You might also like
- Mnemonics Anatomy 1st SemDocument4 pagesMnemonics Anatomy 1st SemNastassja Callmedoctor Douse67% (3)
- HSE Report On Mooring IntegrityDocument313 pagesHSE Report On Mooring IntegritysanumajNo ratings yet
- Ovarian TorsionDocument4 pagesOvarian TorsionRiko KuswaraNo ratings yet
- Cerebral PalsyDocument24 pagesCerebral PalsyUday Kumar100% (1)
- MANAURITE XM Material PDFDocument8 pagesMANAURITE XM Material PDFkbc404No ratings yet
- FF4 58 Service Manual ERQU40E3HUSDocument20 pagesFF4 58 Service Manual ERQU40E3HUSCarmen Adriana Garcia MendozaNo ratings yet
- Learning Activity Sheet In: Computer Systems ServicingDocument12 pagesLearning Activity Sheet In: Computer Systems ServicingCarvalds 0315No ratings yet
- Fmea PC ProcessDocument2 pagesFmea PC Processsudeep_singh1No ratings yet
- Kumiko Jigs Japanese Woodworking PDFDocument9 pagesKumiko Jigs Japanese Woodworking PDFJaime Montiel100% (1)
- Prune Belly SyndromeDocument39 pagesPrune Belly SyndromeHudaNo ratings yet
- Present Perfect and Simple Past Tenses in ESL Grammar ExercisesDocument36 pagesPresent Perfect and Simple Past Tenses in ESL Grammar ExercisesNguyen Quoc AnhNo ratings yet
- Table Napkin Folding TechniquesDocument6 pagesTable Napkin Folding TechniquesMiguel BaricuatroNo ratings yet
- Duodenal AtresiaDocument18 pagesDuodenal AtresiaRianto Noviady RamliNo ratings yet
- Case Report on Duodenal Stenosis in a 3rd Month BoyDocument15 pagesCase Report on Duodenal Stenosis in a 3rd Month BoyMuhammad Khairuna SyahPutraNo ratings yet
- 2022ClinPerinatology Mowrer AbdominalWallDefect AReviewDocument11 pages2022ClinPerinatology Mowrer AbdominalWallDefect AReviewdarkangelmx1No ratings yet
- Gastroschisis: Case ReportDocument2 pagesGastroschisis: Case ReportMuhammad Syamil RozlanNo ratings yet
- Advances in Prenatal and Perinatal Diagnosis and Management of GastroschisisDocument36 pagesAdvances in Prenatal and Perinatal Diagnosis and Management of GastroschisisLondonNo ratings yet
- Ecgds 09 00916Document4 pagesEcgds 09 00916Houda El MoufidNo ratings yet
- Abstract ReferenceDocument10 pagesAbstract ReferenceOvamelia JulioNo ratings yet
- Kayatsha - Gastroschisis and Omphalocele A Case ReportDocument4 pagesKayatsha - Gastroschisis and Omphalocele A Case ReportAffannul HakimNo ratings yet
- Hisprung JurnalDocument14 pagesHisprung JurnalWiwit ClimberNo ratings yet
- Late Third Trimester Prenatal Ultrasound Diagnosis of Duodenal AtresiaDocument4 pagesLate Third Trimester Prenatal Ultrasound Diagnosis of Duodenal AtresiaIful SaifullahNo ratings yet
- Medicine: A Newborn Patient With Both Annular Pancreas and Meckel 'S DiverticulumDocument5 pagesMedicine: A Newborn Patient With Both Annular Pancreas and Meckel 'S DiverticulumAdrian UmbriaNo ratings yet
- Prune Belly SyndromeDocument33 pagesPrune Belly SyndromePrasanna KumarNo ratings yet
- Pediatric Clinics of North America IIDocument54 pagesPediatric Clinics of North America IIkarenNo ratings yet
- GastroschisisDocument17 pagesGastroschisisAsterisa PutriNo ratings yet
- Neonatal Bowel Obstructions GuideDocument27 pagesNeonatal Bowel Obstructions GuideNaty BmNo ratings yet
- PSU Vol 06, 1996Document5 pagesPSU Vol 06, 1996rajarshikNo ratings yet
- Gastro SCH Is IsDocument13 pagesGastro SCH Is IsferoNo ratings yet
- Small Bowel ObstructionDocument4 pagesSmall Bowel ObstructionRayhanun MardhatillahNo ratings yet
