You might also like
- Halitosis Journal (English)Document7 pagesHalitosis Journal (English)nicolasbriansNo ratings yet
- HALITOSISDocument6 pagesHALITOSISrashui100% (1)
- Halitosis JournalDocument9 pagesHalitosis JournalnicolasbriansNo ratings yet
- A Current Approach To Halitosis and Oral MalodorDocument9 pagesA Current Approach To Halitosis and Oral MalodorNadya PuspitaNo ratings yet
- Etiological Factors, Diagnoses, and Treatments of Halitosis: A Review UpdateDocument5 pagesEtiological Factors, Diagnoses, and Treatments of Halitosis: A Review UpdatePingkanmartjunNo ratings yet
- Constipation and Obstipation GuideDocument67 pagesConstipation and Obstipation GuideAradhanaRamchandaniNo ratings yet
- Leukoplakia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandLeukoplakia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Demin/Remin in Preventive Dentistry: Demineralization By Foods, Acids, And Bacteria, And How To Counter Using RemineralizationFrom EverandDemin/Remin in Preventive Dentistry: Demineralization By Foods, Acids, And Bacteria, And How To Counter Using RemineralizationNo ratings yet
- HalitosisDocument6 pagesHalitosispratyusha vallamNo ratings yet
- Differential Diagnosis of Tongue LesionsDocument12 pagesDifferential Diagnosis of Tongue LesionsKartikakhairaniNo ratings yet
- Question Papers For Bds Second YearDocument6 pagesQuestion Papers For Bds Second Yearsridevi sivaramakrishnanNo ratings yet
- Oral HygieneDocument13 pagesOral HygieneBilal AqeelNo ratings yet
- PsoriasisDocument4 pagesPsoriasisLau ColastreNo ratings yet
- Early Childhood Caries - A Review PDFDocument7 pagesEarly Childhood Caries - A Review PDFdr parveen bathlaNo ratings yet
- StomatitisDocument74 pagesStomatitisZahoor ZaidiNo ratings yet
- National Oral Health Policy FrameworkDocument21 pagesNational Oral Health Policy FrameworkDilipManohari Manoharidilip100% (3)
- Oral MedicineDocument136 pagesOral Medicineganang19No ratings yet
- GINGIVITISDocument43 pagesGINGIVITISRamyaNo ratings yet
- Sample ThesisDocument46 pagesSample ThesisRaj Subedi100% (1)
- Halitosis and MenopauseDocument6 pagesHalitosis and MenopausenicolasbriansNo ratings yet
- HalitosisDocument34 pagesHalitosisVinay KumarNo ratings yet
- Oral Manifestations of Nutritional Disorders2Document33 pagesOral Manifestations of Nutritional Disorders2Yeoh Wen LiNo ratings yet
- Deviated Nasal Septum: Ahmednagar Homoeopathic Medical College & Hospital AhmednagarDocument13 pagesDeviated Nasal Septum: Ahmednagar Homoeopathic Medical College & Hospital AhmednagarSuhas IngaleNo ratings yet
- Oral IrrigatorDocument30 pagesOral IrrigatorNorman Tri Kusumo100% (1)
- CSOM TreatmentDocument21 pagesCSOM TreatmentSarwinder SinghNo ratings yet
- Orofacial Infections in Children PedoDocument40 pagesOrofacial Infections in Children PedoFourthMolar.comNo ratings yet
- Vit K in Wound HealingDocument9 pagesVit K in Wound HealingRishabh KapoorNo ratings yet
- Effect of Tongue Brushing On Oral Malodor in AdolescentsDocument5 pagesEffect of Tongue Brushing On Oral Malodor in AdolescentsMarian Si Teofana HasnaNo ratings yet
