You might also like
- Trauma HandbookDocument321 pagesTrauma HandbookDaniyal AzmatNo ratings yet
- Pressure UlcerDocument126 pagesPressure UlcerSyabie Yassin100% (1)
- Best Practice Guidelines - Wound Management Diabetic Foot UlcersDocument27 pagesBest Practice Guidelines - Wound Management Diabetic Foot UlcersAndrada Catrinoiu100% (1)
- AnkleSprain PCG 27032009Document30 pagesAnkleSprain PCG 27032009Rachel BlackburnNo ratings yet
- Practice Test - Des O'NeillDocument48 pagesPractice Test - Des O'NeillTahir Rizvi97% (31)
- Prevention and Management of Foot Problems in Diabetes: A Summary Guidance For Daily Practice 2015, Based On The IWGDF Guidance DocumentsDocument9 pagesPrevention and Management of Foot Problems in Diabetes: A Summary Guidance For Daily Practice 2015, Based On The IWGDF Guidance DocumentsMatthew PhillipsNo ratings yet
- Best Practice Guidelines Wound Management Diabetic Foot Ulcers PDFDocument27 pagesBest Practice Guidelines Wound Management Diabetic Foot Ulcers PDFLely JuniariNo ratings yet
- English: Second Quarter - Module 3Document17 pagesEnglish: Second Quarter - Module 3NMDNMSSD67% (3)
- Changing Light Bulbs SafelyDocument1 pageChanging Light Bulbs SafelyAshok Suresh100% (4)
- IWGDF Guidelines 2019 PDFDocument194 pagesIWGDF Guidelines 2019 PDFMara100% (2)
- Date & Time Focus Data Action Response D: Into OR, A - Year Old - PerDocument2 pagesDate & Time Focus Data Action Response D: Into OR, A - Year Old - PerMichelle Gliselle Guinto MallareNo ratings yet
- Teen Breathe June2020Document70 pagesTeen Breathe June2020Екатерина Кедрина100% (1)
- Dental EmergenciesDocument41 pagesDental Emergenciesemancipation1506No ratings yet
- Bedside Ultrasound: Level 1 - Second EditionFrom EverandBedside Ultrasound: Level 1 - Second EditionRating: 5 out of 5 stars5/5 (1)
- Example Letter of Medical NecessityDocument4 pagesExample Letter of Medical Necessitystarlette.hara100% (1)
- Meaning and Definition of Management DevelopmentDocument7 pagesMeaning and Definition of Management DevelopmentRiteshTirkey100% (2)
- Contemporary Periodontal Surgery: An Illustrated Guide to the Art behind the ScienceFrom EverandContemporary Periodontal Surgery: An Illustrated Guide to the Art behind the ScienceNo ratings yet
- OsteoarthritisDocument386 pagesOsteoarthritisA Syed ZahidNo ratings yet
- Diabetic FootDocument104 pagesDiabetic FootadibeuutNo ratings yet
- Ureteral CalculiDocument177 pagesUreteral CalculisolcitourraNo ratings yet
- Viêm KH PDocument14 pagesViêm KH PChang ĐỗNo ratings yet
- Npuap Epuap Pppia CPG 2017Document348 pagesNpuap Epuap Pppia CPG 2017RivanFirdausNo ratings yet
- A Clinical Practice Guideline For Physical Therapy in Patients With Hip or Knee OsteoarthritisDocument21 pagesA Clinical Practice Guideline For Physical Therapy in Patients With Hip or Knee OsteoarthritisalonsoNo ratings yet
- ME and Resus Standards Resus Council UKDocument41 pagesME and Resus Standards Resus Council UKklopine1234No ratings yet
- Practical Guidelines On The Prevention and Management of Diabetic Foot IWGDF 2019Document10 pagesPractical Guidelines On The Prevention and Management of Diabetic Foot IWGDF 2019Maya SariNo ratings yet
- Clinical Algorithms To Aid Osteoarthritis Guideline DisseminationDocument13 pagesClinical Algorithms To Aid Osteoarthritis Guideline Disseminationfidatahir93No ratings yet
- 2019 Guidelines Bariatric Surgery EAES SAGESDocument29 pages2019 Guidelines Bariatric Surgery EAES SAGESDra Maha HafezNo ratings yet
- Updated 10-16-14 Quick Reference Guide Digital Npuap Epuap Pppia 16oct2014Document75 pagesUpdated 10-16-14 Quick Reference Guide Digital Npuap Epuap Pppia 16oct2014Anonymous kZQet6QA100% (1)