- Adult Bowel Intussusception: Presentation, Location, Etiology, Diagnosis and TreatmentDocument4 pagesAdult Bowel Intussusception: Presentation, Location, Etiology, Diagnosis and TreatmentRizki Ismi Arsyad IINo ratings yet
- Prenatal diagnosis of gastroschisis by ultrasoundDocument5 pagesPrenatal diagnosis of gastroschisis by ultrasoundhakimrosliNo ratings yet
- Abdomina Wall Defects 2Document12 pagesAbdomina Wall Defects 2pamellapesseNo ratings yet
- Prenatal Diagnosis and Successful Surgical Treatment of Gastrochisis: Case ReportDocument4 pagesPrenatal Diagnosis and Successful Surgical Treatment of Gastrochisis: Case ReportIJAR JOURNALNo ratings yet
- Gallbladder Diseases in PregnancyDocument7 pagesGallbladder Diseases in PregnancyAnonymous 9QxPDpNo ratings yet
- Idiopathic Sclerosing Encapsulating Peritonitis: Abdominal CocoonDocument6 pagesIdiopathic Sclerosing Encapsulating Peritonitis: Abdominal CocoonRameshKumarNo ratings yet
- Hirschsprung DiseaseDocument44 pagesHirschsprung DiseaseAhmad Abu KushNo ratings yet
- Aproximación Multidisciplinaria Al Diagnóstico y Tratamiento de La Obs Intestinal 2018Document124 pagesAproximación Multidisciplinaria Al Diagnóstico y Tratamiento de La Obs Intestinal 2018Jorge Nuñez LucicNo ratings yet
- Atresia of Jejunum and IleumDocument5 pagesAtresia of Jejunum and IleumTiffany AdelinaNo ratings yet
- Duodenal Atresia and Stenosis: Emily Partridge and Holly L. HedrickDocument7 pagesDuodenal Atresia and Stenosis: Emily Partridge and Holly L. HedrickWahyu IndraNo ratings yet
- Propedeutics - Barrett's Esophagus - SMSDocument18 pagesPropedeutics - Barrett's Esophagus - SMSSafeer VarkalaNo ratings yet
- A Comprehensive Analysis of 51 Neonates With Congenital Intestinal AtresiaDocument5 pagesA Comprehensive Analysis of 51 Neonates With Congenital Intestinal AtresiaSilverius Seantoni SabellaNo ratings yet
- Anak BangsalDocument4 pagesAnak BangsalRegina AyediaNo ratings yet
- Imaging of Congenital Anomalies of The Gastrointestinal TractDocument12 pagesImaging of Congenital Anomalies of The Gastrointestinal TractMateen ShukriNo ratings yet
- A Pattern Based Approach To The Bowel Obstruction in The NewbornDocument12 pagesA Pattern Based Approach To The Bowel Obstruction in The Newborntiosam59100% (1)
- Duodenal Stenosis from Midgut Malrotation and Ladd's BandDocument1 pageDuodenal Stenosis from Midgut Malrotation and Ladd's BandKevinJuliusTanadyNo ratings yet
- Prenatal Diagnosis of Anterior Abdominal Wall Defects: Pictorial EssayDocument12 pagesPrenatal Diagnosis of Anterior Abdominal Wall Defects: Pictorial EssayNurul ArdaniNo ratings yet
- International Journal of Pharmaceutical Science Invention (IJPSI)Document3 pagesInternational Journal of Pharmaceutical Science Invention (IJPSI)inventionjournalsNo ratings yet
- Title: A Case Report On Left-Sided AppendicitisDocument10 pagesTitle: A Case Report On Left-Sided Appendicitishom lakshmiNo ratings yet
- LAPcarlberg 2016Document21 pagesLAPcarlberg 20164bm5hb2dydNo ratings yet
- Emergency Complications of Hirschsprung DiseaseDocument17 pagesEmergency Complications of Hirschsprung DiseaseAngelica Stephanie MoqueteNo ratings yet
- Pre Fumo 2014Document12 pagesPre Fumo 2014LiaApprilia Kartinii Cupcupcuap ElvenadoNo ratings yet
- Gastric VolvulusDocument6 pagesGastric VolvulusIosif SzantoNo ratings yet
