You might also like
- Fundamentals of Nursing Questionnaire With Answer Key (Lippincott Manual of Nursing Practice)Document6 pagesFundamentals of Nursing Questionnaire With Answer Key (Lippincott Manual of Nursing Practice)YujenNo ratings yet
- California Code Changes: 2022 TITLE 24 UpdatesDocument63 pagesCalifornia Code Changes: 2022 TITLE 24 UpdatesErika Wesso100% (2)
- Ethno NursingDocument5 pagesEthno NursingElmer OrganiaNo ratings yet
- 14 Steps To A Healthy LifestyleDocument3 pages14 Steps To A Healthy LifestyleLuise MauieNo ratings yet
- Population Health ManagementDocument7 pagesPopulation Health ManagementMimansa BhargavaNo ratings yet
- CC Concept Map FinalDocument8 pagesCC Concept Map Finalapi-593859653No ratings yet
- Assessing Knowledge, Attitude, and Practice of Diabetes Type 2 Patients Attending Keruguya Referral HospitalDocument10 pagesAssessing Knowledge, Attitude, and Practice of Diabetes Type 2 Patients Attending Keruguya Referral HospitalInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Drug Study: Phinma University of PangasinanDocument4 pagesDrug Study: Phinma University of PangasinanBrythym De GuzmanNo ratings yet
- Journal For MEdical WardDocument8 pagesJournal For MEdical WardValcrist BalderNo ratings yet
- Professional Nursing Research PaperDocument6 pagesProfessional Nursing Research Paperapi-357132774No ratings yet
- Nursing Diagnosis Analysis Goal/Objectives Intervention Rationale EvaluationDocument3 pagesNursing Diagnosis Analysis Goal/Objectives Intervention Rationale EvaluationLorraine Punla PanganNo ratings yet
- Iv Therapy With Edited RationaleDocument5 pagesIv Therapy With Edited RationaleKysha HuangNo ratings yet
- Community Assessment Windshield Survey - EditedDocument8 pagesCommunity Assessment Windshield Survey - EditedGeorge OwuorNo ratings yet
- How to recognize and treat chokingDocument29 pagesHow to recognize and treat chokingTamajong Tamajong PhilipNo ratings yet
- Head Nursing: University of Cebu - BaniladDocument30 pagesHead Nursing: University of Cebu - BaniladVjay DingNo ratings yet
- GI BleedDocument28 pagesGI BleedAnn Lan100% (1)
- Drug Study Drug Name Classificatio N Dosage/ Prepatarion Indication Contraindication Side Effects Nursing ResponsibilitiesDocument4 pagesDrug Study Drug Name Classificatio N Dosage/ Prepatarion Indication Contraindication Side Effects Nursing ResponsibilitiesTheresa AbrilloNo ratings yet
- Orientation On Community Health - Doh Programs & ServicesDocument11 pagesOrientation On Community Health - Doh Programs & ServicesAudrey Beatrice ReyesNo ratings yet
- Clabsi101 508Document53 pagesClabsi101 508Arjun KumarNo ratings yet
- Oral Care & Ventilator Acquired PneumoniaDocument14 pagesOral Care & Ventilator Acquired Pneumoniaapi-211614689No ratings yet
- Adult Care Plan Impair Gas ExchangeDocument2 pagesAdult Care Plan Impair Gas ExchangeVic DangNo ratings yet
- SKILL 8-16 Drawing Blood From A Central Venous Catheter: Key TermsDocument7 pagesSKILL 8-16 Drawing Blood From A Central Venous Catheter: Key TermsElizalde HusbandNo ratings yet
- IV TherapyDocument86 pagesIV TherapyAllyssa Leila Estrebillo OrbeNo ratings yet
- GC Geria Tool-Module1Document12 pagesGC Geria Tool-Module1Patricia Mae MirandaNo ratings yet
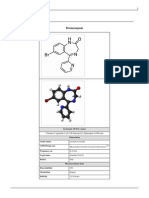
- BromazepamDocument6 pagesBromazepamMariusNeicuNo ratings yet
- Infections in ICUDocument7 pagesInfections in ICUNikolay ToméNo ratings yet
- Nursing Care PlanDocument1 pageNursing Care PlanDaisy PacoNo ratings yet
- Guide To IV SolutionsDocument1 pageGuide To IV SolutionsKim BadillesNo ratings yet
- Procedure-Nasogastric Tube InsertionDocument22 pagesProcedure-Nasogastric Tube Insertionmohamad dildarNo ratings yet
