You might also like
- Radiography Techniques and Safety in Pediatric Dental PatientsDocument125 pagesRadiography Techniques and Safety in Pediatric Dental PatientsHebah NawafNo ratings yet
- Radiology in Pediatric Dentistry 2Document44 pagesRadiology in Pediatric Dentistry 2Aima Cuba100% (1)
- Pe Ads Presnt NTNDocument38 pagesPe Ads Presnt NTNHebah NawafNo ratings yet
- Radiology in Pediatric DentistryDocument125 pagesRadiology in Pediatric DentistryHebah NawafNo ratings yet
- Intra-Oral Radio Graphs For The Pediatric Dental Patient PedoDocument44 pagesIntra-Oral Radio Graphs For The Pediatric Dental Patient PedoFourthMolar.comNo ratings yet
- 3 Radiographic Dental Assessment For The Child Patient PDFDocument21 pages3 Radiographic Dental Assessment For The Child Patient PDFFamodimu Funbi SamuelNo ratings yet
- 4 Intraoral Radiographic TechniquesDocument35 pages4 Intraoral Radiographic TechniquesDan 04100% (1)
- ALARADocument38 pagesALARAMuhammadRizkyRadliyaMaulanaNo ratings yet
- CG A001 04 Radiographs Guideline PDFDocument10 pagesCG A001 04 Radiographs Guideline PDFmahmoudNo ratings yet
- Diagnosis in Orthodontics - Part IIIDocument38 pagesDiagnosis in Orthodontics - Part IIIkaran patelNo ratings yet
- Intra-Oral Radiographic TechniquesDocument163 pagesIntra-Oral Radiographic TechniquesdrdeepsomrNo ratings yet
- Dental Radiography For The Pediatric Patient PedoDocument30 pagesDental Radiography For The Pediatric Patient PedoFourthMolar.comNo ratings yet
- Lec 4Document4 pagesLec 4Dr NisrinNo ratings yet
- Intraoral Radiographic ExaminationDocument79 pagesIntraoral Radiographic Examinationغلاها عبدوNo ratings yet
- Intraoral RadiographsDocument41 pagesIntraoral RadiographsRobins DhakalNo ratings yet
- Panoramic Imaging & Cone Beam Computed TomographyDocument54 pagesPanoramic Imaging & Cone Beam Computed TomographyMenna KhNo ratings yet
- Intraoral Radiographic Techniques ǁ: by Dr. WajnaaDocument32 pagesIntraoral Radiographic Techniques ǁ: by Dr. WajnaaALI abd-alamamNo ratings yet
- Pedo Script 4Document14 pagesPedo Script 4Salam BataienehNo ratings yet
- Recent Advances in Dental Radiography For Pediatric Patients: A ReviewDocument6 pagesRecent Advances in Dental Radiography For Pediatric Patients: A ReviewFebriani SerojaNo ratings yet
- Dental RadiologyDocument134 pagesDental RadiologyDeepak JhaNo ratings yet
- Major Topic Abbreviation: RadiologyDocument105 pagesMajor Topic Abbreviation: Radiologycontrolpane100% (2)
- Intra Oral Radiography: - Presented byDocument34 pagesIntra Oral Radiography: - Presented byNehal MainaliNo ratings yet
- Extraoral Periapical Radiography An Alternative Approach To Intraoral Periapical RadiographyDocument5 pagesExtraoral Periapical Radiography An Alternative Approach To Intraoral Periapical RadiographysevattapillaiNo ratings yet
- An Introduction To RadiographsDocument2 pagesAn Introduction To RadiographsGraceNo ratings yet
- CG A001 05 RadiographsDocument11 pagesCG A001 05 Radiographsishan singhNo ratings yet
- Extraoral Radiographic TechniqueDocument3 pagesExtraoral Radiographic TechniqueimmortalneoNo ratings yet
- Panoramic Radiograph Y Panoramic Radiograph Y: Hiba Shah BSMT Batch Iii Sem4 Dental RadiographyDocument16 pagesPanoramic Radiograph Y Panoramic Radiograph Y: Hiba Shah BSMT Batch Iii Sem4 Dental RadiographyHiba ShahNo ratings yet
- Intraoral Radiographic TechniqueDocument29 pagesIntraoral Radiographic Techniqueabdullah aliNo ratings yet
- Orthodontics - 1st LectureDocument11 pagesOrthodontics - 1st LectureMarwan Qasim GhNo ratings yet
- Radiation Exposure in Pediatric Dentistry: An IntroductionDocument5 pagesRadiation Exposure in Pediatric Dentistry: An Introductionchaithra collegeNo ratings yet
- Intraoral ProjectionsDocument73 pagesIntraoral ProjectionsrespikNo ratings yet
- Recent Advances in Dental RadiographyDocument6 pagesRecent Advances in Dental RadiographyShivani DubeyNo ratings yet
- Dental X-Ray ExamsDocument2 pagesDental X-Ray ExamsSara Loureiro da LuzNo ratings yet
