You might also like
- Drug Cheat SheetDocument2 pagesDrug Cheat SheetKeith McDonald100% (2)
- Oet 2.0 Practice Tests Nursing - WritingDocument30 pagesOet 2.0 Practice Tests Nursing - WritingSagiraju Srinu92% (12)
- Common ICU DripsDocument1 pageCommon ICU DripsSunshine Willis100% (2)
- Top 300 Drugs Pocket Reference Guide (2021 Edition)From EverandTop 300 Drugs Pocket Reference Guide (2021 Edition)Rating: 5 out of 5 stars5/5 (1)
- Insite 2010 2018 CookbookDocument16 pagesInsite 2010 2018 CookbookBrianNo ratings yet
- Biology Project-Drugs and Alcohol AbuseDocument23 pagesBiology Project-Drugs and Alcohol AbuseDeepika78% (18)
- Stangor2 - 1 TIF Ch05Document28 pagesStangor2 - 1 TIF Ch05Chinonso AhunaNo ratings yet
- Intravenous Anaesthetics: Thiopentone Methohexitone Propofol KetamineDocument9 pagesIntravenous Anaesthetics: Thiopentone Methohexitone Propofol KetamineTomNo ratings yet
- Muscle Relaxants: Vecuronium Rocuronium Atracurium CisatracuriumDocument4 pagesMuscle Relaxants: Vecuronium Rocuronium Atracurium CisatracuriumTomNo ratings yet
- Handout 2563 OpioidsDocument84 pagesHandout 2563 OpioidsPiya TangNo ratings yet
- Summary of Common Opioids: Opioid Morphine Oxycodone Fentanyl Alfentanil Remifentanil PethidineDocument2 pagesSummary of Common Opioids: Opioid Morphine Oxycodone Fentanyl Alfentanil Remifentanil PethidineSammuel1324No ratings yet
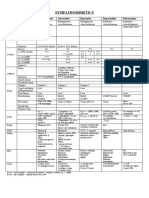
- Sympathomimetics Comparison ChartDocument4 pagesSympathomimetics Comparison ChartTomNo ratings yet
- Propofol Thiopentone Ketamine: A Comparison of Three Intravenous AnestheticsDocument38 pagesPropofol Thiopentone Ketamine: A Comparison of Three Intravenous AnestheticsenoNo ratings yet
- Managing Pain With OpioidsDocument4 pagesManaging Pain With Opioidsbab_gulNo ratings yet
- Neuromuscular BlockersDocument1 pageNeuromuscular Blockersgibsonb2No ratings yet
- Inhalation agents and anesthetic drugsDocument3 pagesInhalation agents and anesthetic drugsNicole CardenasNo ratings yet
- Pgx-Guided Dosing in Pain Management: (Group 7)Document1 pagePgx-Guided Dosing in Pain Management: (Group 7)Michelle Kristine DonnellyNo ratings yet
- Nursing Cheat SheetDocument1 pageNursing Cheat Sheetramesh kumarNo ratings yet
- Opioids MedicalDocument11 pagesOpioids MedicalduckyouisaacNo ratings yet
- NSAIDSDocument18 pagesNSAIDSduckyouisaacNo ratings yet
- Opioid Equianalgesic ChartDocument1 pageOpioid Equianalgesic Chartdamondouglas100% (7)
- Opioids in AnaesthesiaDocument28 pagesOpioids in AnaesthesiaChhabilal BastolaNo ratings yet
- Classification of InfectiousDocument3 pagesClassification of InfectiousabubakarNo ratings yet
- Sedative-Hypnotic and Antipsychotic Drugs GuideDocument17 pagesSedative-Hypnotic and Antipsychotic Drugs GuideBijay Kumar MahatoNo ratings yet
- Antiepileptic Drugs (Aed) : R. Anita. IndriyantiDocument36 pagesAntiepileptic Drugs (Aed) : R. Anita. Indriyantiandisti2323No ratings yet
- Suxamethonium Atracurium Cisatracurium Pancuronium Vecuronium RocuroniumDocument1 pageSuxamethonium Atracurium Cisatracurium Pancuronium Vecuronium Rocuroniumicen00bNo ratings yet
- PR STEPLADDER CTS AmmaliaDocument27 pagesPR STEPLADDER CTS AmmaliaAmmalia RachmiNo ratings yet
- PR Stepladder Cts AmmaliaDocument27 pagesPR Stepladder Cts AmmaliaAmmalia RachmiNo ratings yet
- Ed Adult and PaedsDocument2 pagesEd Adult and PaedsPrashin RocharamNo ratings yet
- Kuliah OpioidDocument50 pagesKuliah OpioidAndi RifkyNo ratings yet
