You might also like
- Surpac IntroductionDocument207 pagesSurpac IntroductionKrist Jan Jimenez Separa0% (1)
- Climaveneta CVM 20 ManualDocument20 pagesClimaveneta CVM 20 ManualisaNo ratings yet
- Reliability of One Ceph Software in Cephalometric Tracing: A Comparative StudyDocument5 pagesReliability of One Ceph Software in Cephalometric Tracing: A Comparative StudyBeniyaNo ratings yet
- A Comparison of Cephalometric Measurements Obtained Using Conventional and Digital MethodsDocument7 pagesA Comparison of Cephalometric Measurements Obtained Using Conventional and Digital MethodsNereo LopezNo ratings yet
- Evaluation of An Online Website-Based Platform For Cephalometric AnalysisDocument5 pagesEvaluation of An Online Website-Based Platform For Cephalometric AnalysisMartha Lia Castaño EcheverryNo ratings yet
- DMF 41 011 PDFDocument7 pagesDMF 41 011 PDFDenis KimNo ratings yet
- Andriola Et Al 2021 Computed Tomography Imaging Superimposition Protocols To Assess Outcomes in Orthognathic Surgery ADocument14 pagesAndriola Et Al 2021 Computed Tomography Imaging Superimposition Protocols To Assess Outcomes in Orthognathic Surgery AmlnunezNo ratings yet
- Majalah IKORTI Juni 2015Document50 pagesMajalah IKORTI Juni 2015istidaristiviaNo ratings yet
- Comparisons of Cephalometric Image Analysis by Information Technology (IT) in The Treatment of Dentomaxillofacial ChangesDocument20 pagesComparisons of Cephalometric Image Analysis by Information Technology (IT) in The Treatment of Dentomaxillofacial ChangesIJAERS JOURNALNo ratings yet
- 66 JPR D 20 00116Document13 pages66 JPR D 20 00116AncikNo ratings yet
- A Comparative Study On Use of Manual Versus Digital Method Using Mobile Application For Cephalometric MeasurementsDocument6 pagesA Comparative Study On Use of Manual Versus Digital Method Using Mobile Application For Cephalometric MeasurementsBeniyaNo ratings yet
- Suresh2022 PDFDocument8 pagesSuresh2022 PDFFilipe do Carmo Barreto DiasNo ratings yet
- Articulo 18Document9 pagesArticulo 18Carlos A Neira MartínezNo ratings yet
- 49-Article Text-153-3-10-20200225Document12 pages49-Article Text-153-3-10-20200225yohanNo ratings yet
- Assessment of The Reliability of Automatic Cephalometric Analysis SoftwareDocument6 pagesAssessment of The Reliability of Automatic Cephalometric Analysis SoftwareMartha Lia Castaño EcheverryNo ratings yet
- Determining The Effective Number and Surfaces of TDocument11 pagesDetermining The Effective Number and Surfaces of TTerem TebautaNo ratings yet
- The Accuracy of Implant Placement With Computer-GuidedDocument11 pagesThe Accuracy of Implant Placement With Computer-GuidedRyan Ardi PradanaNo ratings yet
- Dolphin For Ortho SurgDocument8 pagesDolphin For Ortho Surglohith dNo ratings yet
- Albarakati DMF 2012Document7 pagesAlbarakati DMF 2012RidzNo ratings yet
- Al-Rimawi Et Al-2019-Clinical Oral Implants ResearchDocument7 pagesAl-Rimawi Et Al-2019-Clinical Oral Implants ResearchSohaib ShujaatNo ratings yet
- J of Oral Rehabilitation - 2017 - Jokstad - Computer Assisted Technologies Used in Oral Rehabilitation and The ClinicalDocument30 pagesJ of Oral Rehabilitation - 2017 - Jokstad - Computer Assisted Technologies Used in Oral Rehabilitation and The ClinicalJorge AlvaradoNo ratings yet
- Comparative Assessment of Complete-Coverage, Fixed Tooth-Supported Prostheses Fabricated From Digital Scans or Conventional Impressions A Systematic Review and Meta-AnalysisDocument9 pagesComparative Assessment of Complete-Coverage, Fixed Tooth-Supported Prostheses Fabricated From Digital Scans or Conventional Impressions A Systematic Review and Meta-Analysis박소영No ratings yet
