You might also like
- The Wim Hof Method - Wim HofDocument13 pagesThe Wim Hof Method - Wim Hofrichard dickison100% (10)
- Jake Yvan Dizon Case Study, Chapter 49, Assessment and Management of Patients With Hepatic DisordersDocument8 pagesJake Yvan Dizon Case Study, Chapter 49, Assessment and Management of Patients With Hepatic DisordersJake Yvan DizonNo ratings yet
- RLEFand ECSDocument3 pagesRLEFand ECSPaul JacksonNo ratings yet
- Scenario: Respiratory DisordersDocument4 pagesScenario: Respiratory DisordersPremiums of the RoseNo ratings yet
- Urinary Tract Infection Nursing-Care-PlanDocument3 pagesUrinary Tract Infection Nursing-Care-PlanRnspeakcomNo ratings yet
- Bronchial Artery Embolization: DR Tinku JosephDocument51 pagesBronchial Artery Embolization: DR Tinku JosephRadison sierraNo ratings yet
- Elena Ocyo (Pedia - NCP)Document3 pagesElena Ocyo (Pedia - NCP)elle leliNo ratings yet
- PneumoniaDocument2 pagesPneumoniaPia MedinaNo ratings yet
- Orientation On Community Health - Doh Programs & ServicesDocument11 pagesOrientation On Community Health - Doh Programs & ServicesAudrey Beatrice ReyesNo ratings yet
- HypertensionDocument3 pagesHypertensionkarl de guzmanNo ratings yet
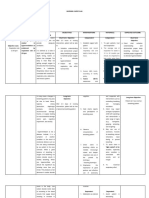
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationJustine Mae A. LoriaNo ratings yet
- Nursing Care Plan: Assessment Diagnosis Inference Goal Intervention Rationale EvaluationDocument4 pagesNursing Care Plan: Assessment Diagnosis Inference Goal Intervention Rationale EvaluationSugar Capule - ManuelNo ratings yet
- PCM Mock Test 16 December 2012Document3,924 pagesPCM Mock Test 16 December 2012goyaltarunNo ratings yet
- Subjective: Elevated Blood Glucose STO: After 4 Hours of Independent: STO: After 4 Hours ofDocument9 pagesSubjective: Elevated Blood Glucose STO: After 4 Hours of Independent: STO: After 4 Hours ofDacillo GailleNo ratings yet
- Group Work 3 - Nutrition Care ProcessDocument3 pagesGroup Work 3 - Nutrition Care Processcharles estradaNo ratings yet
- NCP On DyspneaDocument5 pagesNCP On DyspneaDizzy BualanNo ratings yet
- Kardex (MW 2)Document3 pagesKardex (MW 2)Aubrey Unique EvangelistaNo ratings yet
- Sas 21Document4 pagesSas 21Sistine Rose LabajoNo ratings yet
- NCP Active SeizureDocument4 pagesNCP Active SeizureAngelica CorpuzNo ratings yet
- Community Health Nursing-1 Unit 2Document52 pagesCommunity Health Nursing-1 Unit 2Asif Ali LashariNo ratings yet
- Student NurseDocument2 pagesStudent NurseTAYABAN, KENNETH JAKE, Q.No ratings yet
- Vasculitis 1Document2 pagesVasculitis 1PAMELA CASTILLONo ratings yet
- JDM Care PlanDocument5 pagesJDM Care PlangopscharanNo ratings yet
- Repaso 1 Anatomy Andominal Wall 0 CavityDocument7 pagesRepaso 1 Anatomy Andominal Wall 0 CavityAngelitza AlmodóvarNo ratings yet
- Problem Nursing Diagnosis Background Knowledge Goal and Objective Nursing Intervention Rationale EvaluationDocument2 pagesProblem Nursing Diagnosis Background Knowledge Goal and Objective Nursing Intervention Rationale Evaluationcherrymae mataNo ratings yet