- Management Recommendations For Knee Osteoarthritis: How Usable Are They?Document8 pagesManagement Recommendations For Knee Osteoarthritis: How Usable Are They?tiwiyunNo ratings yet
- Evidance Table For Traction Management and CareDocument13 pagesEvidance Table For Traction Management and CarehakamNo ratings yet
- Guideline Title: Clinical Practice Guidelines For The Management of Clubfoot Deformity Using The Ponseti MethodDocument31 pagesGuideline Title: Clinical Practice Guidelines For The Management of Clubfoot Deformity Using The Ponseti MethodAna-Maria DuleaNo ratings yet
- Best Practise Recommendations UkDocument16 pagesBest Practise Recommendations UkdrvijeypsgNo ratings yet
- 10 1111@anae 15291Document13 pages10 1111@anae 15291Ili RamosNo ratings yet
- VV Mai03-Parodont ENGDocument19 pagesVV Mai03-Parodont ENGAlyaNo ratings yet
- IWGDF Guidelines 2023Document349 pagesIWGDF Guidelines 2023fabianasaboyaNo ratings yet
- Total Ankle Replacement Surgery (Arthroplasty)Document12 pagesTotal Ankle Replacement Surgery (Arthroplasty)ashut1No ratings yet
- Early Management of Severe Abdominal - 2020 - Anaesthesia Critical Care - Pain MDocument9 pagesEarly Management of Severe Abdominal - 2020 - Anaesthesia Critical Care - Pain MRicardoNo ratings yet
- 1 - Anaesthesia 2012 Guidelines Das - Tracheal ExtubationDocument23 pages1 - Anaesthesia 2012 Guidelines Das - Tracheal ExtubationTelmo Santos100% (2)
- American Society Ostomy SurgeryDocument13 pagesAmerican Society Ostomy SurgeryvictorNo ratings yet
- Arthritis Care Research - 2020 - Kolasinski - 2019 American College of Rheumatology Arthritis Foundation Guideline ForDocument14 pagesArthritis Care Research - 2020 - Kolasinski - 2019 American College of Rheumatology Arthritis Foundation Guideline ForRodrigoNo ratings yet
- Knee Assessement FormDocument2 pagesKnee Assessement FormLee Woo GuanNo ratings yet
- Osteoarthritis Guideline Early View 2019Document14 pagesOsteoarthritis Guideline Early View 2019Tergfdsx DsfdsgdNo ratings yet
- Guidelines for Dentists UKDocument41 pagesGuidelines for Dentists UKRomi Sepúlveda SaldiviaNo ratings yet
- Diabetes Metabolism Res - 2023 - Schaper - Practical Guidelines On The Prevention and Management of Diabetes Related FootDocument14 pagesDiabetes Metabolism Res - 2023 - Schaper - Practical Guidelines On The Prevention and Management of Diabetes Related FootClaudia MNo ratings yet
- Acute Nursing Care of The Older Adult With Fragility Hip Fracture An International Perspective Part 2 PDFDocument15 pagesAcute Nursing Care of The Older Adult With Fragility Hip Fracture An International Perspective Part 2 PDFOktaNo ratings yet
- 2019 American College of Rheumatology/Arthritis Foundation Guideline For The Management of Osteoarthritis of The Hand, Hip, and KneeDocument14 pages2019 American College of Rheumatology/Arthritis Foundation Guideline For The Management of Osteoarthritis of The Hand, Hip, and KneeHellmann Adrian Escobar CNo ratings yet
- Diabetes Metabolism Res - 2023 - SchaperDocument14 pagesDiabetes Metabolism Res - 2023 - SchaperUsman AliNo ratings yet
- Resusgl 2010Document157 pagesResusgl 2010Salman IslamNo ratings yet
- Barreras Facilitadores Implementacion LabioDocument9 pagesBarreras Facilitadores Implementacion LabioOpeNo ratings yet
- Osteoarthritis Guideline Early View 2019Document14 pagesOsteoarthritis Guideline Early View 2019Gaby CastilloNo ratings yet
- Metatarsophalangeal Joint Replacement of The Hallux PDF 1899863212945093Document6 pagesMetatarsophalangeal Joint Replacement of The Hallux PDF 1899863212945093JanetNo ratings yet
- CPR Guideline PDFDocument157 pagesCPR Guideline PDFPandu AnggoroNo ratings yet