- Nurse's Role in Multidisciplinary Stroke CareDocument12 pagesNurse's Role in Multidisciplinary Stroke CareLauren GatesNo ratings yet
- Tubo-Ovarian Abscess - Contemporary Approach To ManagementDocument9 pagesTubo-Ovarian Abscess - Contemporary Approach To ManagementDanny. JayNo ratings yet
- Data Collection and Patient DiagnosisDocument14 pagesData Collection and Patient DiagnosisJen CareyNo ratings yet
- COPAR Community Outreach ProgramDocument5 pagesCOPAR Community Outreach ProgramKrizza Edejer TrillanaNo ratings yet
- Community Health Nursing Laws PhilippinesDocument6 pagesCommunity Health Nursing Laws PhilippinesAlhaisa BejemilNo ratings yet
- Final ResearchDocument65 pagesFinal ResearchHarbrinder GurmNo ratings yet
- Historical Aspects of Nursing InformaticsDocument5 pagesHistorical Aspects of Nursing InformaticsaxlzekeNo ratings yet
- Narrative PathophysiologyDocument5 pagesNarrative Pathophysiologymyer pasandalanNo ratings yet
- Chronic Kidney DiseaseDocument17 pagesChronic Kidney DiseaseJuanchi INNo ratings yet
- Nursing Management of Common Skin and Parasitic DiseasesDocument14 pagesNursing Management of Common Skin and Parasitic Diseasesyer tagalajNo ratings yet
- ElectrocardiogramDocument3 pagesElectrocardiogramladydreamer_92No ratings yet
- Clonidine Hydro ChlorideDocument4 pagesClonidine Hydro Chlorideapi-3797941100% (1)
- Subjectives: Short Term Independent: Short TermDocument13 pagesSubjectives: Short Term Independent: Short TermMarlo Dañez NorbeNo ratings yet
- Nursing Care PlanDocument2 pagesNursing Care PlanMiar QuestNo ratings yet
- Electronic Discharge LetterDocument14 pagesElectronic Discharge LetterHDrachslerNo ratings yet
- Nurse's Safety Attitudes As Perceived by Geriatric Patients in Homecare InstitutionsDocument16 pagesNurse's Safety Attitudes As Perceived by Geriatric Patients in Homecare InstitutionsGlobal Research and Development ServicesNo ratings yet
- Sleep Fundamental of NursingDocument6 pagesSleep Fundamental of NursingTono NsNo ratings yet
- PHIE1012015 MasterDocument10 pagesPHIE1012015 MasterDOH-EAMC medicalrecordsNo ratings yet
- Sas 21Document4 pagesSas 21Sistine Rose LabajoNo ratings yet
- Adolescent Nutrition Final CountdownDocument18 pagesAdolescent Nutrition Final CountdownNicole Denise PortugalezaNo ratings yet
- Knowledge and Practices of Nurses in Infection Prevention and Control Within A Tertiary Care HospitalDocument4 pagesKnowledge and Practices of Nurses in Infection Prevention and Control Within A Tertiary Care HospitalAnonymous TzvMOnNo ratings yet
- Community Health Profile of Barangay DimagibaDocument184 pagesCommunity Health Profile of Barangay Dimagibastephanie valerioNo ratings yet
- Maternal and Child Health Nursing, 8 Edition.: LESSON PREVIEW/REVIEW (5 Minutes)Document7 pagesMaternal and Child Health Nursing, 8 Edition.: LESSON PREVIEW/REVIEW (5 Minutes)raker boiNo ratings yet
- Communicable Disease NursingDocument22 pagesCommunicable Disease NursingNur SanaaniNo ratings yet
- Leukopenia and Bone Marrow TransplantationDocument20 pagesLeukopenia and Bone Marrow Transplantationdhanya jayanNo ratings yet
- Integumentary ManagementDocument25 pagesIntegumentary ManagementAlyssa MontimorNo ratings yet
- Propofol Drug StudyDocument3 pagesPropofol Drug Studygersalia.christiennikkiNo ratings yet
- Legal Aspects and The NurseDocument50 pagesLegal Aspects and The NurseClark Lim100% (1)
- Pediatrics: Stages of Development and GrowthDocument9 pagesPediatrics: Stages of Development and GrowthNur SanaaniNo ratings yet
- Hyponatremia and Hypernatremia in The ElderlyDocument15 pagesHyponatremia and Hypernatremia in The ElderlyStacey WoodsNo ratings yet
- Mesna: Mesna, Sold Under The BrandDocument17 pagesMesna: Mesna, Sold Under The BrandAndry HamdaniNo ratings yet