- Drugs and Dosage Drugs and Dosage: Atropine Sulfate 1Mg/MlDocument3 pagesDrugs and Dosage Drugs and Dosage: Atropine Sulfate 1Mg/MlIna RamosNo ratings yet
- DRUGS2Document1 pageDRUGS2KaoriMarieSembranoNo ratings yet
- TOP DRUGS - Doc Version 1Document12 pagesTOP DRUGS - Doc Version 1Charme Jean RaygonNo ratings yet
- Opioid Equianalgesic Table EtcDocument2 pagesOpioid Equianalgesic Table EtcHerrera MiguelNo ratings yet
- Drugsto HAFALDocument3 pagesDrugsto HAFALThanyun YunNo ratings yet
- John MeechanDocument79 pagesJohn Meechan1dentistNo ratings yet
- Pre-Operative Orders Post-Op Orders (Ga)Document3 pagesPre-Operative Orders Post-Op Orders (Ga)Alissandra OcampoNo ratings yet
- Blood Pressure: 90/60 MM/HG To 120/80 MM/HG Breathing: 16 To 24 Breaths Per Minute Pulse: 60 To 100 Beats Per Minute Temperature: 97.8°F To 99.1°F (36.5°C To 37.5°C)Document11 pagesBlood Pressure: 90/60 MM/HG To 120/80 MM/HG Breathing: 16 To 24 Breaths Per Minute Pulse: 60 To 100 Beats Per Minute Temperature: 97.8°F To 99.1°F (36.5°C To 37.5°C)Ahmed AlkhaqaniNo ratings yet
- Alkaline Phosphatase, Liquid Package InsertDocument2 pagesAlkaline Phosphatase, Liquid Package InsertMonik MonikaNo ratings yet
- Top DrugsDocument12 pagesTop DrugsStephanie Villanueva AdvinculaNo ratings yet
- Vital signs and therapeutic drug levels reference guideDocument4 pagesVital signs and therapeutic drug levels reference guidePanJan BalNo ratings yet
- Guidelines For Nurse Controlled and Patient Controlled Analgesia Morphine InfusionDocument2 pagesGuidelines For Nurse Controlled and Patient Controlled Analgesia Morphine Infusionfinchan IrawanNo ratings yet
- PrescribingDocument2 pagesPrescribingPei Xing KwekNo ratings yet
- LA GeneralDocument2 pagesLA GeneralNicole CardenasNo ratings yet
- Agents Used in Musculoskeletal Disorders FajarDocument136 pagesAgents Used in Musculoskeletal Disorders Fajarilham maulanaNo ratings yet
- Republic of The PhilippinesDocument5 pagesRepublic of The Philippinesjonacris08No ratings yet
- Sedatives & HypnoticsDocument49 pagesSedatives & HypnoticsShubha DiwakarNo ratings yet
- Routine Anesthesia Set UpDocument4 pagesRoutine Anesthesia Set UpSteve Johnstone100% (2)
- Farmakologi Obat Obesitas Dislipidemia 2022Document57 pagesFarmakologi Obat Obesitas Dislipidemia 2022Meidy PratiwiNo ratings yet
- Spinal Cord CompressionDocument4 pagesSpinal Cord Compressionian3yeung-2No ratings yet
- Anti-Epileptic DrugsDocument2 pagesAnti-Epileptic DrugsKaoriMarieSembranoNo ratings yet
- CVP Plus Rituximab (R-CVP) For Lymphoma: Page 1 of 2Document2 pagesCVP Plus Rituximab (R-CVP) For Lymphoma: Page 1 of 2Andreea NeculceaNo ratings yet
- Anaesthetic Drugs Cheat SheetsDocument2 pagesAnaesthetic Drugs Cheat SheetsPkern100% (3)
- PICU Drug Handbook 2014 PDFDocument106 pagesPICU Drug Handbook 2014 PDFMelissa SantosoNo ratings yet
- Psychoactive and AntibioticsDocument2 pagesPsychoactive and AntibioticsKaoriMarieSembranoNo ratings yet
- Protokol RcheopDocument3 pagesProtokol RcheopYudha RozyNo ratings yet
- Epilepsy Is Due To Sudden, Excessive Depolarization Of: Some or All Cerebral NeuronsDocument19 pagesEpilepsy Is Due To Sudden, Excessive Depolarization Of: Some or All Cerebral NeuronsMourian AmanNo ratings yet
- Dr. Ranjan's Hundred Drug and Disease SeriesDocument102 pagesDr. Ranjan's Hundred Drug and Disease SeriesRohan GhoshNo ratings yet
- Ccu Guideline Nicvd-1Document9 pagesCcu Guideline Nicvd-1Farhan AnikNo ratings yet
