You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Hand Hygiene Knowledge Assessment Questionnaire (IHI)Document2 pagesHand Hygiene Knowledge Assessment Questionnaire (IHI)Suseno Aji50% (2)
- Belles Palsy Case Study Group 1Document36 pagesBelles Palsy Case Study Group 1JOEY MEAD ARUGAY100% (1)
- Stress - The Different Kinds of StressDocument4 pagesStress - The Different Kinds of StressbogdanNo ratings yet
- Breast Cancer Case StudyDocument48 pagesBreast Cancer Case StudyJay Jay100% (3)
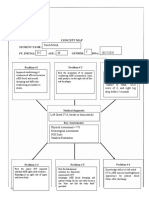
- Careplan - Concept Map DCDocument8 pagesCareplan - Concept Map DCTara McNeillNo ratings yet
- Tara's CH. 64 Arthritis and Connective Tissue DisordersDocument34 pagesTara's CH. 64 Arthritis and Connective Tissue DisordersTara McNeillNo ratings yet
- Tara's CH 63 Musculoskeletal ProblemsDocument23 pagesTara's CH 63 Musculoskeletal ProblemsTara McNeillNo ratings yet
- Urden Chapter - 018 Cardio Diagnostic ProceduresDocument29 pagesUrden Chapter - 018 Cardio Diagnostic ProceduresTara McNeillNo ratings yet
- Urden, Stacy, Lough: Critical Care Nursing, 6 Edition: Chapter 19: Cardiovascular Disorders Test Bank Multiple ChoiceDocument13 pagesUrden, Stacy, Lough: Critical Care Nursing, 6 Edition: Chapter 19: Cardiovascular Disorders Test Bank Multiple ChoiceTara McNeillNo ratings yet
- Case Study 1 - Head InjuryDocument9 pagesCase Study 1 - Head InjuryTara McNeillNo ratings yet
- Tara's Intro To Critical CareDocument6 pagesTara's Intro To Critical CareTara McNeillNo ratings yet
- Careplan - Concept Map DCDocument8 pagesCareplan - Concept Map DCTara McNeillNo ratings yet
- Case Study 1 - Head InjuryDocument9 pagesCase Study 1 - Head InjuryTara McNeillNo ratings yet
- Tara's Anatomy and Physiology - Aehlert ECGs Made EasyDocument16 pagesTara's Anatomy and Physiology - Aehlert ECGs Made EasyTara McNeillNo ratings yet
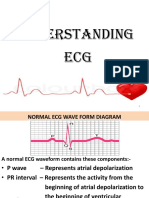
- Understanding ECG Waveforms and Analyzing RhythmsDocument37 pagesUnderstanding ECG Waveforms and Analyzing RhythmsTara McNeillNo ratings yet
- ECG Fast and Easy PPDocument38 pagesECG Fast and Easy PPTara McNeillNo ratings yet
- Urden Chapter - 018 Cardio Diagnostic ProceduresDocument29 pagesUrden Chapter - 018 Cardio Diagnostic ProceduresTara McNeillNo ratings yet
- Urden Chapter - 017 Cardio AssessmentDocument6 pagesUrden Chapter - 017 Cardio AssessmentTara McNeill100% (1)
- Atsp Book 2011Document24 pagesAtsp Book 2011Chengyuan ZhangNo ratings yet
- NCM 116 - GIT (MODULE 5 Part II)Document6 pagesNCM 116 - GIT (MODULE 5 Part II)Meryville JacildoNo ratings yet
- Tutorial 1 1. General Learning ObjectiveDocument2 pagesTutorial 1 1. General Learning ObjectiveMartha Marthad.karifoNo ratings yet
- Malignant Otitis Externa in Patients With Diabetes Mellitus: Case ReportDocument0 pagesMalignant Otitis Externa in Patients With Diabetes Mellitus: Case ReportSuci PramadianiNo ratings yet
- Congenital Ptosis: Evalution and Management DR - Tarakeswara Rao - MsDocument27 pagesCongenital Ptosis: Evalution and Management DR - Tarakeswara Rao - MsVikram Simha NagendlaNo ratings yet
- Understanding Language Disorders in ChildrenDocument3 pagesUnderstanding Language Disorders in Childrenramandeep kaurNo ratings yet
- The Goals of Physical Therapy For Low Back Pain - Hospital For Special SurgeryDocument3 pagesThe Goals of Physical Therapy For Low Back Pain - Hospital For Special SurgerywmtxbbNo ratings yet
- 5Document47 pages5Nasti PalilingNo ratings yet
- Fitz Neurology Paces NotesDocument40 pagesFitz Neurology Paces NotesDrShamshad Khan100% (1)
- OpisthorchisDocument17 pagesOpisthorchisIqraAzizNo ratings yet
- Guide to Salivary Gland NeoplasmsDocument28 pagesGuide to Salivary Gland Neoplasmsrameshparajuli14100% (1)
- Bed Side Teaching Whipple'S Procedure: Submitted To-Sarita Nadiya Madam Submitted By-Ms - ManishaDocument8 pagesBed Side Teaching Whipple'S Procedure: Submitted To-Sarita Nadiya Madam Submitted By-Ms - ManishaManisha ShakyaNo ratings yet
- COVID-19 challenges of a resource-limited countryDocument4 pagesCOVID-19 challenges of a resource-limited countryAlton Nathaniel Nadela DagaleaNo ratings yet
- Histiocytic SarcomaDocument8 pagesHistiocytic SarcomadanishNo ratings yet
- Adhd Final Draft EssayDocument5 pagesAdhd Final Draft Essayapi-273449893100% (1)
- Tam 2007Document5 pagesTam 2007Sarly FebrianaNo ratings yet
- Clinical Aspect of MalariaDocument68 pagesClinical Aspect of MalariaselviaNo ratings yet
- Gineco Eu An 2016 NR 3Document60 pagesGineco Eu An 2016 NR 3GîrbovanCristinaNo ratings yet
- Case StudyDocument4 pagesCase StudyMargarita Limon BalunesNo ratings yet
- Our Hormones' Role in HealthDocument2 pagesOur Hormones' Role in HealthChristina Bajar MatibagNo ratings yet
- Drug index for Risperdal, Diumide, Amlodipine, Linagliptin and other medicationsDocument103 pagesDrug index for Risperdal, Diumide, Amlodipine, Linagliptin and other medicationsvalencia222No ratings yet
- CUTANEOUS ALLERGY MECHANISMS AND TESTINGDocument26 pagesCUTANEOUS ALLERGY MECHANISMS AND TESTINGThiti JessadaromNo ratings yet
- Cardiology Pharmacist Guide to Acute Coronary SyndromeDocument38 pagesCardiology Pharmacist Guide to Acute Coronary SyndromeAnonymous100% (1)
- Liposomal Doxorubicin ExtravasationDocument2 pagesLiposomal Doxorubicin ExtravasationjathieNo ratings yet
- Flu Report Current WeekDocument6 pagesFlu Report Current WeekNews10NBCNo ratings yet
- (NEJM, May 2023) - Medication-Related Osteonecrosis of The Jaw (Images in Clinical Medicine)Document1 page(NEJM, May 2023) - Medication-Related Osteonecrosis of The Jaw (Images in Clinical Medicine)NigelyulNo ratings yet