- The Community as Client: Assessment and DiagnosisDocument43 pagesThe Community as Client: Assessment and DiagnosisAbid HussainNo ratings yet
- Kontrak Belajar Gadar Igd BaruDocument14 pagesKontrak Belajar Gadar Igd BaruAstridNo ratings yet
- 1 Nursing Process AssessmentDocument28 pages1 Nursing Process AssessmentAyman NabilNo ratings yet
- 7 - Updated My Plate, Revised 2016Document15 pages7 - Updated My Plate, Revised 2016Ayman NabilNo ratings yet
- Immobility Studnets ObjectivesDocument3 pagesImmobility Studnets ObjectivesAyman NabilNo ratings yet
- Patient His Initial Name Is (AS) and The Patient Is Male. HeDocument29 pagesPatient His Initial Name Is (AS) and The Patient Is Male. HeAyman NabilNo ratings yet
- Glossary List - Terms Related To Vital SignsDocument5 pagesGlossary List - Terms Related To Vital SignsAyman NabilNo ratings yet
- Clustering Data Sheet and Concept Map and Nursing Care Plan HypertensionDocument4 pagesClustering Data Sheet and Concept Map and Nursing Care Plan HypertensionAyman NabilNo ratings yet
- Final syllabus-NU101-1-3-2021 Students Version PDFDocument17 pagesFinal syllabus-NU101-1-3-2021 Students Version PDFAyman NabilNo ratings yet
- Hypertension Session Student ObjectivesDocument2 pagesHypertension Session Student ObjectivesAyman NabilNo ratings yet
- Clustering Data Sheet and Concept Map and Nursing Care Plan PosteopreativeDocument4 pagesClustering Data Sheet and Concept Map and Nursing Care Plan PosteopreativeAyman NabilNo ratings yet
- Group 1 Parkinsons Pre TestDocument4 pagesGroup 1 Parkinsons Pre TestAyman NabilNo ratings yet
- Circulation Preparation SheetDocument3 pagesCirculation Preparation SheetAyman NabilNo ratings yet
- 3.07.00.simulation Lab Policy - Approved210217Document10 pages3.07.00.simulation Lab Policy - Approved210217Ayman NabilNo ratings yet
- Clustering Data Sheet and Concept Map and Nursing Care Plan ParkonsonsDocument3 pagesClustering Data Sheet and Concept Map and Nursing Care Plan ParkonsonsAyman NabilNo ratings yet
- Clustering Data Sheet and Concept Map and Nursing Care Plan HTNDocument4 pagesClustering Data Sheet and Concept Map and Nursing Care Plan HTNAyman NabilNo ratings yet
- Clustering Data Sheet and Concept Map and Nursing Care Plan SKINDocument4 pagesClustering Data Sheet and Concept Map and Nursing Care Plan SKINAyman NabilNo ratings yet
- Clinical Lab Safety GuidlinesDocument9 pagesClinical Lab Safety GuidlinesAyman NabilNo ratings yet
- Clustering Data Sheet and Concept Map and Nursing Care Plan HTNDocument4 pagesClustering Data Sheet and Concept Map and Nursing Care Plan HTNAyman NabilNo ratings yet
- MUST Malnutrition Universal Screening Tool PDFDocument6 pagesMUST Malnutrition Universal Screening Tool PDFHoria CostrutNo ratings yet
- Case Study 1Document3 pagesCase Study 1Ayman NabilNo ratings yet
- Case Study Parkinsonism 2019 StudentDocument3 pagesCase Study Parkinsonism 2019 StudentAyman NabilNo ratings yet
- Flore InceDocument1 pageFlore InceAyman NabilNo ratings yet
- Anticoagulation Booklet Tumble Eng Jan 2014Document12 pagesAnticoagulation Booklet Tumble Eng Jan 2014Ayman NabilNo ratings yet
- BuseJohnBVoraJi 2012 Chapter1WhereDoesInsu EvidenceBasedManagemeDocument20 pagesBuseJohnBVoraJi 2012 Chapter1WhereDoesInsu EvidenceBasedManagemeAyman NabilNo ratings yet
- AymanDocument3 pagesAymanAyman NabilNo ratings yet
- Prevention of Foodborne Disease: The Five Keys To Safer FoodDocument2 pagesPrevention of Foodborne Disease: The Five Keys To Safer FoodZubda ButtNo ratings yet
- NU101 Foundations of Nursing Practice Fluid and Electrolytes Balance Glossary List of Important TermsDocument3 pagesNU101 Foundations of Nursing Practice Fluid and Electrolytes Balance Glossary List of Important TermsAyman NabilNo ratings yet
