You might also like
- Concise Definitive Review: Stress Ulcer ProphylaxisDocument11 pagesConcise Definitive Review: Stress Ulcer ProphylaxisMuhammad Umar RazaNo ratings yet
- Formulating Research Problems, Questions and HypothesesDocument39 pagesFormulating Research Problems, Questions and HypothesesanushavergheseNo ratings yet
- Michael J. Welch, Carol S. Redvanly - Handbook of RadiopharmaceuticalsDocument862 pagesMichael J. Welch, Carol S. Redvanly - Handbook of RadiopharmaceuticalsMarc RitzNo ratings yet
- Comparison of Oral Versus Intravenous Proton Pump InhibitorsDocument6 pagesComparison of Oral Versus Intravenous Proton Pump InhibitorsirsyadilfikriNo ratings yet
- CC 9312Document10 pagesCC 9312Fitrianto Dwi UtomoNo ratings yet
- The Effectiveness of Standard Single Dose Omeprazole Vs High Dosecontinuous Infusion in Highrisk Critically Ill Patients 2155 6148 1000819Document5 pagesThe Effectiveness of Standard Single Dose Omeprazole Vs High Dosecontinuous Infusion in Highrisk Critically Ill Patients 2155 6148 1000819jerryNo ratings yet
- 484 ArticleText 1393 2 10 20201115Document8 pages484 ArticleText 1393 2 10 20201115speedyz3377No ratings yet
- PRP2 8 E00624Document7 pagesPRP2 8 E00624Susana RocheNo ratings yet
- Prone Position in Management of COVID-19 Patients A CommentaryDocument3 pagesProne Position in Management of COVID-19 Patients A CommentaryJoseLuisNo ratings yet
- 10 1002@bjs5 50332Document7 pages10 1002@bjs5 50332nur hasnahNo ratings yet
- Stress Ulcer Versus Placebo - 2Document8 pagesStress Ulcer Versus Placebo - 2ayu mustikariniNo ratings yet
- Clinical Outcomes of Esophagogastroduodenoscopy In.27Document6 pagesClinical Outcomes of Esophagogastroduodenoscopy In.27Agung KaryawinaraNo ratings yet
- Guideline For Stress Ulcer Prophylaxis in The Intensive Care UnitDocument4 pagesGuideline For Stress Ulcer Prophylaxis in The Intensive Care Unitannisa edwarNo ratings yet
- Stress Ulcer Versus Placebo - 2Document8 pagesStress Ulcer Versus Placebo - 2Ayu MustikariniNo ratings yet
- Inhibidor Bomba de Protones e Infecci - NDocument10 pagesInhibidor Bomba de Protones e Infecci - NSMIBA Medicina100% (1)
- Art:10.1186/s13054 016 1252 2Document9 pagesArt:10.1186/s13054 016 1252 2IsnaNo ratings yet
- EsomeprazoleDocument7 pagesEsomeprazoleSanjay NavaleNo ratings yet
- 18 BudimirDocument8 pages18 BudimirJain KasparNo ratings yet
- Medical Doctors Practice Regarding The Upper Gastrointestinal Bleeding Management at Mohammed Salih Edris Bleeding CenterDocument7 pagesMedical Doctors Practice Regarding The Upper Gastrointestinal Bleeding Management at Mohammed Salih Edris Bleeding CenterInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 2 9882 SPDocument5 pages2 9882 SPdesak indryNo ratings yet
- Tugas RCT SenaDocument10 pagesTugas RCT SenaArfad El HabibieNo ratings yet
- Bardou Stressulcerprophylaxis Natrure Review Gastro 2015Document11 pagesBardou Stressulcerprophylaxis Natrure Review Gastro 2015nur hidayatNo ratings yet
- Nej Mo A 2303706Document11 pagesNej Mo A 2303706xivydpndNo ratings yet
- Comparison of Omeprazole and Ranitidine For Stress Ulcer ProphylaxisDocument5 pagesComparison of Omeprazole and Ranitidine For Stress Ulcer ProphylaxisAngelica Hurtado CollanteNo ratings yet
- 1212-Article Text-2279-1-10-20210313Document9 pages1212-Article Text-2279-1-10-20210313Gh RossiNo ratings yet
- Jurnal Open Closed Suction GelartiDocument9 pagesJurnal Open Closed Suction GelartiAyahe Bima MubarakaNo ratings yet