- Brig Anti 2017Document18 pagesBrig Anti 2017Marjorie Lisseth Calderón LozanoNo ratings yet
- Jejunojejunal Intussusception As Initial Presentation of Coeliac Disease: A Case Report and Review of LiteratureDocument6 pagesJejunojejunal Intussusception As Initial Presentation of Coeliac Disease: A Case Report and Review of Literatureellya theresiaNo ratings yet
- Gastroschisis: Prenatal Diagnosis and OutcomeDocument16 pagesGastroschisis: Prenatal Diagnosis and OutcomeEnvhy WinaNo ratings yet
- Prenatal Diagnosis of Abdominal Wall DefectsDocument12 pagesPrenatal Diagnosis of Abdominal Wall DefectsLushaNo ratings yet
- JP2014 239406Document13 pagesJP2014 239406laela varantikaNo ratings yet
- H. pylori gastritis and ulcer diseaseDocument6 pagesH. pylori gastritis and ulcer diseasetambamanuellaNo ratings yet
- GastroschisisDocument19 pagesGastroschisiskunaidongNo ratings yet
- Pseudo Prune Belly Syndrome in FemaleDocument6 pagesPseudo Prune Belly Syndrome in Femalereza kurniawanNo ratings yet
- A Radiologist's Opint of View Darvishzadeh2016Document21 pagesA Radiologist's Opint of View Darvishzadeh2016Agustina ZabiniNo ratings yet
- Article: Adult Hirschsprung Disease As Acute Intestinal Obstruction: A Case ReportDocument7 pagesArticle: Adult Hirschsprung Disease As Acute Intestinal Obstruction: A Case ReportRisky AmaliaNo ratings yet
- Omphalocele and GastroschisisDocument12 pagesOmphalocele and Gastroschisisluisisea100% (1)
- Prenatal Management, Pregnancy and Pediatric Outcomes in Fetuses With Septated Cystic HygromaDocument5 pagesPrenatal Management, Pregnancy and Pediatric Outcomes in Fetuses With Septated Cystic HygromawitaNo ratings yet
- Case 3384: Hirschsprung's Disease in A NeonateDocument6 pagesCase 3384: Hirschsprung's Disease in A NeonatetanushreeNo ratings yet
- Diagnosing and Treating Ovarian TorsionDocument8 pagesDiagnosing and Treating Ovarian TorsionSebastian GandyNo ratings yet
- Case Report Esophageal AtresiaDocument3 pagesCase Report Esophageal Atresiaadriani lawrenciaNo ratings yet
- Guide to Pediatric Urology and Surgery in Clinical PracticeFrom EverandGuide to Pediatric Urology and Surgery in Clinical PracticeNo ratings yet
- Diseases of the Liver and Biliary TreeFrom EverandDiseases of the Liver and Biliary TreeAnnarosa FloreaniNo ratings yet
- Vitamin K Deficiency Bleeding A Case Study: Advances in Neonatal Care December 2013Document7 pagesVitamin K Deficiency Bleeding A Case Study: Advances in Neonatal Care December 2013NasriNo ratings yet
- Case Series: Newborn Haemorrhagic Disorders: About 30 CasesDocument8 pagesCase Series: Newborn Haemorrhagic Disorders: About 30 CasesNasriNo ratings yet
- Innocent Blood: A History of Hemorrhagic Disease of The NewbornDocument7 pagesInnocent Blood: A History of Hemorrhagic Disease of The NewbornNasriNo ratings yet
- 5105 11336 3 PB 2Document18 pages5105 11336 3 PB 2Taufik 81No ratings yet
- Vitamin K deficiency bleeding of newborn masquerading haemophilia BDocument5 pagesVitamin K deficiency bleeding of newborn masquerading haemophilia BNasriNo ratings yet
- Cordelia SlidesCarnivalDocument40 pagesCordelia SlidesCarnivalEnzo Alcívar ThomasNo ratings yet
- Penanganan Hipotiroid Pada Anak Dengan Sindrom Nefrotik: Bernadetha NadeakDocument14 pagesPenanganan Hipotiroid Pada Anak Dengan Sindrom Nefrotik: Bernadetha NadeakMuh FardiansyahNo ratings yet
