You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Igg Candida: Clinical Information For ProfessionalsDocument1 pageIgg Candida: Clinical Information For ProfessionalsDragosAurNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Immune Response To Fungal InfectionsDocument14 pagesThe Immune Response To Fungal Infectionsishihara-deny-3078No ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grundfos Price List CAT 4 Feb 2020Document52 pagesGrundfos Price List CAT 4 Feb 2020DragosAurNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Immunity To Enterotoxin-Producing BacteriaDocument2 pagesImmunity To Enterotoxin-Producing BacteriaDragosAurNo ratings yet
- The Role of Klebsiella in Crohn's Disease With A Potential ForDocument9 pagesThe Role of Klebsiella in Crohn's Disease With A Potential ForDragosAurNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Overlooked Immune State in Candidemia: A Risk Factor For MortalityDocument12 pagesThe Overlooked Immune State in Candidemia: A Risk Factor For MortalityDragosAurNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- FSDigest Aflatoxins EN PDFDocument5 pagesFSDigest Aflatoxins EN PDFBashar SaiidNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Identintificare CandidaDocument5 pagesIdentintificare CandidaDragosAurNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Chronic Diarrhea and MalabsorptionDocument77 pagesChronic Diarrhea and MalabsorptionDragosAurNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Therapeutic Guidelines in Systemic Fungal Infection 3edDocument127 pagesTherapeutic Guidelines in Systemic Fungal Infection 3eddohuutri66No ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Fat MalabsorbtionDocument18 pagesFat MalabsorbtionDragosAurNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Therapeutic Guidelines in Systemic Fungal Infection 3edDocument127 pagesTherapeutic Guidelines in Systemic Fungal Infection 3eddohuutri66No ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Detection and Quantitation of Aflatoxin For The Diagnosis ofDocument4 pagesDetection and Quantitation of Aflatoxin For The Diagnosis ofDragosAurNo ratings yet
- Immunity To Enterotoxin-Producing BacteriaDocument2 pagesImmunity To Enterotoxin-Producing BacteriaDragosAurNo ratings yet
- Table 1 Histories of patients with refractory giardiasisDocument1 pageTable 1 Histories of patients with refractory giardiasisDragosAurNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- 1,3-Beta-D-Glucan (Fungitell), SerumDocument4 pages1,3-Beta-D-Glucan (Fungitell), SerumDragosAurNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- CD4 Lymphocytopenia Without Hiv InfectionDocument6 pagesCD4 Lymphocytopenia Without Hiv InfectionDragosAurNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Treatment-refractory giardiasis challenges and solutionsDocument13 pagesTreatment-refractory giardiasis challenges and solutionsDragosAurNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Candida glabrata Strains Resistant to Fluconazole and ItraconazoleDocument3 pagesCandida glabrata Strains Resistant to Fluconazole and ItraconazoleDragosAurNo ratings yet
- Clinical Evaluation GIDocument2 pagesClinical Evaluation GIDragosAurNo ratings yet
- Dr. Adrian Marinescu Matei Bals Virgil Musta, Medic Primar de Boli InfecțioaseDocument17 pagesDr. Adrian Marinescu Matei Bals Virgil Musta, Medic Primar de Boli InfecțioaseDragosAurNo ratings yet
- 1,3-Beta-D-Glucan (Fungitell), SerumDocument4 pages1,3-Beta-D-Glucan (Fungitell), SerumDragosAurNo ratings yet
- Toxocara Canis: Veterinary and Zoonotic Importance, Diagnosis and ControlDocument29 pagesToxocara Canis: Veterinary and Zoonotic Importance, Diagnosis and ControlDragosAurNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Diaree Cronica Cu EtiologiiDocument7 pagesDiaree Cronica Cu EtiologiiDragosAurNo ratings yet
- Various AnthelminticsDocument1 pageVarious AnthelminticsDragosAurNo ratings yet
- What Causes Gastritis?Document14 pagesWhat Causes Gastritis?DragosAurNo ratings yet
