You might also like
- Clinical Manifestation, DiagnosisDocument13 pagesClinical Manifestation, DiagnosisGeorgiana BlagociNo ratings yet
- International Journal of Antimicrobial AgentsDocument9 pagesInternational Journal of Antimicrobial AgentsautomationenggNo ratings yet
- Nutrients: The Antiviral, Anti-Inflammatory E Medicinal Herbs and Mushrooms and Sars-Cov-2 InfectionDocument13 pagesNutrients: The Antiviral, Anti-Inflammatory E Medicinal Herbs and Mushrooms and Sars-Cov-2 Infectionmmbire@gmail.comNo ratings yet
- A Comprehensive Summary of The Knowledge On COVID-19 TreatmentDocument37 pagesA Comprehensive Summary of The Knowledge On COVID-19 TreatmentChawki MokademNo ratings yet
- Covid19 An Overview of Diagnostic Approach and Novel Directions For Treatment StrategiesDocument4 pagesCovid19 An Overview of Diagnostic Approach and Novel Directions For Treatment StrategiesMarie Kath LeenNo ratings yet
- Innate and Adaptive Immune Responses Against CoronavirusDocument17 pagesInnate and Adaptive Immune Responses Against CoronavirusHARDITA SALSABILA FORTUNA HARDITA SALSABILA FORTUNANo ratings yet
- Novel SARS CoV 2 Outbreak and COVID19 Disease A Systemic Re 2020 Genes DiDocument11 pagesNovel SARS CoV 2 Outbreak and COVID19 Disease A Systemic Re 2020 Genes DiVidit DixitNo ratings yet
- Background of The Problem: Sarbecovirus, OrthocoronavirinaeDocument16 pagesBackground of The Problem: Sarbecovirus, Orthocoronavirinaesamiza1122No ratings yet
- Decoding Covid-19 With The Sars-Cov-2 GenomeDocument12 pagesDecoding Covid-19 With The Sars-Cov-2 GenomemmNo ratings yet
- PIIS0168827820336758Document17 pagesPIIS0168827820336758Yusup AhmadiNo ratings yet
- Zhou2020 Article CoronavirusDisease2019COVID-19 PDFDocument10 pagesZhou2020 Article CoronavirusDisease2019COVID-19 PDFElena AlexandraNo ratings yet
- Review of Related LiteratureDocument10 pagesReview of Related LiteratureRegine Mae EncinadaNo ratings yet
- Revision de Sdra en CovidDocument14 pagesRevision de Sdra en CovidRociio HernandezNo ratings yet
- Journal Pre-Proof: Transfusion Medicine ReviewsDocument21 pagesJournal Pre-Proof: Transfusion Medicine ReviewstaryumanNo ratings yet
- When A Life Is SpreadingDocument5 pagesWhen A Life Is SpreadingSuhail ShamseeNo ratings yet
- TRADUCCION (1) 1 - The COVID-19 Epidemic PDFDocument3 pagesTRADUCCION (1) 1 - The COVID-19 Epidemic PDFSikamelNo ratings yet
- Factors Affecting SARS CoV 2 (COVID-19) PandemicDocument32 pagesFactors Affecting SARS CoV 2 (COVID-19) PandemicTahir AliNo ratings yet
- Remdesivir For Severe Acute Respiratory Syndrome Coronavirus 2 Causing Covid 19 An Evaluation of The Evidence Yu Chen Cao All ChapterDocument53 pagesRemdesivir For Severe Acute Respiratory Syndrome Coronavirus 2 Causing Covid 19 An Evaluation of The Evidence Yu Chen Cao All Chapterdora.morales550100% (13)
- Covid 19Document22 pagesCovid 19imad khanNo ratings yet
- Joim 13091Document15 pagesJoim 13091sarabisimonaNo ratings yet
- Ebook Remdesivir For Severe Acute Respiratory Syndrome Coronavirus 2 Causing Covid 19 An Evaluation of The Evidence PDF Full Chapter PDFDocument63 pagesEbook Remdesivir For Severe Acute Respiratory Syndrome Coronavirus 2 Causing Covid 19 An Evaluation of The Evidence PDF Full Chapter PDFcarol.thompson605100% (20)