- Hemorrhagic Disease of Newborn: A Prospective Study of Clinical Features and OutcomeDocument5 pagesHemorrhagic Disease of Newborn: A Prospective Study of Clinical Features and OutcomeIan SutejaNo ratings yet
- FIT Clinical Decision Making: Severe Mitral Stenosis and Pulmonary Hypertension in Pregnancy: When To ActDocument1 pageFIT Clinical Decision Making: Severe Mitral Stenosis and Pulmonary Hypertension in Pregnancy: When To ActNasriNo ratings yet
- Vitamin K Deficiency: A Case Report and Review of Current GuidelinesDocument5 pagesVitamin K Deficiency: A Case Report and Review of Current GuidelinesRB M ESNo ratings yet
- Mutius SlidesCarnivalDocument29 pagesMutius SlidesCarnivaldinar aimcNo ratings yet
- Low-Gradient Severe Mitral Stenosis: Hemodynamic Pro Files, Clinical Characteristics, and OutcomesDocument12 pagesLow-Gradient Severe Mitral Stenosis: Hemodynamic Pro Files, Clinical Characteristics, and OutcomesNasriNo ratings yet
- Degenerative Mitral Stenosis: Interpreting The Meaning of Mean GradientDocument3 pagesDegenerative Mitral Stenosis: Interpreting The Meaning of Mean GradientNasriNo ratings yet
- Case ReportDocument6 pagesCase ReportNasriNo ratings yet
- Assessment of Right Ventricular Dysfunction in Patients With Mitral Stenosis: A Speckle Tracking StudyDocument6 pagesAssessment of Right Ventricular Dysfunction in Patients With Mitral Stenosis: A Speckle Tracking StudyNasriNo ratings yet
- Cardiac Arrest in PregnancyDocument4 pagesCardiac Arrest in PregnancyNasriNo ratings yet
- L2 - RELATO DE CASO - ABC71 - InglesDocument3 pagesL2 - RELATO DE CASO - ABC71 - InglesNasriNo ratings yet
- Assessment of Right Ventricular Dysfunction in Patients With Mitral Stenosis: A Speckle Tracking StudyDocument6 pagesAssessment of Right Ventricular Dysfunction in Patients With Mitral Stenosis: A Speckle Tracking StudyNasriNo ratings yet
- L2 - RELATO DE CASO - ABC71 - InglesDocument3 pagesL2 - RELATO DE CASO - ABC71 - InglesNasriNo ratings yet
- Degenerative Mitral Stenosis: Interpreting The Meaning of Mean GradientDocument3 pagesDegenerative Mitral Stenosis: Interpreting The Meaning of Mean GradientNasriNo ratings yet
- Severe Mitral Stenosis in Patients With Severe Mitral Annular Calci FicationDocument3 pagesSevere Mitral Stenosis in Patients With Severe Mitral Annular Calci FicationNasriNo ratings yet
- L2 - RELATO DE CASO - ABC71 - InglesDocument3 pagesL2 - RELATO DE CASO - ABC71 - InglesNasriNo ratings yet
- FIT Clinical Decision Making: Severe Mitral Stenosis and Pulmonary Hypertension in Pregnancy: When To ActDocument1 pageFIT Clinical Decision Making: Severe Mitral Stenosis and Pulmonary Hypertension in Pregnancy: When To ActNasriNo ratings yet
- Cardiorespiratory ArrestDocument5 pagesCardiorespiratory Arrestore wa IzzampNo ratings yet
- Degenerative Mitral Stenosis: Interpreting The Meaning of Mean GradientDocument3 pagesDegenerative Mitral Stenosis: Interpreting The Meaning of Mean GradientNasriNo ratings yet
- Low-Gradient Severe Mitral Stenosis: Hemodynamic Pro Files, Clinical Characteristics, and OutcomesDocument12 pagesLow-Gradient Severe Mitral Stenosis: Hemodynamic Pro Files, Clinical Characteristics, and OutcomesNasriNo ratings yet
- Doacs in Patients With Mitral Stenosis and Atrial FibrillationDocument3 pagesDoacs in Patients With Mitral Stenosis and Atrial FibrillationNasriNo ratings yet
