You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The Most Common Cause of Lower Gastrointestinal BleedingDocument2 pagesThe Most Common Cause of Lower Gastrointestinal BleedingFanny PritaningrumNo ratings yet
- Rectal Bleeding and PolypsDocument4 pagesRectal Bleeding and PolypsFanny PritaningrumNo ratings yet
- Sonographic Features of A Juvenile Polyp - A Case Report andDocument3 pagesSonographic Features of A Juvenile Polyp - A Case Report andFanny PritaningrumNo ratings yet
- Liver Invovlement - SLEDocument7 pagesLiver Invovlement - SLEFanny PritaningrumNo ratings yet
- Clinical Assessment and Treatment Algorithm For LowerDocument7 pagesClinical Assessment and Treatment Algorithm For LowerFanny PritaningrumNo ratings yet
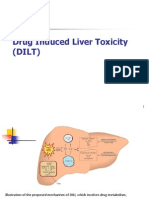
- MOlekulaer Patfis DILIDocument14 pagesMOlekulaer Patfis DILIFanny PritaningrumNo ratings yet
- Severe Ulcerative Colitis UHL Childrens Medical GuidelineDocument8 pagesSevere Ulcerative Colitis UHL Childrens Medical GuidelineFanny PritaningrumNo ratings yet
- Electronic Physician (ISSN: 2008-5842)Document5 pagesElectronic Physician (ISSN: 2008-5842)Aldian DianNo ratings yet
- Liver Complications - SLEDocument5 pagesLiver Complications - SLEFanny PritaningrumNo ratings yet
- Complications of ColonosDocument19 pagesComplications of ColonosFanny PritaningrumNo ratings yet
- Toxicology FinalDocument14 pagesToxicology FinalAyuNo ratings yet
- Classification of Drug Hypersensitivity Into Allergic, P-I, and Pseudo-Allergic FormsDocument14 pagesClassification of Drug Hypersensitivity Into Allergic, P-I, and Pseudo-Allergic FormsFanny PritaningrumNo ratings yet
- AIH - SLE DifferentiateDocument8 pagesAIH - SLE DifferentiateFanny PritaningrumNo ratings yet
- AIH - SLE How To DXDocument3 pagesAIH - SLE How To DXFanny PritaningrumNo ratings yet
- Hepatitis in A Patient With SLE: Is It Autoimmune Hepatitis?Document5 pagesHepatitis in A Patient With SLE: Is It Autoimmune Hepatitis?Fanny PritaningrumNo ratings yet
- Flare in SleDocument9 pagesFlare in SleFanny PritaningrumNo ratings yet
- DILI - Karakterisitik Klinik Dan FRDocument11 pagesDILI - Karakterisitik Klinik Dan FRFanny PritaningrumNo ratings yet
- Immunological ConsiderationDocument18 pagesImmunological ConsiderationFanny PritaningrumNo ratings yet
- HIV-AIDS Related RespiratoryDocument159 pagesHIV-AIDS Related RespiratoryFanny PritaningrumNo ratings yet
- Pulmonary Immune Function in HivDocument16 pagesPulmonary Immune Function in HivFanny PritaningrumNo ratings yet
- En - Practical Approach.2010Document13 pagesEn - Practical Approach.2010rendyjiwonoNo ratings yet
- Role of Innate and Adaptive Immunity During Drug-Induced Liver InjuryDocument10 pagesRole of Innate and Adaptive Immunity During Drug-Induced Liver InjuryFanny PritaningrumNo ratings yet
- pGALS Examination OSCE GuideDocument18 pagespGALS Examination OSCE GuideFanny PritaningrumNo ratings yet
- Lung Is A Major Target Organ For HIV InfectionDocument12 pagesLung Is A Major Target Organ For HIV InfectionFanny PritaningrumNo ratings yet
- Fluid Management in Neonates and InfantsDocument14 pagesFluid Management in Neonates and InfantsJosselle Sempio CalientaNo ratings yet
- CHD in DSDocument2 pagesCHD in DSFanny PritaningrumNo ratings yet
- WHO Interim Guidance On The Use of Mask - 29 January 2020Document2 pagesWHO Interim Guidance On The Use of Mask - 29 January 2020VERA FilesNo ratings yet
- Can Procalcitonin Monitoring Reduce The Length of AntibioticDocument3 pagesCan Procalcitonin Monitoring Reduce The Length of AntibioticFanny PritaningrumNo ratings yet
- Specialized Settings: Section ViiiDocument8 pagesSpecialized Settings: Section ViiiFanny PritaningrumNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Side Effects of Drugs - Annual 33 - J. Aronson (Elsevier, 2011) WWDocument1,122 pagesSide Effects of Drugs - Annual 33 - J. Aronson (Elsevier, 2011) WWAndrei E. HawayNo ratings yet