- Recent Trends and Treatment Approach in COVID-19-A Short ReviewDocument5 pagesRecent Trends and Treatment Approach in COVID-19-A Short ReviewNistara Singh ChawlaNo ratings yet
- Dendritic Cells in COVID 19 Immunopathogenesis Insights For A Possible Role in Determining Disease OutcomeDocument19 pagesDendritic Cells in COVID 19 Immunopathogenesis Insights For A Possible Role in Determining Disease OutcomeRoberto SoehartonoNo ratings yet
- A Review of The 2019 Novel Coronavirus Covid 19 Based On Current Evidence Li Sheng Wang Download 2024 Full ChapterDocument47 pagesA Review of The 2019 Novel Coronavirus Covid 19 Based On Current Evidence Li Sheng Wang Download 2024 Full Chaptermary.greenwood437100% (9)
- Covide 19 BeginigDocument14 pagesCovide 19 BeginigHamza MehalliNo ratings yet
- Journal of AutoimmunityDocument16 pagesJournal of AutoimmunityErin JohnsonNo ratings yet
- 10-23 Sero-Prevalence of Sarscov-2 Specific AntibodiesDocument14 pages10-23 Sero-Prevalence of Sarscov-2 Specific AntibodiesNeha KazmiNo ratings yet
- The Modelling of COVID19 Pathways Sheds Light On Mechanisms, Opportunities and On Controversial Interpretations of Medical Treatments. v2Document15 pagesThe Modelling of COVID19 Pathways Sheds Light On Mechanisms, Opportunities and On Controversial Interpretations of Medical Treatments. v2ballechaseNo ratings yet
- COVID-19 and Multi-Organ ResponseDocument31 pagesCOVID-19 and Multi-Organ ResponseArbaz SultanNo ratings yet
- Immune Responses in COVID-19 and Potential Vaccines: Lessons Learned From SARS and MERS EpidemicDocument9 pagesImmune Responses in COVID-19 and Potential Vaccines: Lessons Learned From SARS and MERS EpidemicCucumber IsHealthy96No ratings yet
- Features, Evaluation and Treatment Coronavirus (COVID-19)Document19 pagesFeatures, Evaluation and Treatment Coronavirus (COVID-19)Prem Shankar GuptaNo ratings yet
- A Review of Sars-Cov-2 and The Ongoing Clinical Trials: Molecular SciencesDocument19 pagesA Review of Sars-Cov-2 and The Ongoing Clinical Trials: Molecular SciencesJoseGarciaNo ratings yet
- Immune Responses in COVID-19 and Potential Vaccines: Lessons Learned From SARS and MERS EpidemicDocument9 pagesImmune Responses in COVID-19 and Potential Vaccines: Lessons Learned From SARS and MERS EpidemicJC XDNo ratings yet
- Review Article COVID-19 Infection in The Human Reproductive Tract of Men and Nonpregnant WomenDocument12 pagesReview Article COVID-19 Infection in The Human Reproductive Tract of Men and Nonpregnant WomenAISHWARYA SYNo ratings yet
- Journal Pre-Proof: Trends in ImmunologyDocument34 pagesJournal Pre-Proof: Trends in ImmunologyIntan AyuNo ratings yet
- The Genetic Sequence, Origin, and Diagnosis of Sars-Cov-2Document7 pagesThe Genetic Sequence, Origin, and Diagnosis of Sars-Cov-2iq_dianaNo ratings yet
- BiomedPap - Bio 202003 0001Document9 pagesBiomedPap - Bio 202003 0001Edison Chiriboga OrtegaNo ratings yet
- COVID-19 Infection: Origin, Transmission, and Characteristics of Human CoronavirusesDocument10 pagesCOVID-19 Infection: Origin, Transmission, and Characteristics of Human CoronavirusesVeronicaNo ratings yet