- Orthod Craniofacial Res - 2021 - Bulatova - Assessment of Automatic Cephalometric Landmark Identification Using ArtificialDocument6 pagesOrthod Craniofacial Res - 2021 - Bulatova - Assessment of Automatic Cephalometric Landmark Identification Using ArtificialPaulusMetehNo ratings yet
- 1 s2.0 S2214785317332091 MainDocument8 pages1 s2.0 S2214785317332091 Mainsomeonefromsomwhere123No ratings yet
- Usability Issues in The Operating Room - Towards CDocument10 pagesUsability Issues in The Operating Room - Towards CEduardo NeriNo ratings yet
- Tin Hco Mau-Jcm-10-02661-V2Document10 pagesTin Hco Mau-Jcm-10-02661-V2Phạm CườngNo ratings yet
- Voxel-Based Superimposition of Cone Beam CT Scans For Orthodontic and Craniofacial Follow-Up Overview and Clinical ImplementationDocument21 pagesVoxel-Based Superimposition of Cone Beam CT Scans For Orthodontic and Craniofacial Follow-Up Overview and Clinical ImplementationPhachara SiripraphonrojNo ratings yet
- Preprints202308 1683 v1Document9 pagesPreprints202308 1683 v1SushmaNo ratings yet
- Using A Clinical Protocol For Orthognathic Surgery and Assessing A 3-Dimensional Virtual ApproachDocument15 pagesUsing A Clinical Protocol For Orthognathic Surgery and Assessing A 3-Dimensional Virtual ApproachKorkmaz SayınsuNo ratings yet
- Prediction of Lip Response To Orthodontic TreatmenDocument8 pagesPrediction of Lip Response To Orthodontic TreatmenhabeebNo ratings yet
- DentHypotheses5384-434005 120320Document14 pagesDentHypotheses5384-434005 120320preethi.badamNo ratings yet
- Jud2020 Article ApplicabilityOfAugmentedRealitDocument13 pagesJud2020 Article ApplicabilityOfAugmentedRealitmohadeseNo ratings yet
- Longo Et Al 2021 Augmented Reality, Virtual ReaDocument13 pagesLongo Et Al 2021 Augmented Reality, Virtual ReaLeandro Magno Correa da SilvaNo ratings yet
- Uso de Sistemas de Impresion Digital Con Scaners Intraorales para Fabricacion de Protesis FijaDocument7 pagesUso de Sistemas de Impresion Digital Con Scaners Intraorales para Fabricacion de Protesis FijaPaola Alexandra LaguadoNo ratings yet
- Accuracy of Dental Implant Surgery Using Dynamic Navigation and Robotic Systems - An in Vitro StudyDocument8 pagesAccuracy of Dental Implant Surgery Using Dynamic Navigation and Robotic Systems - An in Vitro StudyAlejandra MonsalveNo ratings yet
- Joda 2016Document6 pagesJoda 2016Juan MusanNo ratings yet
- 1 s2.0 S0022391321004856 MainDocument8 pages1 s2.0 S0022391321004856 Main安西 泰規No ratings yet
- Digital OrthodonticsDocument16 pagesDigital OrthodonticsDharmapadmi KasilaniNo ratings yet
- Dokumen - Tips A Fully Digital Workflow and Device Manufacturing For The Use of Intraoral ScannersDocument6 pagesDokumen - Tips A Fully Digital Workflow and Device Manufacturing For The Use of Intraoral ScannersdentureNo ratings yet
- Ijerph 19 04719 v2Document6 pagesIjerph 19 04719 v2ade apriediNo ratings yet
- 2022 Facial Scanning Techonologies in The Era of Digital Workflow A Systematic Review and Network Meta AnalysisDocument16 pages2022 Facial Scanning Techonologies in The Era of Digital Workflow A Systematic Review and Network Meta AnalysisVivian LiNo ratings yet
- 1 s2.0 S030057122200210X MainDocument10 pages1 s2.0 S030057122200210X MainFlávia de Souza BastosNo ratings yet
- Reproducibility of Measurements in Tablet-Assisted, PC-aided, and Manual Cephalometric AnalysisDocument6 pagesReproducibility of Measurements in Tablet-Assisted, PC-aided, and Manual Cephalometric AnalysissunilNo ratings yet