- Consensus Statement For Perioperative Care in Total Hip Replacement and Total Knee Replacement Surgery: Enhanced Recovery After Surgery (ERAS®) Society RecommendationsDocument18 pagesConsensus Statement For Perioperative Care in Total Hip Replacement and Total Knee Replacement Surgery: Enhanced Recovery After Surgery (ERAS®) Society RecommendationsJuliana Moreno LadinoNo ratings yet
- Dif Ficult Airway Society 2015 Guidelines For Management of Unanticipated Dif Ficult Intubation in AdultsDocument22 pagesDif Ficult Airway Society 2015 Guidelines For Management of Unanticipated Dif Ficult Intubation in AdultsAnaMariaBustamanteNo ratings yet
- Michael ZonoDocument4 pagesMichael Zonochetna yogeshNo ratings yet
- Guia 14279 230705 081935Document25 pagesGuia 14279 230705 081935Marce SiuNo ratings yet
- BEST EVIDENCE: HEALTH EDUCATION FOOT AND SKIN CAREDocument17 pagesBEST EVIDENCE: HEALTH EDUCATION FOOT AND SKIN CARETeanu Jose Gabrillo TamayoNo ratings yet
- Experts Advise Against Arthroscopy For Almost All Patients With Degenerative Knee Damage - FullDocument9 pagesExperts Advise Against Arthroscopy For Almost All Patients With Degenerative Knee Damage - FullWillbourNo ratings yet
- GUIDELINE Inguinal Hernia Repair Toward Asian GuidelinesDocument8 pagesGUIDELINE Inguinal Hernia Repair Toward Asian GuidelinesHendry Susanto100% (1)
- BMC Musculoskeletal DisordersDocument5 pagesBMC Musculoskeletal DisordersBogdan TudorNo ratings yet
- Ulcer PDFDocument317 pagesUlcer PDFRadu Roxana ElenaNo ratings yet
- Anastesi GuidelineDocument8 pagesAnastesi GuidelineDeboraNainggolanNo ratings yet
- Acute Nursing Care of The Older Adult With Fragility Hip Fracture: An International Perspective (Part 2)Document26 pagesAcute Nursing Care of The Older Adult With Fragility Hip Fracture: An International Perspective (Part 2)spring flowerNo ratings yet
- Pressure Ulcer PreventionDocument8 pagesPressure Ulcer PreventionMsPocketbook HoarderNo ratings yet
- The Surgery-First Orthognathic Approach: With discussion of occlusal plane-altering orthognathic surgeryFrom EverandThe Surgery-First Orthognathic Approach: With discussion of occlusal plane-altering orthognathic surgeryNo ratings yet
- FASJ - 2017 - Valisena - TX of Mortons Neuroma - Systematic ReviewDocument11 pagesFASJ - 2017 - Valisena - TX of Mortons Neuroma - Systematic ReviewJacob DoughertyNo ratings yet
- Imaging of Lesser Metatarsophalangeal JoDocument13 pagesImaging of Lesser Metatarsophalangeal JoneilNo ratings yet
- Design and Analysis of Pilot Studies: Recommendations For Good PracticeDocument6 pagesDesign and Analysis of Pilot Studies: Recommendations For Good PracticeneilNo ratings yet
- The Journal of Foot & Ankle SurgeryDocument5 pagesThe Journal of Foot & Ankle SurgeryneilNo ratings yet
- 1 s2.0 S1008127515000127 MainDocument3 pages1 s2.0 S1008127515000127 MainneilNo ratings yet
- Accepted Manuscript: The FootDocument27 pagesAccepted Manuscript: The FootneilNo ratings yet
- Clinical GovernanceDocument2 pagesClinical GovernanceneilNo ratings yet
- Lee 2017Document10 pagesLee 2017Nasser JaliNo ratings yet
- The Foot: Dalton Ryba, Nooreen Ibrahim, Jim Choi, Vassilios VardaxisDocument6 pagesThe Foot: Dalton Ryba, Nooreen Ibrahim, Jim Choi, Vassilios VardaxisneilNo ratings yet
- Dartfish Terms of UseDocument17 pagesDartfish Terms of UseneilNo ratings yet
- Comparison of Convenience Sampling and Purposive S PDFDocument5 pagesComparison of Convenience Sampling and Purposive S PDFnakul.heble6385No ratings yet
- Selection Criteria For Patients With Chronic Ankle Instability in Controlled Research: A Position Statement of The International Ankle ConsortiumDocument7 pagesSelection Criteria For Patients With Chronic Ankle Instability in Controlled Research: A Position Statement of The International Ankle ConsortiumJohann Sebastian CruzNo ratings yet