- IPIntJComprAdvPharmacol 5-2-49 57Document9 pagesIPIntJComprAdvPharmacol 5-2-49 57jmakbar AkbarNo ratings yet
- Covid 19 A Dreaded Pandemic DiseaseDocument6 pagesCovid 19 A Dreaded Pandemic DiseasegygyNo ratings yet
- 3985-Article Text-11543-1-10-20200510Document12 pages3985-Article Text-11543-1-10-20200510Dr. Nilesh JainNo ratings yet
- Therapeutic Approaches Against Coronaviruses Acute Respiratory SyndromeDocument21 pagesTherapeutic Approaches Against Coronaviruses Acute Respiratory Syndromenow youloseNo ratings yet
- (2020) Ozone (O3) and SARS-CoV-2 - Physiological Bases and Their Therapeutic Possibilities According To COVID-19 Evolutionary StageDocument9 pages(2020) Ozone (O3) and SARS-CoV-2 - Physiological Bases and Their Therapeutic Possibilities According To COVID-19 Evolutionary StageVu TranNo ratings yet
- Travel Medicine and Infectious Disease: ReviewDocument10 pagesTravel Medicine and Infectious Disease: Reviewimamsantos1191No ratings yet
- Coronavirus (COVID-19) : A Review of Clinical Features, Diagnosis, and TreatmentDocument7 pagesCoronavirus (COVID-19) : A Review of Clinical Features, Diagnosis, and TreatmentsumargoNo ratings yet
- Coronavirus WordDocument9 pagesCoronavirus WordYencygarcia RiosNo ratings yet
- 2005 ArtiDocument8 pages2005 ArtiasdjjjjssNo ratings yet
- Jurnal Kesmas Jumal HusniDocument9 pagesJurnal Kesmas Jumal HusniHumam_Aziz_2281No ratings yet
- Article Origin Transmission Characterist COVID PDFDocument8 pagesArticle Origin Transmission Characterist COVID PDFAlexRázuriNo ratings yet
- Coronavirus Disease 2019 (COVID-19) - UpToDateDocument43 pagesCoronavirus Disease 2019 (COVID-19) - UpToDateGloria MiramontesNo ratings yet
- Covid 19 Epidemiology Evolution and Cross Disciplinary Perspectives Jiumeng Sun Download 2024 Full ChapterDocument35 pagesCovid 19 Epidemiology Evolution and Cross Disciplinary Perspectives Jiumeng Sun Download 2024 Full Chaptercynthia.vaughn759100% (12)
- Vol 28 4 2020 2Document6 pagesVol 28 4 2020 2Anton LiusNo ratings yet
- Can We Cure The Coronavirus Disease 19 (COVID19) by Using Rhus Coriaria (Sumac) ExtractDocument7 pagesCan We Cure The Coronavirus Disease 19 (COVID19) by Using Rhus Coriaria (Sumac) ExtractInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- An Overview On Severe Acute Respiratory Syndrome (SARS) : D.S.C. HuiDocument9 pagesAn Overview On Severe Acute Respiratory Syndrome (SARS) : D.S.C. HuiAmerMahmutbegovicNo ratings yet
- McIntosh 2020Document48 pagesMcIntosh 2020Kenia FrnNo ratings yet
- Journal of Advanced Research: Muhammad Adnan Shereen, Suliman Khan, Abeer Kazmi, Nadia Bashir, Rabeea SiddiqueDocument8 pagesJournal of Advanced Research: Muhammad Adnan Shereen, Suliman Khan, Abeer Kazmi, Nadia Bashir, Rabeea SiddiqueAnmol YadavNo ratings yet
- Covid19 PDFDocument40 pagesCovid19 PDFMan Hong SoNo ratings yet
- Articulo 2 PedroDocument18 pagesArticulo 2 Pedroomar pascualNo ratings yet
- 1 s2.0 S2090123220300540 MainDocument8 pages1 s2.0 S2090123220300540 MainFebria Rike ErlianaNo ratings yet
- The Challenge of Defining WellbeingDocument15 pagesThe Challenge of Defining WellbeingIkmah FauzanNo ratings yet