- Outcomes of Direct Oral Anticoagulants in Patients With Mitral StenosisDocument9 pagesOutcomes of Direct Oral Anticoagulants in Patients With Mitral StenosisNasriNo ratings yet
- Assessment of Right Ventricular Dysfunction in Patients With Mitral Stenosis: A Speckle Tracking StudyDocument6 pagesAssessment of Right Ventricular Dysfunction in Patients With Mitral Stenosis: A Speckle Tracking StudyNasriNo ratings yet
- Calcific Mitral Stenosis: Echoes of AgingDocument3 pagesCalcific Mitral Stenosis: Echoes of AgingNasriNo ratings yet
- Heyer Et Al - 1994 - 5 e 6 - Measuring and Monitoring Biological Diversity. Standard Methods For Amphibians - Preface and Cap1Document8 pagesHeyer Et Al - 1994 - 5 e 6 - Measuring and Monitoring Biological Diversity. Standard Methods For Amphibians - Preface and Cap1Vítor Carvalho RochaNo ratings yet
- H 9906 20 71458 6 0 - DP 8800 DP 9900 Service ManualDocument116 pagesH 9906 20 71458 6 0 - DP 8800 DP 9900 Service ManualChristian Randy Castillo EnríquezNo ratings yet
- Leptospirosis National Guidelines - Sri LankaDocument56 pagesLeptospirosis National Guidelines - Sri LankaBrainy-Paykiesaurus LuminirexNo ratings yet
- "Fragile" - StingDocument4 pages"Fragile" - StingFabián ReinosoNo ratings yet
- Structural Dyanmics-Anna University Q PaperDocument7 pagesStructural Dyanmics-Anna University Q PaperVijay AravindNo ratings yet
- ASME B36.10M-2004 Welded and Seamless Wrought Steel Pipe StandardDocument2 pagesASME B36.10M-2004 Welded and Seamless Wrought Steel Pipe StandardAmit BansalNo ratings yet
- Technical Plan For Roll Forming Machine: Model: WLFM40-250-1000Document5 pagesTechnical Plan For Roll Forming Machine: Model: WLFM40-250-1000ibrahimadiop1No ratings yet
- Water Cycle Cer 002Document2 pagesWater Cycle Cer 002api-434008934No ratings yet
- Users Manual: Documenting Process CalibratorDocument134 pagesUsers Manual: Documenting Process CalibratorSilvaa60No ratings yet
- HYBRIFLEX® RRH Hybrid Cable Solution 12 X 24, 6AWG, Low-Inductance, Single-Mode Fiber, DLC Connectors Top and Bottom, 240 FTDocument3 pagesHYBRIFLEX® RRH Hybrid Cable Solution 12 X 24, 6AWG, Low-Inductance, Single-Mode Fiber, DLC Connectors Top and Bottom, 240 FTNoame Pauline SimbajonNo ratings yet
- CIA Patho 1Document23 pagesCIA Patho 1Suhas H GNo ratings yet
- DPS Nashik Class 12 Science SyllabusDocument18 pagesDPS Nashik Class 12 Science SyllabusSayali Morwal-KumawatNo ratings yet
- 00 - Orientation LessonDocument32 pages00 - Orientation LessonRekha ShahNo ratings yet
- Electronic Control Module (ECM) : Shutdown SIS Previous ScreenDocument5 pagesElectronic Control Module (ECM) : Shutdown SIS Previous ScreenWladimir AmaguañaNo ratings yet
- Thesis Defence Public Presentation FinalDocument16 pagesThesis Defence Public Presentation FinalAlina AndreevNo ratings yet
- Toaz - Info Super Coolant Af Nac PRDocument6 pagesToaz - Info Super Coolant Af Nac PRsugi yantoNo ratings yet
- GX7000 New CatalogeDocument20 pagesGX7000 New CatalogeyohanesNo ratings yet
- Motor ManualDocument4 pagesMotor ManualRemezaNo ratings yet
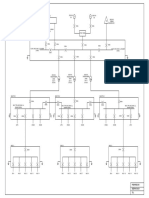
- Conceptual SLDDocument1 pageConceptual SLDakhilNo ratings yet
- Remote Controlled Home Appliances Project ReportDocument5 pagesRemote Controlled Home Appliances Project ReportASHU KNo ratings yet