- Liver Function Tests GuideDocument38 pagesLiver Function Tests GuideshehnilaNo ratings yet
- Clinical Pharmacokinetics in Liver Failure Patients SenddDocument30 pagesClinical Pharmacokinetics in Liver Failure Patients Senddthavia andrianiNo ratings yet
- LIVER DISEASES LECTUREDocument89 pagesLIVER DISEASES LECTURERinkiNo ratings yet
- Drug Induced Liver DisordersDocument31 pagesDrug Induced Liver DisordersJason fernandes jNo ratings yet
- 10 4292@wjgpt v8 I1 26Document14 pages10 4292@wjgpt v8 I1 26Syawal PratamaNo ratings yet
- Therapeutic Roles of Medicinal Herbs For The Treatment of Jaundice and Hepatitis BDocument7 pagesTherapeutic Roles of Medicinal Herbs For The Treatment of Jaundice and Hepatitis BEditor IJTSRDNo ratings yet
- Drug Induced Liver Toxicity (DILD)Document39 pagesDrug Induced Liver Toxicity (DILD)Surya Pratama100% (1)
- Drug-Induced Hepatotoxicity - Overview, Metabolism of Drugs, Clinical and Pathological Manifestations of Drug-Induced Liver DiseaseDocument20 pagesDrug-Induced Hepatotoxicity - Overview, Metabolism of Drugs, Clinical and Pathological Manifestations of Drug-Induced Liver Diseaseal ghiffari muhammad rayhan100% (1)
- Acute Liver Failure in Adults: Etiology, Clinical Manifestations, and Diagnosis - UpToDateDocument14 pagesAcute Liver Failure in Adults: Etiology, Clinical Manifestations, and Diagnosis - UpToDateIatros GarciniNo ratings yet
- Att Reintroduction Nhs FlowchartDocument6 pagesAtt Reintroduction Nhs FlowchartNitesh Gupta100% (1)
- Institute For Safe Medication Practices 2011 ReportDocument25 pagesInstitute For Safe Medication Practices 2011 ReportLaw Med BlogNo ratings yet
- Drug-induced Liver Disease (DILD) Causes, Types, DiagnosisDocument30 pagesDrug-induced Liver Disease (DILD) Causes, Types, DiagnosisSurya PratamaNo ratings yet
- Drug Use in Special Conditions - CLD and CKDDocument93 pagesDrug Use in Special Conditions - CLD and CKDadamu mohammadNo ratings yet
- Philips CA Et Al 2019Document15 pagesPhilips CA Et Al 2019Aditya PaiNo ratings yet
- CC - Liver FunctionDocument5 pagesCC - Liver FunctionOrhan AsdfghjklNo ratings yet
- Pass Critical Care Liver GITDocument49 pagesPass Critical Care Liver GITyorghiLNo ratings yet
- Cuscuta Chinensislam. - A Systematic Review On PDFDocument17 pagesCuscuta Chinensislam. - A Systematic Review On PDFDintakurthi PrasanthNo ratings yet
- Antituberculous Therapy in Special SituationsDocument8 pagesAntituberculous Therapy in Special SituationsMobeen Raza100% (1)
- Cordia MyxaDocument12 pagesCordia MyxaZubair Akram JanjuaNo ratings yet
- PCM PoisonDocument23 pagesPCM PoisonPrabhat KcNo ratings yet
- GARCININADocument9 pagesGARCININAGabriela CuevasNo ratings yet
- Date Pit Review PaperDocument34 pagesDate Pit Review PaperDr-Aftab Ahmed KhanNo ratings yet
- Herbalife Hepatotoxicity Report - HERBLIFE or POTENTIAL STRIFEDocument5 pagesHerbalife Hepatotoxicity Report - HERBLIFE or POTENTIAL STRIFEMohammed AyubNo ratings yet
- DILI Diagnosis & ManagementDocument25 pagesDILI Diagnosis & ManagementSenarathKuleeshaKodisingheNo ratings yet
- Herbal Hepatotoxicity: Suspected Cases Assessed For Alternative CausesDocument6 pagesHerbal Hepatotoxicity: Suspected Cases Assessed For Alternative CausesNariNo ratings yet
- 899 PDFDocument3 pages899 PDFManuel CarboNo ratings yet
- Promoting Restful Sleep in Pediatric PatientDocument4 pagesPromoting Restful Sleep in Pediatric PatientDennis Nyambane MomanyiNo ratings yet
- 3 Review of Literature (13 37) of Hemidesmus IndicusDocument26 pages3 Review of Literature (13 37) of Hemidesmus Indicusmithun_nm100% (1)
- A Critical Review of Phaltrikadi Kwath WSR To Liver DisordersDocument6 pagesA Critical Review of Phaltrikadi Kwath WSR To Liver DisordersAditaya Nath TewariNo ratings yet