- Clinical Oral Implants Res - 2018 - Tahmaseb - The Accuracy of Static Computer Aided Implant Surgery A Systematic ReviewDocument20 pagesClinical Oral Implants Res - 2018 - Tahmaseb - The Accuracy of Static Computer Aided Implant Surgery A Systematic ReviewOctavioJose DuarteFrenkyNo ratings yet
- NDT and E International: Miguel Reseco Bato, Anis Hor, Aurelien Rautureau, Christian BesDocument13 pagesNDT and E International: Miguel Reseco Bato, Anis Hor, Aurelien Rautureau, Christian BesJORGE WILFREDO VERA ALVARADONo ratings yet
- Ipa16 138 SGDocument10 pagesIpa16 138 SGChairul IkhwanNo ratings yet
- Pubb 1 BDJ The Accuracy of Intral Oral Scanners FinalDocument13 pagesPubb 1 BDJ The Accuracy of Intral Oral Scanners Finalmarcofriuli2No ratings yet
- tmpDA24 TMPDocument3 pagestmpDA24 TMPFrontiersNo ratings yet
- Guide Design of Precision Tool Handle Based On Ergonomics CriteriaDocument7 pagesGuide Design of Precision Tool Handle Based On Ergonomics CriteriaFainer Cerpa OliveraNo ratings yet
- EU Digital Pathology Workflow Guidelines 2021Document21 pagesEU Digital Pathology Workflow Guidelines 2021patolog32No ratings yet
- Implementation of UI Based On Gesture Recognition For Hospital Enquiry SystemDocument10 pagesImplementation of UI Based On Gesture Recognition For Hospital Enquiry SystemIJRASETPublicationsNo ratings yet
- Three-Dimensional Assessment of Virtual Bracket Removal For Orthodontic Retainers: A Prospective Clinical StudyDocument10 pagesThree-Dimensional Assessment of Virtual Bracket Removal For Orthodontic Retainers: A Prospective Clinical StudyAndré DrumondNo ratings yet
- Articulo RelacionadoDocument10 pagesArticulo RelacionadoMarlon Cespedes AlccaNo ratings yet
- Gan2018.PdfComparison of Adaptation BetweenDocument9 pagesGan2018.PdfComparison of Adaptation BetweendentureNo ratings yet
- Validity of A Manual Soft Tissue Profile Prediction Method Following Mandibular Setback OsteotomyDocument10 pagesValidity of A Manual Soft Tissue Profile Prediction Method Following Mandibular Setback OsteotomyMuhammad AleemNo ratings yet
- Robotics: Kinematic Optimization For The Design of A Collaborative Robot End-Effector For Tele-EchographyDocument17 pagesRobotics: Kinematic Optimization For The Design of A Collaborative Robot End-Effector For Tele-EchographyAkashNo ratings yet
- Seok 2015Document3 pagesSeok 2015khalidNo ratings yet
- Semi-Automated Mid-Turbinate Swab Sampling Using A Six Degrees of Freedom Collaborative Robot and CamerasDocument8 pagesSemi-Automated Mid-Turbinate Swab Sampling Using A Six Degrees of Freedom Collaborative Robot and CamerasIAES International Journal of Robotics and AutomationNo ratings yet
- Digital Occlusal Analysis and Oral Health-Related Quality of Life of Patients With 3D Printed Complete Dentures Versus Conventional DenturesDocument12 pagesDigital Occlusal Analysis and Oral Health-Related Quality of Life of Patients With 3D Printed Complete Dentures Versus Conventional DenturesIJAR JOURNALNo ratings yet
- Intraoral Versus Extraoral Digital Occlusal Records: A Pilot StudyDocument6 pagesIntraoral Versus Extraoral Digital Occlusal Records: A Pilot StudybrandonNo ratings yet
- ComparingScannerPrecision FinalDocument23 pagesComparingScannerPrecision Finalnegmenas2No ratings yet
- Residual Life Prediction and Optimal Maintenance Decision for a Piece of EquipmentFrom EverandResidual Life Prediction and Optimal Maintenance Decision for a Piece of EquipmentNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)nitish mahatoNo ratings yet
