You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- OB Gyne Clinical and Teaching CasesDocument221 pagesOB Gyne Clinical and Teaching CaseszzNo ratings yet
- FAQs For Doctors-PEDIADocument11 pagesFAQs For Doctors-PEDIAzzNo ratings yet
- PPROMDocument1 pagePPROMzzNo ratings yet
- SEC A Pharma Drugs PDFDocument11 pagesSEC A Pharma Drugs PDFzzNo ratings yet
- Question # 1 Identify Patient Problem and Discuss PathophysiologyDocument2 pagesQuestion # 1 Identify Patient Problem and Discuss PathophysiologyzzNo ratings yet
- Urology PDFDocument24 pagesUrology PDFzzNo ratings yet
- Pharmacology Lab DrugsDocument14 pagesPharmacology Lab DrugszzNo ratings yet
- Case Report:: TH TH THDocument6 pagesCase Report:: TH TH THzzNo ratings yet
- MCQ On PhototherapyDocument12 pagesMCQ On Phototherapylumina.s100% (1)
- Slagle AnnotationDocument2 pagesSlagle Annotationapi-270744371No ratings yet
- Early Detection and Intervention of Autism Spectrum DisorderDocument7 pagesEarly Detection and Intervention of Autism Spectrum DisorderIgnacio WettlingNo ratings yet
- Introduction To Physiotherapy: Prepared By, Dr. Sonia Bhatia (P.T.)Document25 pagesIntroduction To Physiotherapy: Prepared By, Dr. Sonia Bhatia (P.T.)Sankalp BhatiyaNo ratings yet
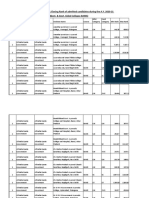
- Category-Wise Opening & Closing Rank of Admitted Candidates During The A.Y. 2020-21 (Govt. & Govt. Aided Colleges-BAMS)Document90 pagesCategory-Wise Opening & Closing Rank of Admitted Candidates During The A.Y. 2020-21 (Govt. & Govt. Aided Colleges-BAMS)Priti LokhandeNo ratings yet
- ExamView - Chapter - 04Document14 pagesExamView - Chapter - 04Stella WangNo ratings yet
- Encephalitis PathophysiologyDocument19 pagesEncephalitis PathophysiologyHeron Bayanin80% (5)
- Accu Chek Guide Manual enDocument132 pagesAccu Chek Guide Manual enAlex XanderNo ratings yet
- 3 - Risk assemt.-DB & SMPDocument4 pages3 - Risk assemt.-DB & SMPAraf KalamNo ratings yet
- Anorexia Case StudyDocument1 pageAnorexia Case StudyRosalva GonzalezNo ratings yet
- Hypothyroidism Concept MapDocument1 pageHypothyroidism Concept Mapel shilohNo ratings yet
- Facts About Sudden Cardiac ArrestDocument2 pagesFacts About Sudden Cardiac ArrestZeljko LekovicNo ratings yet
- Minnesota Health PDFDocument34 pagesMinnesota Health PDFamacksoftNo ratings yet
- Musculoskeletal AssessmentDocument61 pagesMusculoskeletal Assessmentjoreynee100% (3)
- History of Arbovirology: Memories From The Field: Nikos Vasilakis Laura D. Kramer EditorsDocument552 pagesHistory of Arbovirology: Memories From The Field: Nikos Vasilakis Laura D. Kramer Editorsjulio castilloNo ratings yet
- Primary Immunodeficiency DiseasesDocument20 pagesPrimary Immunodeficiency Diseasesodhiambo samwelNo ratings yet
- Bilateral External Carotid Artery Ligation A LifeDocument3 pagesBilateral External Carotid Artery Ligation A LifeYoshua Eric IrawanNo ratings yet
- Obstructive Sleep Apnea-Hypopnea SyndromeDocument31 pagesObstructive Sleep Apnea-Hypopnea SyndromeAída TreviñoNo ratings yet
- Prometric and Bahrain National Health Regulatory Authority (Nhra) Begin Strategic AllianceDocument1 pagePrometric and Bahrain National Health Regulatory Authority (Nhra) Begin Strategic AllianceVelimir RadojicicNo ratings yet
- Gordon's Functional Health PatternDocument5 pagesGordon's Functional Health Patternnerlyn100% (1)
- Diagnosing Anemia Algorithm HandoutDocument2 pagesDiagnosing Anemia Algorithm HandoutValentino Farroñay TafurNo ratings yet
- Tugas Tutorial Ke-3 - Mkwi4201Document6 pagesTugas Tutorial Ke-3 - Mkwi4201Yupi's StudioNo ratings yet
- 13 Demyelinating DiseaseDocument8 pages13 Demyelinating DiseasemgvbNo ratings yet
- Sialorrea PDFDocument6 pagesSialorrea PDFVerónica RuizNo ratings yet
- Epidemiology: Andre Bencee V. Barimbao, RMT, MLS (ASCP)Document55 pagesEpidemiology: Andre Bencee V. Barimbao, RMT, MLS (ASCP)Alondra Aran100% (2)
- India 2Document132 pagesIndia 2Bala KrishnanNo ratings yet
- Incubator Infant PDFDocument1 pageIncubator Infant PDFWondwosen TadesseNo ratings yet
- (PHA6118 Lec) Introduction To PharmacologyDocument5 pages(PHA6118 Lec) Introduction To Pharmacologychristian redotaNo ratings yet
- 22q11.2 Deletion Syndrome - GeneReviews® - NCBI Bookshelf PDFDocument33 pages22q11.2 Deletion Syndrome - GeneReviews® - NCBI Bookshelf PDFZol NnadozieNo ratings yet
- MudrasDocument3 pagesMudrasPraveen Alinkeel100% (1)