- Assessment Diagnosis Planning Nursing Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Planning Nursing Intervention Rationale Evaluationjennelyn losantaNo ratings yet
- Nursing Care PlanDocument1 pageNursing Care PlanMikki lor PuaganNo ratings yet
- 6 Nursing Care Plan 1Document2 pages6 Nursing Care Plan 1Denise Louise PoNo ratings yet
- Assessment Nursing Diagnosis Outcome Identification Planning Nursing Intervention Evaluation IndependentDocument7 pagesAssessment Nursing Diagnosis Outcome Identification Planning Nursing Intervention Evaluation IndependentQueenie Silva100% (1)
- Ineffective Airway Clearance CareplanDocument6 pagesIneffective Airway Clearance CareplanderreshaNo ratings yet
- Acutepain RevisedDocument3 pagesAcutepain RevisedAndrea AutorNo ratings yet
- A Case Study of A 1-Year-Old Child Diagnosed With Bronchial Asthma in Acute ExacerbationDocument36 pagesA Case Study of A 1-Year-Old Child Diagnosed With Bronchial Asthma in Acute ExacerbationKyra Bianca R. FamacionNo ratings yet
- Risk For IneffectiveDocument6 pagesRisk For IneffectiveAce FabrigasNo ratings yet
- Planning 3 NCPSDocument5 pagesPlanning 3 NCPSCuttie Anne GalangNo ratings yet
- NCP Copd AirwayDocument2 pagesNCP Copd AirwaySugar Capule - ManuelNo ratings yet
- Ineffective Coping NCPDocument4 pagesIneffective Coping NCPFrancis Alfred EscaranNo ratings yet
- A Buddhist Perspective On Health and SpiritualityDocument3 pagesA Buddhist Perspective On Health and Spiritualityedi_wsNo ratings yet
- Nursing Care PlanDocument3 pagesNursing Care PlanCindy MariscotesNo ratings yet
- NCP Decreased Cardiac OutputDocument2 pagesNCP Decreased Cardiac OutputYamete KudasaiNo ratings yet
- Prepared By: Rashmi Regmi B. SC Nursing Manmohan Memorial Institute of Health SciencesDocument93 pagesPrepared By: Rashmi Regmi B. SC Nursing Manmohan Memorial Institute of Health SciencesNinaNo ratings yet
- Cues Nursing Diagnosis Scientific Rationale Objectives Intervention Rationale Evaluation IndependentDocument6 pagesCues Nursing Diagnosis Scientific Rationale Objectives Intervention Rationale Evaluation IndependentKasandra Dawn Moquia Beriso100% (1)
- Nursing Care Plan On Platelet DisordersDocument8 pagesNursing Care Plan On Platelet DisordersbhavanaNo ratings yet
- NCP PTBDocument6 pagesNCP PTBJay Dela VegaNo ratings yet
- NURSING CARE PLAN - Impaired Urinary EliminationDocument2 pagesNURSING CARE PLAN - Impaired Urinary EliminationDaniel Andre S. SomorayNo ratings yet
- Journal For MEdical WardDocument8 pagesJournal For MEdical WardValcrist BalderNo ratings yet
- Quality of Prenatal Care Questionnaire: Instrument Development and TestingDocument17 pagesQuality of Prenatal Care Questionnaire: Instrument Development and TestingGreat CoassNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument9 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationYzel Vasquez AdavanNo ratings yet
- Dosage: 50 MG Order: PRN q6h Route: IV (Case Scenario Based)Document3 pagesDosage: 50 MG Order: PRN q6h Route: IV (Case Scenario Based)Edward Luis EsguerraNo ratings yet