- Oral Tumor / Cancer: Wirsma Arif Harahap Head Neck and Breast Oncology Consultant Andalas Medical School PadangDocument55 pagesOral Tumor / Cancer: Wirsma Arif Harahap Head Neck and Breast Oncology Consultant Andalas Medical School Padangnawal asmadiNo ratings yet
- Maxillary SinusDocument67 pagesMaxillary SinusDR. NEETI TATIYANo ratings yet
- Sialolithiasis: Vi Ugboko Fmcds FwacsDocument47 pagesSialolithiasis: Vi Ugboko Fmcds FwacsAkeem Alawode50% (2)
- Emetics and Antiemetics DrugsDocument15 pagesEmetics and Antiemetics DrugsrajenderNo ratings yet
- HalitosisDocument11 pagesHalitosisWirajulay PratiwiNo ratings yet
- Chapter 1Document38 pagesChapter 1synap5esNo ratings yet
- Diagnosis and treatment of gangrene in 40 charactersDocument3 pagesDiagnosis and treatment of gangrene in 40 charactersmksayshiNo ratings yet
- Epidemiology of Oral Cancer PDFDocument6 pagesEpidemiology of Oral Cancer PDFمحمد عبدالهادي إسماعيلNo ratings yet
- Cushing's SyndromeDocument68 pagesCushing's SyndromeKaye De Guzman, BSN - Level 3ANo ratings yet
- Hypertension in The Medically Compromised PatientDocument24 pagesHypertension in The Medically Compromised Patientapi-245611581100% (1)
- Allergic RhinitisDocument21 pagesAllergic RhinitisRahmadona NandaNo ratings yet
- Control Bleeding with Direct PressureDocument14 pagesControl Bleeding with Direct PressureRhomizal MazaliNo ratings yet
- Oral Cancer WordDocument18 pagesOral Cancer WordAdeesh saraf100% (1)
- PSM Spot Community MedicineDocument20 pagesPSM Spot Community MedicinePramila MahaleNo ratings yet
- Introduction To DentistryDocument42 pagesIntroduction To DentistryManjeev100% (2)
- Vago ThomasDocument29 pagesVago ThomasEsti Rahmawati SuryaningrumNo ratings yet
- Chemical Plaque Control PerioDocument28 pagesChemical Plaque Control PerioFourthMolar.comNo ratings yet
- Extraction of TeethDocument84 pagesExtraction of TeethAkram Thabet0% (1)
- Fluoridation - Seminar TopicDocument4 pagesFluoridation - Seminar Topicnawafaslam100% (1)
- Diseases of the Oral Cavity: Signs, Symptoms and ManagementDocument117 pagesDiseases of the Oral Cavity: Signs, Symptoms and ManagementRamanujam SridharNo ratings yet
- Rashtriya Bal Swasthya KaryakramDocument2 pagesRashtriya Bal Swasthya KaryakramNeeraj Bhargav100% (1)
- CystitisDocument2 pagesCystitisMazhar WarisNo ratings yet
- Supragingival AND Subgingival IrrigationDocument19 pagesSupragingival AND Subgingival IrrigationRituArunMathur100% (1)
- Exam Preparatory Manual of Oral Medicine and Radiology: November 2019Document13 pagesExam Preparatory Manual of Oral Medicine and Radiology: November 2019Anudnya JadhavNo ratings yet
- Oral Disease: Dental CariesDocument8 pagesOral Disease: Dental CariesAnna PruteanuNo ratings yet
- Case Presentation - GASTRODocument46 pagesCase Presentation - GASTROalidudeNo ratings yet
- Antibiotics in Dental PracticeDocument31 pagesAntibiotics in Dental PracticeSananda SahaNo ratings yet
- Culture Media in Oral PathologyDocument6 pagesCulture Media in Oral Pathologyimi4No ratings yet
- Sterlization, Disinfection and AntisepticsDocument63 pagesSterlization, Disinfection and AntisepticsMadhura ShekatkarNo ratings yet