- Heart Failure in The Last Year: Progress and Perspective: Journal ReadingDocument31 pagesHeart Failure in The Last Year: Progress and Perspective: Journal ReadingIkmah FauzanNo ratings yet
- 1 2 2018 Lens Induced Glaucoma Bhuvan PDFDocument50 pages1 2 2018 Lens Induced Glaucoma Bhuvan PDFDara AprillyantiNo ratings yet
- COVID-19 Early Warning Score: A Multi-Parameter Screening Tool To Identify Highly Suspected PatientsDocument22 pagesCOVID-19 Early Warning Score: A Multi-Parameter Screening Tool To Identify Highly Suspected PatientsIkmah FauzanNo ratings yet
- WHO COVID 19 LPC - DBMGMT 2020.1 EngDocument6 pagesWHO COVID 19 LPC - DBMGMT 2020.1 EngANWARONo ratings yet
- Vascular Emergencies in Neuro-OphthalmologyDocument10 pagesVascular Emergencies in Neuro-OphthalmologyIkmah FauzanNo ratings yet
- Heart Failure in The Last Year: Progress and Perspective: Journal ReadingDocument31 pagesHeart Failure in The Last Year: Progress and Perspective: Journal ReadingIkmah FauzanNo ratings yet
- Peds 2010-0309 FullDocument11 pagesPeds 2010-0309 FullIkmah FauzanNo ratings yet
- REFERAT 1-S2.0-S1201971210023684-MainDocument14 pagesREFERAT 1-S2.0-S1201971210023684-MainVantyNo ratings yet
- Ecertificate - Dr. - Ikmah - PesertaDocument1 pageEcertificate - Dr. - Ikmah - PesertaIkmah FauzanNo ratings yet
- AlgorithmBLS Adult CACOVID 200406 PDFDocument1 pageAlgorithmBLS Adult CACOVID 200406 PDFBalamuruganNo ratings yet
- Mental Health and Psychosocial Considerations During The COVID-19 OutbreakDocument6 pagesMental Health and Psychosocial Considerations During The COVID-19 OutbreakAndrianiNo ratings yet
- MainDocument13 pagesMainIkmah FauzanNo ratings yet
- Returning To Physical Activity After Covid-19: Practice PointerDocument6 pagesReturning To Physical Activity After Covid-19: Practice PointerIkmah FauzanNo ratings yet
- COVID-19 Early Warning Score: A Multi-Parameter Screening Tool To Identify Highly Suspected PatientsDocument22 pagesCOVID-19 Early Warning Score: A Multi-Parameter Screening Tool To Identify Highly Suspected PatientsIkmah FauzanNo ratings yet
- Edit Virtual HR Managing Dyslipidemia in Special PopulationDocument38 pagesEdit Virtual HR Managing Dyslipidemia in Special PopulationIkmah FauzanNo ratings yet
- 1118 Electrical Injuries EMPDocument20 pages1118 Electrical Injuries EMPAbog Luis Guillermo Andrade FloresNo ratings yet
- Burn Practice GuidelineDocument20 pagesBurn Practice GuidelineRay Martínez100% (1)
- Airborne Sars Cov-2Document8 pagesAirborne Sars Cov-2Ikmah FauzanNo ratings yet
- Certificate of Participation: Ikmah Fauzan, S.Ked ParticipantDocument1 pageCertificate of Participation: Ikmah Fauzan, S.Ked ParticipantIkmah FauzanNo ratings yet
- Handbook: For Clinical Management of DengueDocument124 pagesHandbook: For Clinical Management of DengueraattaiNo ratings yet
- Nuclear CardiologyDocument36 pagesNuclear CardiologyZilga ReginaNo ratings yet
- New TNM Lung CancerDocument4 pagesNew TNM Lung CancerIkmah FauzanNo ratings yet
- Pamphlet AmoebiasisDocument3 pagesPamphlet AmoebiasisAristotel Cabais100% (1)
- Covid 19Document9 pagesCovid 19XA18 Pankti Kamlesh PatelNo ratings yet
- Dengue Fever Textbook DiscussionDocument2 pagesDengue Fever Textbook DiscussionKeyyth OirelNo ratings yet