- NCP ReviseDocument7 pagesNCP ReviseRhobic ManansalaNo ratings yet
- Ortho NCPDocument3 pagesOrtho NCPMarshin Thea CelociaNo ratings yet
- Ineffective Breathing Pattern Related To HyperventilationDocument4 pagesIneffective Breathing Pattern Related To HyperventilationVanessa Charlotte LagunayNo ratings yet
- Ariane NCP 1Document2 pagesAriane NCP 1Kristian Ray EraulaNo ratings yet
- Drug Dosage Mechanism of Action Indications & Contraindications Side Effects & Adverse Effects Nursing ResponsibilityDocument1 pageDrug Dosage Mechanism of Action Indications & Contraindications Side Effects & Adverse Effects Nursing ResponsibilityAthena SaturdayNo ratings yet
- Name of Drug Classification and Mode of Action Adverse Effects/precautions Nursing ConsiderationsDocument3 pagesName of Drug Classification and Mode of Action Adverse Effects/precautions Nursing ConsiderationsDyanne BautistaNo ratings yet
- Nursing Care Plan Assessment Diagnosis Inference Planning Intervention Rationale Evaluation Subjective: Short Term: Independent: Goal MetDocument4 pagesNursing Care Plan Assessment Diagnosis Inference Planning Intervention Rationale Evaluation Subjective: Short Term: Independent: Goal MetKiana OcampoNo ratings yet
- Nursing Care Plan Patient's Name: L. Fajardo Age: 19 Y.O AddressDocument3 pagesNursing Care Plan Patient's Name: L. Fajardo Age: 19 Y.O AddressLeticia ElricNo ratings yet
- Premenstrual Dysphoric DisorderDocument11 pagesPremenstrual Dysphoric Disorderapi-3764215No ratings yet
- Group 9 Sickle Cell Anemia Case Study ActivityDocument4 pagesGroup 9 Sickle Cell Anemia Case Study ActivityJuliaNo ratings yet
- Assessment Diagnosis Planning Interventions Rationale Evaluation Subjective Data: Short Term Independent: Short TermDocument14 pagesAssessment Diagnosis Planning Interventions Rationale Evaluation Subjective Data: Short Term Independent: Short TermMarlo Dañez NorbeNo ratings yet
- IPPA SampleDocument28 pagesIPPA Samplekimglaidyl bontuyanNo ratings yet
- Scenario 4 - NCPDocument15 pagesScenario 4 - NCPVian RiveraNo ratings yet
- NCPDocument7 pagesNCPRuth MontebonNo ratings yet
- Peda Ruell BioCDocument2 pagesPeda Ruell BioCMarlo Dañez NorbeNo ratings yet
- Marlo Norbe BSN4A NCM19 Org - StructureDocument1 pageMarlo Norbe BSN4A NCM19 Org - StructureMarlo Dañez NorbeNo ratings yet
- Norbe Group3SetA Medicine Week1 Requirements.Document23 pagesNorbe Group3SetA Medicine Week1 Requirements.Marlo Dañez NorbeNo ratings yet
- NORBE BSN4A Midterm Activity 1Document2 pagesNORBE BSN4A Midterm Activity 1Marlo Dañez NorbeNo ratings yet
- Norbe Bsn4a Example of PropositionDocument6 pagesNorbe Bsn4a Example of PropositionMarlo Dañez NorbeNo ratings yet
- Norbe Marlo BSN2A PEDIA-CYSTIC-FIBROSISDocument2 pagesNorbe Marlo BSN2A PEDIA-CYSTIC-FIBROSISMarlo Dañez NorbeNo ratings yet
- Activity 1: Recognizing Ethical ProblemsDocument3 pagesActivity 1: Recognizing Ethical ProblemsMarlo Dañez NorbeNo ratings yet
- Nursing Care Planreadiness of Enhanced Therapeutic Management CompressDocument2 pagesNursing Care Planreadiness of Enhanced Therapeutic Management CompressMarlo Dañez NorbeNo ratings yet