- 12 - 2015 - LT Safety and Efficacy of Imatinib in PAH - IMPRES (10) 70Document10 pages12 - 2015 - LT Safety and Efficacy of Imatinib in PAH - IMPRES (10) 70edward the iiiNo ratings yet
- Jur Nal LLLLLDocument9 pagesJur Nal LLLLLsabrina nurNo ratings yet
- Hamai2018 PDFDocument4 pagesHamai2018 PDFMelissa VegaNo ratings yet
- Traa 144Document9 pagesTraa 144RashifNo ratings yet
- The Clinical Outcomes and Predictive Factors For.24Document5 pagesThe Clinical Outcomes and Predictive Factors For.24KeziaNo ratings yet
- Khan2014 PDFDocument4 pagesKhan2014 PDFtikaNo ratings yet
- Hydrocortisone, Vitamin C, and Thiamine For The Treatment of Severe Sepsis and Septic ShockDocument10 pagesHydrocortisone, Vitamin C, and Thiamine For The Treatment of Severe Sepsis and Septic Shockmmmaw mmNo ratings yet
- GNL 10 581Document6 pagesGNL 10 581Teh NuraqilahNo ratings yet
- A Comprehensive Study of Intestinal ObstructionDocument9 pagesA Comprehensive Study of Intestinal ObstructionRoxana ElenaNo ratings yet
- Stress Ulcer, Gastritis, and Gastrointestinal Bleeding Prophylaxis in Critically Ill Pediatric Patients: A Systematic ReviewDocument9 pagesStress Ulcer, Gastritis, and Gastrointestinal Bleeding Prophylaxis in Critically Ill Pediatric Patients: A Systematic ReviewIkrima MuhdarmuhallyNo ratings yet
- 50000520210101Document7 pages50000520210101Amaliah HakimNo ratings yet
- Dorner Av ShuntDocument13 pagesDorner Av ShuntClaudia TiffanyNo ratings yet
- IJP - Volume 8 - Issue 9 - Pages 11939-11944Document6 pagesIJP - Volume 8 - Issue 9 - Pages 11939-11944A'la Nur RoyanNo ratings yet
- Ibuprofen, A Potential Cause of Acute Hemorrhagic Gastritis in Children - A Case ReportDocument4 pagesIbuprofen, A Potential Cause of Acute Hemorrhagic Gastritis in Children - A Case ReportOmegawati PramudyaNo ratings yet
- Artic GotaDocument13 pagesArtic GotaAbraham MedinaNo ratings yet
- Aggressive or Moderate Fluid Resuscitation in Acute Pancreatitis NEJMDocument12 pagesAggressive or Moderate Fluid Resuscitation in Acute Pancreatitis NEJMPedro de la RosaNo ratings yet
- Loxytocine: Alternative Therapeutique Dans Les Hemorragies Digestives Hautes Variqueuses A Antananarivo (Madagascar) ?Document7 pagesLoxytocine: Alternative Therapeutique Dans Les Hemorragies Digestives Hautes Variqueuses A Antananarivo (Madagascar) ?IJAR JOURNALNo ratings yet
- SC Compared With IV Epoetin in HD PatientsDocument6 pagesSC Compared With IV Epoetin in HD PatientsNhung NguyenNo ratings yet
- ContentServer 8Document7 pagesContentServer 8Fitra PahlevyNo ratings yet
- Transesophageal Echocardiographic Assessment in Patients With SevereDocument3 pagesTransesophageal Echocardiographic Assessment in Patients With SevereDrMarcus KeyboardNo ratings yet
- Zhao, 2021 PDFDocument10 pagesZhao, 2021 PDFiaw iawNo ratings yet
- Streptokinase Versus Unfractionated Heparin Nebu in ARDS RCT 2020Document8 pagesStreptokinase Versus Unfractionated Heparin Nebu in ARDS RCT 2020Fransisca Dewi KumalaNo ratings yet
- Bensi 2018Document10 pagesBensi 2018Karol Y. Wilson LondoñoNo ratings yet
- Eckardt Et Al.Document12 pagesEckardt Et Al.sheharyarNo ratings yet
- Effect of Antibiotic Prophylaxis On Acute Necrotizing Pancreatitis: Results of A Randomized Controlled TrialDocument7 pagesEffect of Antibiotic Prophylaxis On Acute Necrotizing Pancreatitis: Results of A Randomized Controlled TrialKirsten HartmanNo ratings yet