- Measles MorbiliDocument16 pagesMeasles MorbiliRegyna SusantiNo ratings yet
- Chapter 4 Social Pharmacy Introduction To Microbiology and Common NoteskartsDocument6 pagesChapter 4 Social Pharmacy Introduction To Microbiology and Common NoteskartsSushovan AshNo ratings yet
- Actinic CheilitisDocument12 pagesActinic CheilitisCathy Guerrero100% (1)
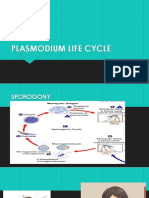
- Plasmodium Life CycleDocument7 pagesPlasmodium Life CyclePrince Robert ChuaNo ratings yet
- Tanauan City Integrated High School Trapiche 1, Tanauan City, Batangas Health Declaration FormDocument4 pagesTanauan City Integrated High School Trapiche 1, Tanauan City, Batangas Health Declaration FormKurt VillaNo ratings yet
- Black DeathDocument6 pagesBlack Deathapi-237394422No ratings yet
- Book 1Document18 pagesBook 1Rakesh SharmaNo ratings yet
- Dr. Tahira Gul: House Officer Medicine Unit IiDocument19 pagesDr. Tahira Gul: House Officer Medicine Unit IishravaniNo ratings yet
- Correspondence: Enteric Involvement in Hospitalised Patients With COVID-19 Outside WuhanDocument2 pagesCorrespondence: Enteric Involvement in Hospitalised Patients With COVID-19 Outside WuhanSeri Agustin SartikaNo ratings yet
- Draft Articel KKN Agatha Dwi Natasya RevDocument8 pagesDraft Articel KKN Agatha Dwi Natasya RevAgatha Dwi NatasyaNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormBest JiratipNo ratings yet
- DBQ 3Document6 pagesDBQ 3api-448501859No ratings yet
- Brain InfectionDocument61 pagesBrain Infectionmanisha paikarayNo ratings yet
- DVM 8th Assignment PSci-602Document3 pagesDVM 8th Assignment PSci-602pinnn poooNo ratings yet
- ICD 10 Isolation CodesDocument4 pagesICD 10 Isolation CodesShuaib KauchaliNo ratings yet
- F2 Chapter 4 Human HealthDocument6 pagesF2 Chapter 4 Human HealthJue Hazea GoldshopNo ratings yet
- Pex 11Document4 pagesPex 11shennie anteNo ratings yet
- English-6-Q2-Module-1-Lesson-2-Palpallatoc - Lydia E. - FINALDocument15 pagesEnglish-6-Q2-Module-1-Lesson-2-Palpallatoc - Lydia E. - FINALDanielLarryAquinoNo ratings yet
- Amtrak Vaccine MandateDocument2 pagesAmtrak Vaccine MandateAnna SaundersNo ratings yet
- Mycoplasma GenitaliumDocument2 pagesMycoplasma Genitaliumanurag shrivastavaNo ratings yet
- Pathology Test Performed: Assay InterpretationDocument1 pagePathology Test Performed: Assay InterpretationjyzrNo ratings yet
- Principles of Antibiotic Formulary Selection For P&T Committees 1Document3 pagesPrinciples of Antibiotic Formulary Selection For P&T Committees 1madengNo ratings yet
- DiseasesDocument3 pagesDiseasesBarani KingNo ratings yet
- Giardiasis - Causes, Symptoms, and TreatmentDocument9 pagesGiardiasis - Causes, Symptoms, and TreatmentEmproNo ratings yet
- ACG Clinical Guideline Diagnosis, Treatment, And.14Document21 pagesACG Clinical Guideline Diagnosis, Treatment, And.14Jeremy A H.L.No ratings yet
- What Is TonsillitisDocument4 pagesWhat Is TonsillitisAn NukmanNo ratings yet
- Chapter 5 Antifungal DrugsDocument55 pagesChapter 5 Antifungal DrugsAssssssNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (24)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (80)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)