- Randomized Controlled Trials: The Technique and Challenges: Special Article: IOS 50 Year Commemorative IssueDocument6 pagesRandomized Controlled Trials: The Technique and Challenges: Special Article: IOS 50 Year Commemorative IssueSai KrupaNo ratings yet
- Thiruvenkatachari 2010Document2 pagesThiruvenkatachari 2010Sai KrupaNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)nitish mahatoNo ratings yet
- The Reliability of The Frankfort Horizontal in Roentgenographic CephalometryDocument6 pagesThe Reliability of The Frankfort Horizontal in Roentgenographic CephalometrySai KrupaNo ratings yet
- Functional Jaw Orthopedics For Class II Malocclusion: Where Do We Stand Today?Document9 pagesFunctional Jaw Orthopedics For Class II Malocclusion: Where Do We Stand Today?Sai KrupaNo ratings yet
- Cadman 1975Document24 pagesCadman 1975Sai KrupaNo ratings yet
- Treacher Collins Syndrome: A Systematic Review of Evidence-Based Treatment and RecommendationsDocument14 pagesTreacher Collins Syndrome: A Systematic Review of Evidence-Based Treatment and RecommendationsSai KrupaNo ratings yet
- Cadman 1975Document36 pagesCadman 1975Sai KrupaNo ratings yet
- Of Orthodontics: American JournalDocument18 pagesOf Orthodontics: American JournalSai KrupaNo ratings yet
- Treacher Collins Syndrome: A Case ReviewDocument6 pagesTreacher Collins Syndrome: A Case ReviewSai KrupaNo ratings yet
- Bastian 2020Document12 pagesBastian 2020Sai KrupaNo ratings yet
- Bastian 2020Document12 pagesBastian 2020Sai KrupaNo ratings yet
- Treachercollinssyndrome: Albaraa Aljerian,, Mirko S. GilardinoDocument9 pagesTreachercollinssyndrome: Albaraa Aljerian,, Mirko S. GilardinoSai KrupaNo ratings yet
- Mouthguardsandorthodonticpatients: Features SectionDocument6 pagesMouthguardsandorthodonticpatients: Features SectionSai KrupaNo ratings yet
- An Overview of Orthodontic Material Degradation in Oral CavityDocument10 pagesAn Overview of Orthodontic Material Degradation in Oral CavitySai KrupaNo ratings yet
- Review Article: Jan/MarDocument6 pagesReview Article: Jan/MarSai KrupaNo ratings yet
- The Removable Orthodontic App&xwe: Frans P.G.M. Van Der Linden The NetherlandsDocument10 pagesThe Removable Orthodontic App&xwe: Frans P.G.M. Van Der Linden The NetherlandsSai KrupaNo ratings yet
- Prevalence and Risk Indicators of Non-Carious Cervical Lesions in Male FootballersDocument9 pagesPrevalence and Risk Indicators of Non-Carious Cervical Lesions in Male FootballersSai KrupaNo ratings yet
- Jios - Jios 224 17Document5 pagesJios - Jios 224 17Sai KrupaNo ratings yet
- Socioeconomic Status Scales Modified Kuppuswamy and Udai Pareekh's Scale Updated For 2019Document4 pagesSocioeconomic Status Scales Modified Kuppuswamy and Udai Pareekh's Scale Updated For 2019Sai KrupaNo ratings yet
- Australian Orthodontic Wires PDFDocument5 pagesAustralian Orthodontic Wires PDFRebin AliNo ratings yet
- Stainless SteelDocument33 pagesStainless SteelSai KrupaNo ratings yet
- Mandibular Changes Produced by Functional Appliances in Class II Malocclusion: A Systematic ReviewDocument13 pagesMandibular Changes Produced by Functional Appliances in Class II Malocclusion: A Systematic ReviewSai KrupaNo ratings yet
- White Coated Niti WiresDocument8 pagesWhite Coated Niti WiresSai KrupaNo ratings yet
- Stainless Steel in OrthodonticsDocument45 pagesStainless Steel in OrthodonticsSai KrupaNo ratings yet
- White Coated Niti WiresDocument8 pagesWhite Coated Niti WiresSai KrupaNo ratings yet
- The Quad Helix Appliance: Ruel W. BenchDocument7 pagesThe Quad Helix Appliance: Ruel W. BenchSai KrupaNo ratings yet