- Social MeasuresDocument22 pagesSocial MeasuresfarhanaNo ratings yet
- StomatitisDocument44 pagesStomatitisNessa Layos Morillo100% (1)
- Preprosthetic Surgery 12-02-015Document32 pagesPreprosthetic Surgery 12-02-015Yaser JasNo ratings yet
- Antimicrobial Stewardship Program BenefitsDocument31 pagesAntimicrobial Stewardship Program BenefitsPrathusha Umakhanth100% (2)
- SA DIAGNOSTIC: SALIVA AS A POWERFUL DIAGNOSTIC TOOLDocument30 pagesSA DIAGNOSTIC: SALIVA AS A POWERFUL DIAGNOSTIC TOOLPrathusha UmakhanthNo ratings yet
- Lasers in DentistryDocument66 pagesLasers in DentistryPrathusha UmakhanthNo ratings yet
- Defense Mechanisms of Gingiva & Host Response: By, Prathusha.U CRIDocument42 pagesDefense Mechanisms of Gingiva & Host Response: By, Prathusha.U CRIPrathusha UmakhanthNo ratings yet
- Piezosurgery: By, Prathusha.U CRI Department of Public Health Dentistry Chettinad Dental CollegeDocument36 pagesPiezosurgery: By, Prathusha.U CRI Department of Public Health Dentistry Chettinad Dental CollegePrathusha Umakhanth100% (1)
- Nanotechnology in DentistryDocument38 pagesNanotechnology in DentistryPrathusha Umakhanth100% (1)
- Halitosis - Etilogy and PathogenesisDocument26 pagesHalitosis - Etilogy and PathogenesisPrathusha UmakhanthNo ratings yet
- Autoimmune Vesiculobullous LesionsDocument32 pagesAutoimmune Vesiculobullous LesionsPrathusha UmakhanthNo ratings yet
- Nanotechnology in DentistryDocument38 pagesNanotechnology in DentistryPrathusha Umakhanth100% (1)
- Lasers in DentistryDocument66 pagesLasers in DentistryPrathusha UmakhanthNo ratings yet
- Piezosurgery: By, Prathusha.U CRI Department of Public Health Dentistry Chettinad Dental CollegeDocument36 pagesPiezosurgery: By, Prathusha.U CRI Department of Public Health Dentistry Chettinad Dental CollegePrathusha Umakhanth100% (1)
- Facial Space InfectionsDocument76 pagesFacial Space InfectionsPrathusha UmakhanthNo ratings yet
- Facial Space InfectionsDocument76 pagesFacial Space InfectionsPrathusha UmakhanthNo ratings yet
- SPACE INFECTIONS OF HEAD Amp NECK - 1Document66 pagesSPACE INFECTIONS OF HEAD Amp NECK - 1Prathusha UmakhanthNo ratings yet
- Oral Medicine SeminarDocument18 pagesOral Medicine SeminarPrathusha UmakhanthNo ratings yet
- DD of Jaw LesionsDocument92 pagesDD of Jaw LesionsPrathusha UmakhanthNo ratings yet
- Magsaysay Memorial College of Zambales, IncDocument4 pagesMagsaysay Memorial College of Zambales, IncJoanne CuestaNo ratings yet
- Office Hygiene British English Upper Intermediate Advanced GroupDocument3 pagesOffice Hygiene British English Upper Intermediate Advanced GroupPablo Tejedor LópezNo ratings yet
- Health PPT 33Document26 pagesHealth PPT 33Kamlesh KumarNo ratings yet
- Cardiovascular System PharmacothDocument78 pagesCardiovascular System PharmacothKumera Dinkisa ToleraNo ratings yet
- Cost Accounting Horngren 15th Edition Test BankDocument38 pagesCost Accounting Horngren 15th Edition Test Bankmitchellunderwooda4p4d100% (16)
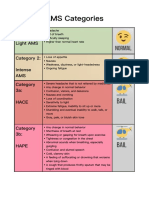
- AMS Symptoms and CategoriesDocument1 pageAMS Symptoms and CategoriesyyggvcNo ratings yet