- Plantar Plate Tear in HurdlerDocument5 pagesPlantar Plate Tear in HurdlerneilNo ratings yet
- Custom Orthotics PDFDocument14 pagesCustom Orthotics PDFneilNo ratings yet
- Health Promotion On Nutrition For Children Under FiveDocument21 pagesHealth Promotion On Nutrition For Children Under FiveSinta WuLandariNo ratings yet
- 21 - Piriformis SyndromeDocument11 pages21 - Piriformis SyndromewatiNo ratings yet
- Removable Partial Denture Occlusion: John R. Ivanhoe, DDS, Kevin D. Plummer, DDSDocument17 pagesRemovable Partial Denture Occlusion: John R. Ivanhoe, DDS, Kevin D. Plummer, DDSAna MaríaNo ratings yet
- CS14396 XimenaParra Advanced Management of WHS A2 MyapchubDocument6 pagesCS14396 XimenaParra Advanced Management of WHS A2 MyapchubXimena ParraNo ratings yet
- Ik Gujral Punjab Technical University Jalandhar, Kapurthala: Sess Sem Sub Code Sub Title Course/BranchDocument178 pagesIk Gujral Punjab Technical University Jalandhar, Kapurthala: Sess Sem Sub Code Sub Title Course/BranchMohit KaundalNo ratings yet
- MSDS DDDocument2 pagesMSDS DDBaher SaidNo ratings yet
- Tutorial 1A - Public HealthDocument22 pagesTutorial 1A - Public Healthmuhammad saufi sulaimanNo ratings yet
- Board and Reviewer Assignments for Convened IRB ReviewDocument5 pagesBoard and Reviewer Assignments for Convened IRB ReviewMuhammad Zaryab KhanNo ratings yet
- BT-740 OP Manual (740-ENG-OPM-EUR-R02) PDFDocument50 pagesBT-740 OP Manual (740-ENG-OPM-EUR-R02) PDFJaneth Pariona SedanNo ratings yet
- Time Out: GrammarDocument8 pagesTime Out: GrammarNguyễnVũHoàngTấnNo ratings yet
- Nursing Health AssessmentDocument19 pagesNursing Health AssessmentAHMAD HASIMI BIN ABDUL GHANI STUDENTNo ratings yet
- English Assignment Direct and Indirect SentencesDocument6 pagesEnglish Assignment Direct and Indirect SentencesSasmita Novalis ArrizqiNo ratings yet
- AL CIERRE DE Julio Del 2021: Barra COD AlfabetaDocument2 pagesAL CIERRE DE Julio Del 2021: Barra COD AlfabetaBrian Javier GomezNo ratings yet
- Artigo - Thought Disorder Schizophrenia - EnglishDocument11 pagesArtigo - Thought Disorder Schizophrenia - EnglishFrancisco ReigNo ratings yet
- قواعد التوثيق في البحوث والدراسات التربويةDocument19 pagesقواعد التوثيق في البحوث والدراسات التربويةnemra1No ratings yet
- The Application of CAD CAM Technology in DentistryDocument13 pagesThe Application of CAD CAM Technology in DentistryMihaela Vasiliu0% (1)
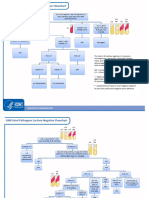
- GNR Stool Pathogens Lactose Negative FlowchartDocument2 pagesGNR Stool Pathogens Lactose Negative FlowchartKeithNo ratings yet
- Ebook Conflict and Communication 1St Edition Jandt Test Bank Full Chapter PDFDocument27 pagesEbook Conflict and Communication 1St Edition Jandt Test Bank Full Chapter PDFgladysvanx3z100% (9)
- Thesis Statement For Nickel and DimedDocument8 pagesThesis Statement For Nickel and Dimedafkntwbla100% (2)
- Curriculam Vitae: ObjectiveDocument5 pagesCurriculam Vitae: ObjectiveGokul RajNo ratings yet
- Seligman Attributional Style QuestionnaireDocument14 pagesSeligman Attributional Style QuestionnaireAnjali VyasNo ratings yet
- Employees' Financial Literacy, Behavior, Stress and WellnessDocument12 pagesEmployees' Financial Literacy, Behavior, Stress and WellnessYong Leigh LocusamNo ratings yet
- Chapter Two-Foundation of Individual Behavior and Learning in An OrganizationDocument16 pagesChapter Two-Foundation of Individual Behavior and Learning in An OrganizationMikias DegwaleNo ratings yet
- Time Magazine USA - December 22 2023Document98 pagesTime Magazine USA - December 22 2023paccs2006No ratings yet