You might also like
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 2019 Fall Expo Contact List PDFDocument10 pages2019 Fall Expo Contact List PDFSoji AdimulaNo ratings yet
- Chronic Wound Managment HMIDocument37 pagesChronic Wound Managment HMIannisa edwarNo ratings yet
- Hospital Bill FormatDocument2 pagesHospital Bill Formatsandee1910100% (2)
- University Physics Volume 2 Derived Copy For Ysc1213 1.75Document441 pagesUniversity Physics Volume 2 Derived Copy For Ysc1213 1.75Soji AdimulaNo ratings yet
- Starcke. The History of Articulators - The Appearance and Early History of Facebow. (2000)Document5 pagesStarcke. The History of Articulators - The Appearance and Early History of Facebow. (2000)Jose Enrique AvilaNo ratings yet
- LLLLFTL Ttllaosu RP, Ry: !rll1blllnts Allows Rehabilitation of Function andDocument179 pagesLLLLFTL Ttllaosu RP, Ry: !rll1blllnts Allows Rehabilitation of Function andTsvetelin KaloianovNo ratings yet
- Gauss Law ReviewDocument61 pagesGauss Law ReviewSoji AdimulaNo ratings yet
- Chapter 11Document12 pagesChapter 11Soji AdimulaNo ratings yet
- DiagramsDocument62 pagesDiagramsSoji AdimulaNo ratings yet
- Tree Care Industry MagazineDocument44 pagesTree Care Industry MagazineSoji AdimulaNo ratings yet
- Son of South Korean Immigrants, Bucks County's Andrew Heo Carries Family's Olympic Dream To BeijingDocument8 pagesSon of South Korean Immigrants, Bucks County's Andrew Heo Carries Family's Olympic Dream To BeijingSoji AdimulaNo ratings yet
- Sun Hasn't Set On Sunrise Packaging - Minneapolis - St. Paul Business JournalDocument4 pagesSun Hasn't Set On Sunrise Packaging - Minneapolis - St. Paul Business JournalSoji AdimulaNo ratings yet
- Chem 14CL - Lecture 1 - Amino - AcidDocument17 pagesChem 14CL - Lecture 1 - Amino - AcidSoji AdimulaNo ratings yet
- Molecular Orbitals and Curved ArrowsDocument51 pagesMolecular Orbitals and Curved ArrowsSoji AdimulaNo ratings yet
- Periodic Properties of The Elements: Theodore L. Brown H. Eugene Lemay, Jr. and Bruce E. BurstenDocument82 pagesPeriodic Properties of The Elements: Theodore L. Brown H. Eugene Lemay, Jr. and Bruce E. BurstenSoji AdimulaNo ratings yet
- Bio-Med 350: Normal Heart Function and Congestive Heart FailureDocument59 pagesBio-Med 350: Normal Heart Function and Congestive Heart FailureSoji AdimulaNo ratings yet
- Faculty Version With Model Answers: Body FluidsDocument10 pagesFaculty Version With Model Answers: Body FluidsSoji AdimulaNo ratings yet
- Inflammation and Repair: Definition of Inflammation Acute Inflammation Vascular Events in InflammationDocument35 pagesInflammation and Repair: Definition of Inflammation Acute Inflammation Vascular Events in InflammationSoji AdimulaNo ratings yet
- RC Circuits: Instructor: Kazumi TolichDocument11 pagesRC Circuits: Instructor: Kazumi TolichSoji AdimulaNo ratings yet
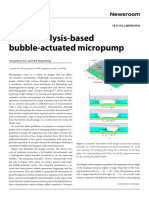
- An Electrolysis-Based Bubble-Actuated Micropump: Cheng-Hsien Liu and Chih Ming ChengDocument3 pagesAn Electrolysis-Based Bubble-Actuated Micropump: Cheng-Hsien Liu and Chih Ming ChengSoji AdimulaNo ratings yet
- Happy Labor Day: Tuesday, September 8, 2020Document1 pageHappy Labor Day: Tuesday, September 8, 2020Soji AdimulaNo ratings yet
- What Is An Argument?: ConclusionDocument25 pagesWhat Is An Argument?: ConclusionSoji AdimulaNo ratings yet