- HIV/Syphilis StudiesDocument2 pagesHIV/Syphilis StudiesYusuf Arif SalamNo ratings yet
- Research Worksheet - Conspiracy Research PaperDocument3 pagesResearch Worksheet - Conspiracy Research PaperViktor SpauldingNo ratings yet
- Deep Vein ThrombosisDocument9 pagesDeep Vein ThrombosisitdocNo ratings yet
- Biostatistics - Part 8A - DR - Vennila JDocument22 pagesBiostatistics - Part 8A - DR - Vennila JIts AnythingNo ratings yet
- Electromyography (EMG) : By:-Aishwarya More & Pooja MishraDocument74 pagesElectromyography (EMG) : By:-Aishwarya More & Pooja MishraAisha MoreNo ratings yet
- IDSA - Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in WomenDocument7 pagesIDSA - Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in Womenamalia puspita dewiNo ratings yet
- Philosphy AssignmentDocument2 pagesPhilosphy Assignmentpang jing zheNo ratings yet
- Renal Stone Types, Causes and SymptomsDocument29 pagesRenal Stone Types, Causes and Symptomsarim100% (1)
- WHO Global Air Quality Guidelines 2021Document300 pagesWHO Global Air Quality Guidelines 2021Ermes BigattonNo ratings yet
- Feasibility and Estimated Efficacy of Blood Flow Restricted Training in Female Patients With Rheumatoid Arthritis A Randomized Controlled Pilot StudyDocument10 pagesFeasibility and Estimated Efficacy of Blood Flow Restricted Training in Female Patients With Rheumatoid Arthritis A Randomized Controlled Pilot StudyDaniel Andrés Bulla GarcíaNo ratings yet
- MPPC Health Indeminity FormDocument2 pagesMPPC Health Indeminity FormmichaelforkcsNo ratings yet
- Rush University HCQDocument24 pagesRush University HCQJuana Atkins100% (1)
- Radiobiology For The Radiologist 8th Edition Ebook PDFDocument61 pagesRadiobiology For The Radiologist 8th Edition Ebook PDFroy.mula622100% (40)
- Tuberculosis in Infancy and ChildhoodDocument39 pagesTuberculosis in Infancy and ChildhoodPediatrics SLCM-WHQMNo ratings yet
- Tiket Juragan GombalDocument3 pagesTiket Juragan Gombaldhebys suryaniNo ratings yet
- Anesthetic Consideration For Patients With Obstructive JaundiceDocument47 pagesAnesthetic Consideration For Patients With Obstructive JaundiceagatakassaNo ratings yet
- Ecg For The Exam-Score 2020Document17 pagesEcg For The Exam-Score 2020prasannasimhaNo ratings yet
- Absorb Amplify Course List (Updated Monthly)Document6 pagesAbsorb Amplify Course List (Updated Monthly)Madhu KumarNo ratings yet
- Set 5, Reumatology, ArpanaDocument14 pagesSet 5, Reumatology, ArpanaSahana hadaNo ratings yet
- A Case Study In:: Hirschsprung DiseaseDocument18 pagesA Case Study In:: Hirschsprung DiseaseJaimie La PenaNo ratings yet
- The Covi d-19 Vacci Ne, The New Li Fe Saver: A Brief IntroductionDocument3 pagesThe Covi d-19 Vacci Ne, The New Li Fe Saver: A Brief IntroductionyaraNo ratings yet
- Parkinsons Disease Rating Scales A Literature RevDocument20 pagesParkinsons Disease Rating Scales A Literature RevIna Gorodețchi-DidîcNo ratings yet
- 2019 BerryDocument15 pages2019 BerrybryaneatscamerasNo ratings yet
- Guidelines On Sports Cardiology and - ExerciseDocument80 pagesGuidelines On Sports Cardiology and - ExerciseBruno S. Homem De FariaNo ratings yet