- Oral and Parenteral Medications 1Document61 pagesOral and Parenteral Medications 1Marlo Dañez NorbeNo ratings yet
- BSN III Research Titles 2nd Sem 2021 2022Document5 pagesBSN III Research Titles 2nd Sem 2021 2022Marlo Dañez NorbeNo ratings yet
- DAPIT HAPON: Aging Like A SunDocument2 pagesDAPIT HAPON: Aging Like A SunMarlo Dañez NorbeNo ratings yet
- Assessment Diagnosis Planning Interventions Rationale Evaluation Subjective Data: Short Term Independent: Short TermDocument14 pagesAssessment Diagnosis Planning Interventions Rationale Evaluation Subjective Data: Short Term Independent: Short TermMarlo Dañez NorbeNo ratings yet
- Peda Act 5Document1 pagePeda Act 5Marlo Dañez NorbeNo ratings yet
- Norbe GastroDocument23 pagesNorbe GastroMarlo Dañez NorbeNo ratings yet
- 1st EVALUATION OF HIGH RISK OF PREGNANCYDocument2 pages1st EVALUATION OF HIGH RISK OF PREGNANCYMarlo Dañez NorbeNo ratings yet
- Drug StudyDocument5 pagesDrug StudyMarlo Dañez NorbeNo ratings yet
- Common Laboratory Apparatus: CHM01aLDocument17 pagesCommon Laboratory Apparatus: CHM01aLMarlo Dañez NorbeNo ratings yet
- NI Lab MidTerm Act 3Document2 pagesNI Lab MidTerm Act 3Marlo Dañez NorbeNo ratings yet
- Alkanes: Name: Mauren D. Norbe November 10, 2021 Year/Course: Bscpe 1-Ge Assignment in ChemlecDocument3 pagesAlkanes: Name: Mauren D. Norbe November 10, 2021 Year/Course: Bscpe 1-Ge Assignment in ChemlecMarlo Dañez NorbeNo ratings yet
- Marlo D. Norbe BSN 3 A Nursing Informatics Lab Quiz#2Document2 pagesMarlo D. Norbe BSN 3 A Nursing Informatics Lab Quiz#2Marlo Dañez NorbeNo ratings yet
- Latent Heat of Vaporization: CHM01aL - Chemistry For Engineers - Laboratory Experiment No. 6Document5 pagesLatent Heat of Vaporization: CHM01aL - Chemistry For Engineers - Laboratory Experiment No. 6Marlo Dañez NorbeNo ratings yet
- Marlo D. Norbe BSN3A - GRP 3 Surgery 1 LabDocument5 pagesMarlo D. Norbe BSN3A - GRP 3 Surgery 1 LabMarlo Dañez NorbeNo ratings yet
- Norbe Bsn3a grp3 QUIZDocument3 pagesNorbe Bsn3a grp3 QUIZMarlo Dañez NorbeNo ratings yet
- Web ApplicationDocument3 pagesWeb ApplicationMarlo Dañez NorbeNo ratings yet
- Norbe COMFORT MEASURESDocument10 pagesNorbe COMFORT MEASURESMarlo Dañez NorbeNo ratings yet
- Norbe - Activity 1 Ob 2ND SemDocument4 pagesNorbe - Activity 1 Ob 2ND SemMarlo Dañez NorbeNo ratings yet
- CASEANA Week1Document2 pagesCASEANA Week1Marlo Dañez NorbeNo ratings yet
- Group 10: Script For Activity 5Document2 pagesGroup 10: Script For Activity 5Marlo Dañez NorbeNo ratings yet
- Nursing InformaticsDocument4 pagesNursing Informaticsjulesubayubay5428100% (2)
- Bantuan Hidup DasarDocument77 pagesBantuan Hidup DasarKLINIK KIRANA MEDIKANo ratings yet
- Babylog 8000plusDocument126 pagesBabylog 8000plusMohamed AbdulaalNo ratings yet
- Basic Life Support BlsDocument34 pagesBasic Life Support Blsariel larutaNo ratings yet
- HRCT Thorax Protocol Vs Low Dose CTDocument21 pagesHRCT Thorax Protocol Vs Low Dose CTchristianhasudungan319No ratings yet