- Brian Sellick y Maniobra de SellickDocument3 pagesBrian Sellick y Maniobra de SellickUther PendragonNo ratings yet
- Tindakan MinorDocument2 pagesTindakan MinorBisturi 2022No ratings yet
- Kirstensen 2014 Esc - Esa Guidelines On Non Cardiac SurgeryDocument49 pagesKirstensen 2014 Esc - Esa Guidelines On Non Cardiac SurgeryCorina DiaconescuNo ratings yet
- Vacancies in The Department of Health: DirectorateDocument3 pagesVacancies in The Department of Health: DirectorategxjjsjejduNo ratings yet
- MAHESH S DHA Anesthesia TechnologyDocument4 pagesMAHESH S DHA Anesthesia TechnologyGloria JaisonNo ratings yet
- Orthospace BrochureDocument2 pagesOrthospace BrochureJuan Martinez Del AngelNo ratings yet
- Hernia - Femoral Hernia, Epigastric Hernia, Paraumbilical Hernia, Incisional HerniaDocument29 pagesHernia - Femoral Hernia, Epigastric Hernia, Paraumbilical Hernia, Incisional HerniaKuruNo ratings yet
- Hospital and Medical Care Planning CH 1Document31 pagesHospital and Medical Care Planning CH 1baburamNo ratings yet
- ReviewerDocument10 pagesReviewerCharlene RepolloNo ratings yet
- Package List Swasthysathi 2018-Grade BDocument150 pagesPackage List Swasthysathi 2018-Grade BKuntal GuptaNo ratings yet
- Subject: Walk-In-Interview For The Post of Senior ResidentDocument8 pagesSubject: Walk-In-Interview For The Post of Senior ResidentGUNDEBOINA NarasimhaNo ratings yet
- Book Review: Skull FractureDocument2 pagesBook Review: Skull FractureMohammad AkheelNo ratings yet
- Strategies in Liver TraumaDocument9 pagesStrategies in Liver TraumaLuis Miguel Díaz VegaNo ratings yet
- Jurnal Reading Anestesi M. Fikri Ridha1102015122Document6 pagesJurnal Reading Anestesi M. Fikri Ridha1102015122Hielmy Auliya HasyimNo ratings yet
- Evaluation of Cement-Retained Versus Screw-Retained Implant-Supported Restorations For Marginal Bone Loss A Systematic Review and Meta-AnalysisDocument9 pagesEvaluation of Cement-Retained Versus Screw-Retained Implant-Supported Restorations For Marginal Bone Loss A Systematic Review and Meta-AnalysisJuan Andres EspinozaNo ratings yet
- Statistics: Aesthetic Plastic Surgery National DatabankDocument26 pagesStatistics: Aesthetic Plastic Surgery National DatabankNuka AtabegashviliNo ratings yet
- Basik Lasik - Tips On Lasik Eye SurgeryDocument4 pagesBasik Lasik - Tips On Lasik Eye Surgeryenglish-exactly100% (1)
- Brochure JD Guided Surgery KitDocument6 pagesBrochure JD Guided Surgery KitTeaca DumitruNo ratings yet
- Chymoral Plus'Document3 pagesChymoral Plus'Neha SureshNo ratings yet
- PH Orthooutcomesreport 0904 Final SampleDocument15 pagesPH Orthooutcomesreport 0904 Final Sampleapi-550152465No ratings yet
- ATS Surgical Table PDFDocument3 pagesATS Surgical Table PDFErnesto RiquelmeNo ratings yet
- Medanta VisitDocument3 pagesMedanta VisitArpita HalderNo ratings yet
- Newsletter ISAPS Sept Dec 2012 PDFDocument21 pagesNewsletter ISAPS Sept Dec 2012 PDFhuyenthanh1807No ratings yet
- Condylar SagDocument8 pagesCondylar Sagshreya dasNo ratings yet
- An Impressive Personality Of: Dato' DR Sheikh Muszaphar ShukorDocument10 pagesAn Impressive Personality Of: Dato' DR Sheikh Muszaphar ShukorFariza AinaNo ratings yet
- Endal Et Al. 2011 (A HRCT Study of Changes Istmus)Document5 pagesEndal Et Al. 2011 (A HRCT Study of Changes Istmus)Adriiana Jaimes JaimesNo ratings yet