- "It Made Me Dizzy and I Kept Getting Up During The Night To Empty My Bladder.", "I've Never Smoked and I Don't DrinkDocument1 page"It Made Me Dizzy and I Kept Getting Up During The Night To Empty My Bladder.", "I've Never Smoked and I Don't DrinkAyman NabilNo ratings yet
- Health Teaching For Fluid RestrictionDocument1 pageHealth Teaching For Fluid RestrictionAyman NabilNo ratings yet
- Final Mobility Skill Preparation Sheet3Document5 pagesFinal Mobility Skill Preparation Sheet3Ayman NabilNo ratings yet
- Full Download Olds Maternal Newborn Nursing and Womens Health Across The Lifespan 10th Edition Davidson Test BankDocument13 pagesFull Download Olds Maternal Newborn Nursing and Womens Health Across The Lifespan 10th Edition Davidson Test Bankshandybrady100% (40)
- Guidelines FOR Implementing Drug Utilization Review Programs IN HospitalsDocument58 pagesGuidelines FOR Implementing Drug Utilization Review Programs IN HospitalsMuhammad Faris MahmudNo ratings yet
- MODULE 2: Nursing Theorists & Theory 2021: Module Title Module No. Total Study Hours Module Writer/sDocument10 pagesMODULE 2: Nursing Theorists & Theory 2021: Module Title Module No. Total Study Hours Module Writer/sNavora, Bryle TrixthaneNo ratings yet
- Mianwali 1Document104 pagesMianwali 1asstt_dir_pndNo ratings yet
- BSN Curriculum 20 21 English 1Document3 pagesBSN Curriculum 20 21 English 1ROSE DIVINAGRACIANo ratings yet
- Nursing Care Plan For PalliaDocument13 pagesNursing Care Plan For Palliakarl_poorNo ratings yet
- Kolaborasi Interprofesional - DR - Dr.pritaDocument53 pagesKolaborasi Interprofesional - DR - Dr.pritaNanik MaskunatinNo ratings yet
- Windshield SurveyDocument7 pagesWindshield Surveyapi-241238306No ratings yet
- Health Promotion Test QuestionsDocument5 pagesHealth Promotion Test QuestionsAyesha khanNo ratings yet
- Hospital Incident and Accident ReportingDocument17 pagesHospital Incident and Accident ReportingSachin Singh100% (1)
- NVPC - Elderly PDFDocument2 pagesNVPC - Elderly PDFAlex WangNo ratings yet
- Care of Adults 24 Adult and Older Adult DevelopmentDocument29 pagesCare of Adults 24 Adult and Older Adult DevelopmentGaras AnnaBerniceNo ratings yet
- Jurisprudence (NLE)Document3 pagesJurisprudence (NLE)Maginalyn CangasNo ratings yet
- SWOT AnalysisDocument9 pagesSWOT AnalysisAshraf Ali Smadi88% (24)
- Research ProposalDocument26 pagesResearch ProposalLOGESWARRY K.VESUPATHYNo ratings yet
- Nyeri Akut dan Nutrisi KurangDocument73 pagesNyeri Akut dan Nutrisi KurangYuniar Valentine Putri PratiwiNo ratings yet
- NEWS2 Chart 4 - Clinical Response To NEWS Trigger Thresholds - 0 PDFDocument1 pageNEWS2 Chart 4 - Clinical Response To NEWS Trigger Thresholds - 0 PDFFlouria Stefanny SimatupangNo ratings yet
- X Disease Prevention XDocument6 pagesX Disease Prevention XDivya VarsiniNo ratings yet
- The Patient%u2019s Experience With Critical IllnessDocument15 pagesThe Patient%u2019s Experience With Critical IllnessineNo ratings yet
- HND Medical ScienceDocument588 pagesHND Medical Sciencembabit leslieNo ratings yet
- Evaluation and FHSISDocument6 pagesEvaluation and FHSISShara SampangNo ratings yet
- Spirituality in Health AssessmentDocument12 pagesSpirituality in Health Assessmentapi-491774875No ratings yet
- Nursing 2015Document12 pagesNursing 2015Rachel VictorianaNo ratings yet
- Case Study 17th July 2021Document1 pageCase Study 17th July 2021sivakamasundari pichaipillaiNo ratings yet
- AnxietyDocument2 pagesAnxietyikoiNo ratings yet
- Nursing Care Plan for Skeletal Traction PatientDocument3 pagesNursing Care Plan for Skeletal Traction PatientMarshin Thea CelociaNo ratings yet
- Apa Paper 2nd SemesterDocument5 pagesApa Paper 2nd Semesterapi-268209871No ratings yet
- Booklet For of Florence NightingaleDocument3 pagesBooklet For of Florence NightingaleSopan ShindeNo ratings yet