- Bishara2008 PDFDocument9 pagesBishara2008 PDFSai KrupaNo ratings yet
- DO RequestDocument3 pagesDO RequestAhmed IsmailNo ratings yet
- CTR Manufacturing Develops 2 Tap Changer Transformers With FR3 Fluid 1Document5 pagesCTR Manufacturing Develops 2 Tap Changer Transformers With FR3 Fluid 1SM KNo ratings yet
- Sae Summer KepsDocument6 pagesSae Summer KepsPritesh KumarNo ratings yet
- Contoh Report Jar TestDocument12 pagesContoh Report Jar TestIzzat75% (4)
- WIND LOADS (Computation of QH For MWFRS, Low Rise BuildingDocument2 pagesWIND LOADS (Computation of QH For MWFRS, Low Rise BuildingRomeo QuerubinNo ratings yet
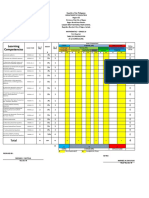
- Learning Competencies: TotalDocument4 pagesLearning Competencies: TotalLaira Joy Salvador - ViernesNo ratings yet
- Pac3A Sect 600 EarthworksDocument66 pagesPac3A Sect 600 EarthworksazizuddinNo ratings yet
- SEAWEEDDocument118 pagesSEAWEEDJeromeGenilanNo ratings yet
- Excel CheatsheetDocument1 pageExcel CheatsheetBoring BlandNo ratings yet
- Singapore DTL Signalling by Joana Lee (Siemens Pte LTD) 18th Nov 2016Document23 pagesSingapore DTL Signalling by Joana Lee (Siemens Pte LTD) 18th Nov 2016Rizky Harry SungguhNo ratings yet
- Che Vol1Document139 pagesChe Vol1abiramanNo ratings yet
- Remy Hvh250 Application Manual: Preliminary Draft Hvh250 Motormanual20110407.Doc Page 1 of 31Document31 pagesRemy Hvh250 Application Manual: Preliminary Draft Hvh250 Motormanual20110407.Doc Page 1 of 31David WalshNo ratings yet
- Ca 3241Document1 pageCa 3241Tien LamNo ratings yet
- SPE 102828 Field Success in Carbonate Acid Diversion, Utilizing Laboratory Data Generated by Parallel Flow TestingDocument14 pagesSPE 102828 Field Success in Carbonate Acid Diversion, Utilizing Laboratory Data Generated by Parallel Flow TestingzachNo ratings yet
- Front Wheel Brake, Brake Pad SensorDocument2 pagesFront Wheel Brake, Brake Pad SensorKifah ZaidanNo ratings yet
- IINNO Catalogue2012 01 SMART 021112 B PDFDocument25 pagesIINNO Catalogue2012 01 SMART 021112 B PDFmiraijewelsNo ratings yet
- Inspection and Testing of OC/EF Protection Relay: Relay Site Test ReportDocument3 pagesInspection and Testing of OC/EF Protection Relay: Relay Site Test ReportMASUD RANANo ratings yet
- CLA Unit I Matrices QB StudentDocument24 pagesCLA Unit I Matrices QB StudentPranil ShivarkarNo ratings yet
- F15-04 (2013) Standard Specification For Iron-Nickel-Cobalt Sealing AlloyDocument7 pagesF15-04 (2013) Standard Specification For Iron-Nickel-Cobalt Sealing Alloymercab15No ratings yet
- EMV Multi Cable Transit Modular System (EMC-System) : PDFDocument7 pagesEMV Multi Cable Transit Modular System (EMC-System) : PDFbakien-canNo ratings yet
- Anti-Domination Number of A Graph: MallikarjunbasannakattimaniDocument5 pagesAnti-Domination Number of A Graph: MallikarjunbasannakattimaniajmrdNo ratings yet
- Keyop Functions 9F3715Document114 pagesKeyop Functions 9F3715Art MessickNo ratings yet
- Introduction To DSADocument11 pagesIntroduction To DSAdhiraj1223353No ratings yet
- BalancesDocument8 pagesBalancescchauling6841No ratings yet
- CSS - 05-Module 5.2 - Network Devices1Document6 pagesCSS - 05-Module 5.2 - Network Devices1Elixa HernandezNo ratings yet
- Vastu ShastraDocument36 pagesVastu ShastraAnjanaya Lamani0% (1)
- Pupalaikis - S Parameters For Signal IntegrityDocument666 pagesPupalaikis - S Parameters For Signal IntegrityzhangwenNo ratings yet
- Web Technology QuantumDocument335 pagesWeb Technology QuantumabhishekgsNo ratings yet