- Peritoneal Dialysis-Related Peritonitis Caused by Pseudomonas Species: Insight From A Post-Millennial Case SeriesDocument9 pagesPeritoneal Dialysis-Related Peritonitis Caused by Pseudomonas Species: Insight From A Post-Millennial Case SeriesDesi HutapeaNo ratings yet
- Lam 2015Document8 pagesLam 2015ferrevNo ratings yet
- Stress Ulcer Prophylaxis GuidelinesDocument9 pagesStress Ulcer Prophylaxis GuidelinesHAIDAR RACHMANNo ratings yet
- 14 - Mazandarani2012Document7 pages14 - Mazandarani2012TandeanTommyNovenantoNo ratings yet
- IJOPP - v5 - I3 - 2012 5Document7 pagesIJOPP - v5 - I3 - 2012 5Ambujesh ChaturvediNo ratings yet
- Articulo NeumologiaDocument11 pagesArticulo NeumologiaHernandoJoseViloriaSanchezNo ratings yet
- Fphar 13 1021584Document11 pagesFphar 13 1021584topanNo ratings yet
- Estudio CheetaDocument11 pagesEstudio CheetacrisordNo ratings yet
- Corticosteroid and BleedingDocument9 pagesCorticosteroid and BleedingRestu TriwulandaniNo ratings yet
- Upper Gastrointestinal Bleeding in Critically Ill Patients: Proton-Pump Inhibitors, Histamine-2 Receptor Antagonists or Placebo? Many Questions Remain UnansweredDocument4 pagesUpper Gastrointestinal Bleeding in Critically Ill Patients: Proton-Pump Inhibitors, Histamine-2 Receptor Antagonists or Placebo? Many Questions Remain UnansweredNurul Kamilah SadliNo ratings yet
- Top Trials in Gastroenterology & HepatologyFrom EverandTop Trials in Gastroenterology & HepatologyRating: 4.5 out of 5 stars4.5/5 (7)
- Tatalaksana Kad 1Document7 pagesTatalaksana Kad 1Nurul Kamilah SadliNo ratings yet
- Guideline StatinDocument7 pagesGuideline StatinNurul Kamilah SadliNo ratings yet
- Ppi-Warfarin 1Document4 pagesPpi-Warfarin 1Nurul Kamilah SadliNo ratings yet
- Inhibition and Induction of CYP Enzymes in Humans: An UpdateDocument52 pagesInhibition and Induction of CYP Enzymes in Humans: An UpdateNurul Kamilah SadliNo ratings yet
- Acute Oxaliplatin-Induced Hemolytic Anemia, Thrombocytopenia, and Renal Failure: Case Report and A Literature ReviewDocument3 pagesAcute Oxaliplatin-Induced Hemolytic Anemia, Thrombocytopenia, and Renal Failure: Case Report and A Literature ReviewNurul Kamilah SadliNo ratings yet
- Doosis KalsiumDocument8 pagesDoosis KalsiumNurul Kamilah SadliNo ratings yet
- Konversi Insulin IV-sc 2Document12 pagesKonversi Insulin IV-sc 2Nurul Kamilah SadliNo ratings yet
- Anemia Pada Diabetes New OnsetDocument6 pagesAnemia Pada Diabetes New OnsetNurul Kamilah SadliNo ratings yet
- Crp-Il6 Di KadDocument8 pagesCrp-Il6 Di KadNurul Kamilah SadliNo ratings yet
- Anti-Diabetic Effect Of Telmisartan Through Its Partial Pparγ-Agonistic ActivityDocument9 pagesAnti-Diabetic Effect Of Telmisartan Through Its Partial Pparγ-Agonistic ActivityNurul Kamilah SadliNo ratings yet
- Anemia Pada Diabetes New OnsetDocument6 pagesAnemia Pada Diabetes New OnsetNurul Kamilah SadliNo ratings yet
- Cisplatin Etoposide (Intravenous)Document7 pagesCisplatin Etoposide (Intravenous)Nurul Kamilah SadliNo ratings yet
- Guidelien RaDocument16 pagesGuidelien RaNurul Kamilah SadliNo ratings yet
- Anti KankerDocument129 pagesAnti KankerNurul Kamilah SadliNo ratings yet
- DRUG NAME: Fluorouracil: Synonym (S) : Common Trade Name: ClassificationDocument14 pagesDRUG NAME: Fluorouracil: Synonym (S) : Common Trade Name: ClassificationNurul Kamilah SadliNo ratings yet
- Regimen Kanker RektumDocument8 pagesRegimen Kanker RektumNurul Kamilah SadliNo ratings yet
- Folfox 1Document8 pagesFolfox 1Nurul Kamilah SadliNo ratings yet
