% (1)
- Format of Synopsis - Project - 1Document5 pagesFormat of Synopsis - Project - 1euforia hubNo ratings yet
- Grab E-Receipt for 15,000 RP Ride on March 30Document1 pageGrab E-Receipt for 15,000 RP Ride on March 30WellyNo ratings yet
- Health Fitness Guide UK 2018 MayDocument100 pagesHealth Fitness Guide UK 2018 MayMitch Yeoh100% (2)
- Community HelpersDocument3 pagesCommunity Helpersapi-252790280100% (1)
- Internship Report Zannatul Ferdousi Alam YameemDocument51 pagesInternship Report Zannatul Ferdousi Alam YameemZannatul Ferdousi Alam YameemNo ratings yet
- Year 12 Holiday Homework Term 3Document4 pagesYear 12 Holiday Homework Term 3Lucas GauciNo ratings yet
- Ncm110nif Midterm Laboratory NotesDocument12 pagesNcm110nif Midterm Laboratory NotesMicah jay MalvasNo ratings yet
- 2iccas2005 Paper 377Document5 pages2iccas2005 Paper 377Cristian BandilaNo ratings yet
- DaburDocument3 pagesDaburchiru94No ratings yet
- Creating Literacy Instruction For All Students ResourceDocument25 pagesCreating Literacy Instruction For All Students ResourceNicole RickettsNo ratings yet
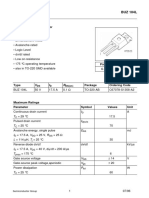
- Sipmos Power Transistor: BUZ 104LDocument10 pagesSipmos Power Transistor: BUZ 104LAlexsander MeloNo ratings yet
- Multibody Simulation of A Freight Bogie With Friction DampersDocument10 pagesMultibody Simulation of A Freight Bogie With Friction DampersGermán GoñiNo ratings yet
- DSC analysis of hair denaturationDocument2 pagesDSC analysis of hair denaturationDiosel Rezia PrazaNo ratings yet
- The Accidental AddictsDocument6 pagesThe Accidental AddictsnorthandsouthnzNo ratings yet
- Rg213 Rgflex Coax Braided Cable: Product Data Sheet RG213-50JFDocument1 pageRg213 Rgflex Coax Braided Cable: Product Data Sheet RG213-50JFPancho BerríosNo ratings yet
- Assessmentof Safety Cultureand Maturityin Mining Environments Caseof Njuli QuarryDocument12 pagesAssessmentof Safety Cultureand Maturityin Mining Environments Caseof Njuli QuarryAbdurrohman AabNo ratings yet
- Radio Drama (Rubric)Document1 pageRadio Drama (Rubric)Queenie BalitaanNo ratings yet
- What Is Your Road, Man?Document232 pagesWhat Is Your Road, Man?Oana AndreeaNo ratings yet