- Normal Dental Radiography in RabbitsDocument9 pagesNormal Dental Radiography in RabbitsMarcelo Anibal AlvarezNo ratings yet
- Diagnosis and Treatment Planning For Edentulous or PotentiallyDocument73 pagesDiagnosis and Treatment Planning For Edentulous or PotentiallyRajsandeep SinghNo ratings yet
- Kodak Radiation Saftey in Dental RadiographyDocument14 pagesKodak Radiation Saftey in Dental RadiographyBala Raghavendra G NNo ratings yet
- Intraoral Projection and Quality Evaluation - Kel 1Document35 pagesIntraoral Projection and Quality Evaluation - Kel 1alzayyanauroraNo ratings yet
- RetrieveDocument7 pagesRetrieve01 X A.A. Gede Reynata Putra XII MIPA 4No ratings yet
- Oral and Maxillofacial Radiology: Oral Surgery Oral Medicine Oral PathologyDocument6 pagesOral and Maxillofacial Radiology: Oral Surgery Oral Medicine Oral PathologynisaNo ratings yet
- NDEB McGill Radiology ReviewDocument3 pagesNDEB McGill Radiology ReviewBrandon HershNo ratings yet
- DA220 Ch1Document32 pagesDA220 Ch1Anne DavisNo ratings yet
- Fundamentals of Oral and Maxillofacial RadiologyFrom EverandFundamentals of Oral and Maxillofacial RadiologyRating: 4 out of 5 stars4/5 (1)
- Need of Lntraoral Periapical Radiographs: 5. Post Extraction Radiographs For Root Fragments and Other Co-Lateral DamagesDocument6 pagesNeed of Lntraoral Periapical Radiographs: 5. Post Extraction Radiographs For Root Fragments and Other Co-Lateral DamagesRifky Al ThariqNo ratings yet
- Chapter 16 - Oral Radiography (Essentials of Dental Assisting)Document96 pagesChapter 16 - Oral Radiography (Essentials of Dental Assisting)mussanteNo ratings yet
- AAPD Radiographic Guidelines 2021Document5 pagesAAPD Radiographic Guidelines 2021SitaResmiListyaNo ratings yet
- Dental RadiologyDocument30 pagesDental RadiologyRobertNo ratings yet
- Modifying Adult IopaDocument2 pagesModifying Adult IopaPramodh PillaiNo ratings yet
- Panoramic RadiographyDocument52 pagesPanoramic RadiographyPuspita Wulansari100% (1)
- Radiation Dose RadiographyDocument17 pagesRadiation Dose RadiographyShivani DubeyNo ratings yet
- L01 DentalDocument61 pagesL01 DentalDeanprint KjayaNo ratings yet
- Extraoral RadiographyDocument33 pagesExtraoral Radiographystig209No ratings yet
- Radiation Protection in Dental RadiographyDocument63 pagesRadiation Protection in Dental Radiographynandani kumariNo ratings yet
- Imaging Patients With Special Needs Mohamad Jaber 202000679Document31 pagesImaging Patients With Special Needs Mohamad Jaber 202000679mhmdNo ratings yet
- Lec 2 Maxillo FacialDocument17 pagesLec 2 Maxillo FacialEman Gamal HelalNo ratings yet
- Lec 2 Maxillo Facialالمرحله الثالثهDocument17 pagesLec 2 Maxillo Facialالمرحله الثالثهEman Gamal HelalNo ratings yet
- Prevent Head and Neck CancersDocument28 pagesPrevent Head and Neck CancersWendy EscalanteNo ratings yet
- Endoscopic Submucosal Dissection: Principles and PracticeFrom EverandEndoscopic Submucosal Dissection: Principles and PracticeNorio FukamiNo ratings yet
- Advanced Colonoscopy: Principles and Techniques Beyond Simple PolypectomyFrom EverandAdvanced Colonoscopy: Principles and Techniques Beyond Simple PolypectomyToyooki SonodaNo ratings yet
- Local Flaps in Facial Reconstruction: A Defect Based ApproachFrom EverandLocal Flaps in Facial Reconstruction: A Defect Based ApproachNo ratings yet
- Recent Advances in Dental Radiography For Pediatric Patients: A ReviewDocument6 pagesRecent Advances in Dental Radiography For Pediatric Patients: A ReviewFebriani SerojaNo ratings yet
- Types of Dental RadiographsDocument9 pagesTypes of Dental RadiographsHebah NawafNo ratings yet
- Periodontal Charting Guide by Dr. Ghadah S. Al-TakroniDocument8 pagesPeriodontal Charting Guide by Dr. Ghadah S. Al-TakroniHebah NawafNo ratings yet
- Paediatric DentalDocument2 pagesPaediatric DentalHebah NawafNo ratings yet
- Paediatric DentalDocument2 pagesPaediatric DentalHebah NawafNo ratings yet