- Risk For Aspiration Related To Esophageal Compromise Affecting The Lower Esophageal Sphincter As Evidenced by Heart Burn.Document2 pagesRisk For Aspiration Related To Esophageal Compromise Affecting The Lower Esophageal Sphincter As Evidenced by Heart Burn.eleinsamNo ratings yet
- Documento PDFDocument17 pagesDocumento PDFJose Miguel CastellonNo ratings yet
- Format Rekapitulasi Keluar Masuk Barang LogistikDocument350 pagesFormat Rekapitulasi Keluar Masuk Barang LogistikMV ANUBISNo ratings yet
- Pulmonary Aneurysms Arteriovenous and FistulasDocument9 pagesPulmonary Aneurysms Arteriovenous and FistulasAlvaro OlateNo ratings yet
- Emergency Airway ManagementDocument13 pagesEmergency Airway Managementelyza whidyantiNo ratings yet
- Pranayama: Yoga Assignment - 1 Tarun Saini Bftech, Sem-7Document13 pagesPranayama: Yoga Assignment - 1 Tarun Saini Bftech, Sem-7TARUN SAININo ratings yet
- Principles and Practice of Mechanic (Document1,466 pagesPrinciples and Practice of Mechanic (vvNo ratings yet
- Itinerary LC4WXEDocument3 pagesItinerary LC4WXECzaraine DyNo ratings yet
- ISTpure MSDS VISSPEC 150 enDocument3 pagesISTpure MSDS VISSPEC 150 enHamid KharazmiNo ratings yet
- Reflection Writing For LogbookDocument4 pagesReflection Writing For Logbookkio josephNo ratings yet
- NEWS2 Chart 3 - NEWS Observation Chart - 0Document1 pageNEWS2 Chart 3 - NEWS Observation Chart - 0Diego PerezNo ratings yet
- 108 LTV 950 BrochureDocument2 pages108 LTV 950 BrochurealhassnyNo ratings yet
- MTV 1000 Transport Icu VentilatorDocument4 pagesMTV 1000 Transport Icu Ventilatorhafezasad100% (1)
- Bronchoscopes (Rigid) : Standard Specification ForDocument3 pagesBronchoscopes (Rigid) : Standard Specification ForElif SarıoğluNo ratings yet
- Case-Scenario Respiratoty Disease During Pregnancy NCPDocument4 pagesCase-Scenario Respiratoty Disease During Pregnancy NCPChristianne CapuaNo ratings yet
- Starling ForcesDocument1 pageStarling ForcesbernieNo ratings yet
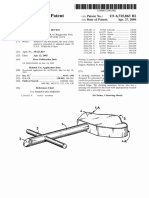
- US Patent No. 6,725,863 B2 To Louis M. Karpel For A "Choking Assistance Device" Later Marketed As The "Heimlich Helper" (4/27/04)Document7 pagesUS Patent No. 6,725,863 B2 To Louis M. Karpel For A "Choking Assistance Device" Later Marketed As The "Heimlich Helper" (4/27/04)Peter M. HeimlichNo ratings yet
- Ventilation Servo-I Universal: Data SheetDocument16 pagesVentilation Servo-I Universal: Data SheetridercoderNo ratings yet
- ACLS Advanced Cardiac Life Support, Iridia MedicalDocument54 pagesACLS Advanced Cardiac Life Support, Iridia MedicalYu Lin ZhangNo ratings yet
- Respiratory Care and Neuromuscular DiseaseDocument1 pageRespiratory Care and Neuromuscular DiseaseMarcelaNo ratings yet
- The Vascular System - EditedDocument5 pagesThe Vascular System - Editedgilbert michaelNo ratings yet
- Airway ManagementDocument16 pagesAirway ManagementSuganthi ParthibanNo ratings yet
- Log Book Foundation ModuleDocument21 pagesLog Book Foundation Modulemaryam zafar100% (2)
- MSDS DupontDocument8 pagesMSDS DupontEMPATI LUWU TIMURNo ratings yet