- Fusarium Dimerum.: Fusarium SPP - Grow Rapidly On Sabouraud Dextrose Agar at 25°C and ProduceDocument14 pagesFusarium Dimerum.: Fusarium SPP - Grow Rapidly On Sabouraud Dextrose Agar at 25°C and ProduceDragosAurNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Caiet Modul 2Document249 pagesCaiet Modul 2Lovely Candles100% (3)
- Dumping Diet 5Document3 pagesDumping Diet 5Syafira SalsabilaNo ratings yet
- DLL ObservationDocument5 pagesDLL ObservationBelinda LapsitNo ratings yet
- List of International Days and WeeksDocument10 pagesList of International Days and WeeksSatram RoopaniNo ratings yet
- Jurnal Skripsi Anestesi 4Document8 pagesJurnal Skripsi Anestesi 4Tiara Anggun NurartoNo ratings yet
- Stree Rog 4Document11 pagesStree Rog 4Sambamurthi Punninnair NarayanNo ratings yet
- Pentasa Tablets and Sachets PIDocument14 pagesPentasa Tablets and Sachets PIGeo GeoNo ratings yet
- Guidelines For Case Classification For The National Birth Defects Prevention StudyDocument9 pagesGuidelines For Case Classification For The National Birth Defects Prevention Studyjorge davidNo ratings yet
- Soal BIGDocument12 pagesSoal BIGRifNo ratings yet
- The Periodontal Pocket: Intended Learning OutcomesDocument4 pagesThe Periodontal Pocket: Intended Learning OutcomesREHAB ABBASNo ratings yet
- Dentoalveolar Injuries and Wiring TechniquesDocument60 pagesDentoalveolar Injuries and Wiring Techniquessamys2ndemailNo ratings yet
- Clobazam As First Add On What Is The Evidence and Experience - Final Deck - 14 Feb 2023Document51 pagesClobazam As First Add On What Is The Evidence and Experience - Final Deck - 14 Feb 2023veerraju tvNo ratings yet
- Vaccination Form (Sample)Document1 pageVaccination Form (Sample)Godfrey Loth Sales Alcansare Jr.No ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Viastar Blue Oral Dissolving Film 50 MG - Sildenafil Sitrat - DKI1953300196A1 - 2019Document17 pagesViastar Blue Oral Dissolving Film 50 MG - Sildenafil Sitrat - DKI1953300196A1 - 2019RIRINo ratings yet
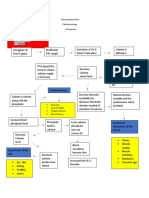
- Hypoparathyroidism PathophysiologyDocument1 pageHypoparathyroidism PathophysiologymaricarNo ratings yet
- Traditional Zootherapeutic Uses in The Treatment of Asthma by The Ethnic Groups of Assam, IndiaDocument5 pagesTraditional Zootherapeutic Uses in The Treatment of Asthma by The Ethnic Groups of Assam, IndiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Pemphigus Foliaceus: Fig. 29.13BDocument1 pagePemphigus Foliaceus: Fig. 29.13BCristian QuitoNo ratings yet
- Resusciation Equipments in IcuDocument29 pagesResusciation Equipments in Icuvinoli100% (1)
- First Responders: The Heroes Who Answer Emergency CallsDocument11 pagesFirst Responders: The Heroes Who Answer Emergency CallsDIANA MARIE MOTA ABREUNo ratings yet
- ConjunctivitisDocument15 pagesConjunctivitisPuviyarasiNo ratings yet
- Transportation in Animals and Plants Worksheet 7Document2 pagesTransportation in Animals and Plants Worksheet 7Parul ShahNo ratings yet
- First Aid For BurnsDocument10 pagesFirst Aid For BurnsRalc Retsel AtadNo ratings yet
- A Study of Stigma and Discrimination Towards People Living With Hiv/AidsDocument20 pagesA Study of Stigma and Discrimination Towards People Living With Hiv/Aidsmusamuwaga100% (1)
- Hydrotherapy Principles & TechniquesDocument75 pagesHydrotherapy Principles & TechniquesSANLAPAN SAHOONo ratings yet
- Week1 - NAILCARE (Sek)Document2 pagesWeek1 - NAILCARE (Sek)rhyzeneNo ratings yet
- OMES-protocol OMDDocument9 pagesOMES-protocol OMDMaritzashuNo ratings yet
- Uts Advocacy PaperDocument11 pagesUts Advocacy PaperPlu AldiniNo ratings yet
- FNCPDocument4 pagesFNCPJonalyn Tumanguil100% (2)
- What Is Nano Silver - Nano Silver PDFDocument2 pagesWhat Is Nano Silver - Nano Silver PDFvijuNo ratings yet
- Flutter IFU New Size - 14 Lang - Iss2 01Document88 pagesFlutter IFU New Size - 14 Lang - Iss2 01Nandhini SivakumarNo ratings yet
- TRAFFIC JAM in EVERESTDocument18 pagesTRAFFIC JAM in EVERESTSB100% (1)
- Treatment of Acute BronchitisDocument3 pagesTreatment of Acute BronchitisjokosudibyoNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)