- Dental Traumatology - 2023 - Tsukiboshi - A Step by Step Guide For Autotransplantation of TeethDocument11 pagesDental Traumatology - 2023 - Tsukiboshi - A Step by Step Guide For Autotransplantation of TeethDevin KwanNo ratings yet
- EXERCIȚII PS - PC Discutii DentistDocument6 pagesEXERCIȚII PS - PC Discutii DentistDana C. RyffelNo ratings yet
- Halitosis - Etilogy and PathogenesisDocument26 pagesHalitosis - Etilogy and PathogenesisPrathusha UmakhanthNo ratings yet
- Class I Cavity Preparation for Amalgam RestorationsDocument43 pagesClass I Cavity Preparation for Amalgam RestorationsASHWINI ATHULNo ratings yet
- 6 D11-116 Julia Elodie VlachojannisDocument10 pages6 D11-116 Julia Elodie VlachojannisDr. Neesu KumbhatNo ratings yet
- Periodontal Instruments: Dr. Apeksha Kamble 1St Year Mds Department of PeriodontologyDocument69 pagesPeriodontal Instruments: Dr. Apeksha Kamble 1St Year Mds Department of PeriodontologyAj VishwadheebNo ratings yet
- Daisy S Dancing Lessons .Document30 pagesDaisy S Dancing Lessons .WAHIBNo ratings yet
- Principles and Practice of Implant Dentistry 2001 - Weiss (18-15)Document671 pagesPrinciples and Practice of Implant Dentistry 2001 - Weiss (18-15)jktrj100% (1)
- Endodontic Pain: Paul A. RosenbergDocument24 pagesEndodontic Pain: Paul A. RosenbergArturo Trejo VeraNo ratings yet
- Meta Tags - Cosmodontist DentalDocument2 pagesMeta Tags - Cosmodontist Dentalotos mediaNo ratings yet
- Posterior Palatal Seal AreaDocument8 pagesPosterior Palatal Seal Areaayan ravalNo ratings yet
- Ijerph 18 06796 v2Document24 pagesIjerph 18 06796 v2paolaNo ratings yet
- Fabrication of Complete/partial Dentures (Different Final Impression Techniques and Materials) For Treating Edentulous Patients (Protocol)Document18 pagesFabrication of Complete/partial Dentures (Different Final Impression Techniques and Materials) For Treating Edentulous Patients (Protocol)Padmini ReddyNo ratings yet
- Comprehensive Review On Recent Root Canal Filling Materials and Techniques - An UpdateDocument6 pagesComprehensive Review On Recent Root Canal Filling Materials and Techniques - An Updatedrpriyanka patelNo ratings yet
- Running Head: Digital Custom Implant Impression: Version of Record Doi: 10.1111/jopr.13200Document16 pagesRunning Head: Digital Custom Implant Impression: Version of Record Doi: 10.1111/jopr.13200Roja AllampallyNo ratings yet
- Jadun2019 Endodontic Microsurgery Part 2Document11 pagesJadun2019 Endodontic Microsurgery Part 2Shirley Granados LauraNo ratings yet
- Dental Hygiene: From Prehistoric Killer to Modern NecessityDocument1 pageDental Hygiene: From Prehistoric Killer to Modern NecessityYahya Al-AmeriNo ratings yet
- Orthodontic Brackets - A Review ArticleDocument10 pagesOrthodontic Brackets - A Review ArticleInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- My Clinical PaperDocument9 pagesMy Clinical PaperNazim SallamNo ratings yet
- Senate Bill 249Document8 pagesSenate Bill 249Sarah LightNo ratings yet
- FCE Test (R+L+W+GDocument20 pagesFCE Test (R+L+W+GTrần Minh ThưNo ratings yet
- Biosmart Dental Materials - A New Era in Dentistry-1Document6 pagesBiosmart Dental Materials - A New Era in Dentistry-1Kanish AggarwalNo ratings yet
- Distinguish Ʃ Ans S SoundDocument4 pagesDistinguish Ʃ Ans S SoundLoan Bùi ThanhNo ratings yet
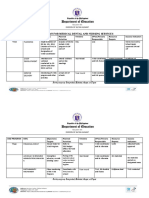
- Sample WINS Action PLanDocument3 pagesSample WINS Action PLanJEANYVIE ESPINOSANo ratings yet
- (Loga.vn) Đề thi học kì 2Document8 pages(Loga.vn) Đề thi học kì 2Hà TrangNo ratings yet
- Kim 2000Document6 pagesKim 2000hayet debbichNo ratings yet
- Skull European Wildcat: Diagram of The General of A Male Domestic CatDocument2 pagesSkull European Wildcat: Diagram of The General of A Male Domestic CatFarhan AhmedNo ratings yet
- Zirconio ImpresoDocument8 pagesZirconio ImpresoLinda Garcia PNo ratings yet
- BJMP Dental Referral FormDocument2 pagesBJMP Dental Referral FormRoyce Christian EbitNo ratings yet
- 22arun Thesis ArticleDocument8 pages22arun Thesis ArticlebhupendraNo ratings yet