- MetabolismDocument15 pagesMetabolismnadila oktaviaNo ratings yet
- QR Klinik Kesihatan Setting, by DR Gerard Loh DMDocument34 pagesQR Klinik Kesihatan Setting, by DR Gerard Loh DMlailatul husnaNo ratings yet
- Station 3 LeafletDocument5 pagesStation 3 LeafletFelicianna Ashwinie StanleyNo ratings yet
- Weekly Report #12Document3 pagesWeekly Report #12natysha villarrubiaNo ratings yet
- Stimulant DrugsDocument2 pagesStimulant DrugsRicardo Abelidas Baluat Jr.No ratings yet
- Research Proposal On: "Bad Impacts of Drug Addiction On Youth, Economy and Society"Document17 pagesResearch Proposal On: "Bad Impacts of Drug Addiction On Youth, Economy and Society"Umme Rukaiya Mitu100% (4)
- Licensure Exams Criminologist ReviewDocument34 pagesLicensure Exams Criminologist ReviewKulot SisonNo ratings yet
- Drug Education and Vice Control MidtermDocument77 pagesDrug Education and Vice Control MidtermJARA, Joan M.No ratings yet
- 2 DdaDocument38 pages2 DdaEdd Monzon Delamide100% (1)
- Case Presentation On CannabisDocument85 pagesCase Presentation On CannabisKisna BhurtelNo ratings yet
- LESSON 4-Risky Behaviors of AdolecentsDocument8 pagesLESSON 4-Risky Behaviors of AdolecentsMary CaputeroNo ratings yet
- Opium - Poppy Cultivation, Morphine and Heroin ManufactureDocument11 pagesOpium - Poppy Cultivation, Morphine and Heroin Manufactureskalpsolo75% (4)
- ASSIGNMENT Drug AbuseDocument28 pagesASSIGNMENT Drug Abuseknj210110318No ratings yet
- Drug & Toxin List SR5Document11 pagesDrug & Toxin List SR5maszerkNo ratings yet
- Study of Women Drug UsersDocument177 pagesStudy of Women Drug UsersIrfan AhmadNo ratings yet
- CHOICES Acronym LeukoencephalopathyDocument15 pagesCHOICES Acronym LeukoencephalopathyLucas MontanhaNo ratings yet
- Drugs: Understanding the Facts, Benefits, and RisksDocument6 pagesDrugs: Understanding the Facts, Benefits, and RisksSamiNo ratings yet
- A Brief History of DrugsDocument11 pagesA Brief History of Drugsmarjorie_usi60% (5)
- TCP AlcoholicDocument13 pagesTCP AlcoholicTracey MarieNo ratings yet
- Substance-Related Disorders: Ms. Jocelyn Alcera Nazario, RN MANDocument149 pagesSubstance-Related Disorders: Ms. Jocelyn Alcera Nazario, RN MAN102680No ratings yet
- The Impact of Drug Abuse On Society A Review On Drug Abuse in The Context of SocietyDocument3 pagesThe Impact of Drug Abuse On Society A Review On Drug Abuse in The Context of SocietyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Drug Metabolism and AnalysisDocument84 pagesDrug Metabolism and AnalysisJed Santos ViernesNo ratings yet
- 2019 Aiken County Accidental OverdosesDocument1 page2019 Aiken County Accidental OverdosesJeremy TurnageNo ratings yet
- The History of Drug Laws in The United StatesDocument6 pagesThe History of Drug Laws in The United StatesAnonymous VdMiv3W9DNo ratings yet
- Appendix1 MorphineDocument75 pagesAppendix1 Morphine민규강No ratings yet
- Reading Module 2023Document29 pagesReading Module 2023Badrut Tamam Hikmawan Fauzi (Tamam)No ratings yet
- Drug SlangDocument59 pagesDrug SlangΕγώ ΕίμαιNo ratings yet
- 2023.07.25 - Knox County Forensic Center 2022 Reports Released (DRD Report)Document36 pages2023.07.25 - Knox County Forensic Center 2022 Reports Released (DRD Report)WVLT NewsNo ratings yet
- History of Addictions: J Epidemiol Community HealthDocument5 pagesHistory of Addictions: J Epidemiol Community HealthMel LissaNo ratings yet
- Forensic Medicine Day 2Document28 pagesForensic Medicine Day 2skNo ratings yet