- Bioequivalence Evaluation of Two Brands of EtoricoDocument7 pagesBioequivalence Evaluation of Two Brands of EtoricoNurul Kamilah SadliNo ratings yet
- FOLFOX - Oxaliplatin / Degramont: Ondansetron IV Must Be Infused Over 15 Minutes in Patients Over 65 Years of AgeDocument4 pagesFOLFOX - Oxaliplatin / Degramont: Ondansetron IV Must Be Infused Over 15 Minutes in Patients Over 65 Years of AgeNurul Kamilah SadliNo ratings yet
- Homework: 1) What Does The Respiratory System Do ?Document6 pagesHomework: 1) What Does The Respiratory System Do ?Mariana VasileNo ratings yet
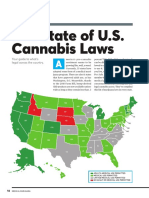
- The State of U.S. Cannabis Laws, AbridgedDocument6 pagesThe State of U.S. Cannabis Laws, AbridgedPaul Marini100% (1)
- Depram & Antidepressant Medical KnowledgeDocument85 pagesDepram & Antidepressant Medical KnowledgePeter KaiserNo ratings yet
- Who Needs Bypass SurgeryDocument70 pagesWho Needs Bypass SurgerymikikiNo ratings yet
- Daily Management PlanDocument4 pagesDaily Management PlanmirojsNo ratings yet
- BTS ILD Registry Annual Report 2021Document38 pagesBTS ILD Registry Annual Report 2021Rana Khaled AwwadNo ratings yet
- Admintrationofmedications1 Copy 181202173921Document186 pagesAdmintrationofmedications1 Copy 181202173921Karl RobleNo ratings yet
- SadsadDocument3 pagesSadsadDalo ZeronNo ratings yet
- Grant Proposal Title: Community Outreach by Dermatology Education (CODE)Document7 pagesGrant Proposal Title: Community Outreach by Dermatology Education (CODE)Darius PanganibanNo ratings yet
- ORE DrugsDocument4 pagesORE DrugsKhalid G. AzouniNo ratings yet
- PACV - Elsevier® JournalFinderDocument16 pagesPACV - Elsevier® JournalFinderJeslyn TengkawanNo ratings yet
- Female Sterilisation: Presented by Group 4Document23 pagesFemale Sterilisation: Presented by Group 4IbrahimWagesNo ratings yet
- ACLS AgorithmDocument55 pagesACLS AgorithmkpsuanNo ratings yet
- Par QDocument1 pagePar QMary Grace DeramasNo ratings yet
- Phaco / Lasik - Hands On Training in India: I Care ConsultantsDocument3 pagesPhaco / Lasik - Hands On Training in India: I Care ConsultantsicareconsultantsNo ratings yet
- Actual List Kedatangan KarantinaDocument3 pagesActual List Kedatangan KarantinaTirta BudiawanNo ratings yet
- Paracetamol Overdose: BW 40 KG Without Fluid RestrictionDocument2 pagesParacetamol Overdose: BW 40 KG Without Fluid RestrictionAndy TanNo ratings yet
- k2 Stom F EngDocument28 pagesk2 Stom F Engdmd1983aminNo ratings yet
- CMO 14 SDocument8 pagesCMO 14 SMariae PanlilioNo ratings yet
- CHN2 Module3 - 2021Document5 pagesCHN2 Module3 - 2021Nopdy JaronNo ratings yet
- Adjustment and Impulse Control DisordersDocument19 pagesAdjustment and Impulse Control DisordersArchana50% (4)
- Health Information Systems: Lesson 5Document7 pagesHealth Information Systems: Lesson 5Jennifer Ledesma-Pido100% (2)
- Reflective Writing 3Document2 pagesReflective Writing 3Luiza NiyazmetovaNo ratings yet
- Ciad 696Document10 pagesCiad 696vsjsqz97nrNo ratings yet
- Vidradhi in B Hat-Trayī A Critical Review of LiteratureDocument8 pagesVidradhi in B Hat-Trayī A Critical Review of LiteratureInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Vims-Vas Malinta 1-12-2022Document129 pagesVims-Vas Malinta 1-12-2022Julia JacoboNo ratings yet
- Glaucoma in A Moggy Cat - A Case ReportDocument5 pagesGlaucoma in A Moggy Cat - A Case ReportMukhlisa RahmanNo ratings yet
- Homeo-11 RrUBRICSDocument32 pagesHomeo-11 RrUBRICSRashid MahmoodNo ratings yet