You might also like
- COVID-19 and Pregnancy: An Umbrella Review of Clinical Presentation, Vertical Transmission, and Maternal and Perinatal OutcomesDocument27 pagesCOVID-19 and Pregnancy: An Umbrella Review of Clinical Presentation, Vertical Transmission, and Maternal and Perinatal OutcomesFauzi AhmadNo ratings yet
- Coronavirus Disease 2019 COVID 19 and Pregnancy A Systematic ReviewDocument5 pagesCoronavirus Disease 2019 COVID 19 and Pregnancy A Systematic ReviewFerika RafarisNo ratings yet
- 10 1111@aogs 13867 PDFDocument19 pages10 1111@aogs 13867 PDFbrenda elielNo ratings yet
- Coronavirus in Pregnancy and Delivery Rapid ReviewDocument16 pagesCoronavirus in Pregnancy and Delivery Rapid Reviewluisemisasc1990No ratings yet
- A Systematic Review and Meta Analysis of Children With Coronavirus Disease 2019 (COVID 19)Document13 pagesA Systematic Review and Meta Analysis of Children With Coronavirus Disease 2019 (COVID 19)Jevera JoshuaNo ratings yet
- Clinical Characteristics and Diagnostic Challenges of Pediatric COVID-19: A Systematic Review and Meta-AnalysisDocument8 pagesClinical Characteristics and Diagnostic Challenges of Pediatric COVID-19: A Systematic Review and Meta-AnalysisArina Al-KhaqNo ratings yet
- 30182-Article Text-56587-1-10-20211025Document8 pages30182-Article Text-56587-1-10-20211025hamdi.mus.mh10No ratings yet
- Jogcr v7n1p1 enDocument6 pagesJogcr v7n1p1 enRony TambaNo ratings yet
- IJCRT22A6345Document7 pagesIJCRT22A6345cedricyannezNo ratings yet
- Correlation Between Pregnancy Status and Severe Corona-Virus Disease Characterized by Cytokine Storm: Systematic Review and Meta-AnalysisDocument30 pagesCorrelation Between Pregnancy Status and Severe Corona-Virus Disease Characterized by Cytokine Storm: Systematic Review and Meta-Analysismila anasantiNo ratings yet
- Covid 19 Prematur Meta AnalisisDocument17 pagesCovid 19 Prematur Meta AnalisisRian AmertaNo ratings yet
- Systematic Review On Inflammatory Bowel Disease Patients With Coronavirus Disease 2019Document13 pagesSystematic Review On Inflammatory Bowel Disease Patients With Coronavirus Disease 2019Ali SheikhNo ratings yet
- Acceptance of A COVID 19 Vaccine and Associated Factors Among Pregnant Women in China A Multi Center Cross Sectional Study Based On Health BeliefDocument12 pagesAcceptance of A COVID 19 Vaccine and Associated Factors Among Pregnant Women in China A Multi Center Cross Sectional Study Based On Health BeliefamalliaNo ratings yet
- 1 s2.0 S1201971221000230 MainDocument12 pages1 s2.0 S1201971221000230 Mainoluwaseunajala404No ratings yet
- IndianJObstetGynecolRes 9 1 35 41Document7 pagesIndianJObstetGynecolRes 9 1 35 41AliyaNo ratings yet
- CALL Score PCP V1Document10 pagesCALL Score PCP V1Jose Emmanuel FranciaNo ratings yet
- Comorbidityand COVID19 in Children PPJDec 2020Document10 pagesComorbidityand COVID19 in Children PPJDec 2020Soraya RezekiNo ratings yet
- Ahead of Print: Establishment of Diagnostic Protocols For COVID-19 PatientsDocument6 pagesAhead of Print: Establishment of Diagnostic Protocols For COVID-19 PatientsSana AbbasNo ratings yet
- 1 s2.0 S0300571222003098 MainDocument8 pages1 s2.0 S0300571222003098 MainRizki Yuli amandaNo ratings yet
- PIIS2589537020301772Document19 pagesPIIS2589537020301772cendyjulianaNo ratings yet
- COVID-19 in Pregnancy - 020522Document53 pagesCOVID-19 in Pregnancy - 020522Rika FatmadonaNo ratings yet
- 1 s2.0 S2468784722000587 MainDocument6 pages1 s2.0 S2468784722000587 Mainabatasa jahahoNo ratings yet
- COVID-19 and Pregnancy: A Review of Clinical Characteristics, Obstetric Outcomes and Vertical TransmissionDocument20 pagesCOVID-19 and Pregnancy: A Review of Clinical Characteristics, Obstetric Outcomes and Vertical TransmissionDra Sandra VèlezNo ratings yet
- Mortality and Morbidity Among Pregnant Women With COVID-19 Infection: A Meta-AnalysisDocument9 pagesMortality and Morbidity Among Pregnant Women With COVID-19 Infection: A Meta-AnalysisIJPHSNo ratings yet
- Czab 133Document9 pagesCzab 1337 MNTNo ratings yet
- Clinical Characteristics of COVID-19 Infection in New-Borns and Pediatrics: A Systematic ReviewDocument8 pagesClinical Characteristics of COVID-19 Infection in New-Borns and Pediatrics: A Systematic ReviewFarida MurtianiNo ratings yet
- Clinical Characteristic Covid ChildrenDocument8 pagesClinical Characteristic Covid ChildrenEstirahayuNo ratings yet
- Correlation of Demographic Profile With Laboratory Parameters and Clinical Factors As Predictors of Covid-19 Severity: A Comprehensive AnalysisDocument7 pagesCorrelation of Demographic Profile With Laboratory Parameters and Clinical Factors As Predictors of Covid-19 Severity: A Comprehensive Analysisindex PubNo ratings yet
- 10.5811@westjem.2020.6.47919 (2) 81105Document7 pages10.5811@westjem.2020.6.47919 (2) 81105Giovan GaulNo ratings yet
- Journal Pre-Proof: International Journal of Infectious DiseasesDocument14 pagesJournal Pre-Proof: International Journal of Infectious DiseasesKenya EspinozaNo ratings yet
- PH JournalDocument7 pagesPH JournalnabilahNo ratings yet
- Awareness and Attitude of Undergraduate Medical Students Towards 2019-Novel Coronavirus in A Local Pakistani Medical CollegeDocument13 pagesAwareness and Attitude of Undergraduate Medical Students Towards 2019-Novel Coronavirus in A Local Pakistani Medical CollegeImtiaz BashirNo ratings yet
- Antenatal Care During The COVID-19 Pandemic: Original Research ArticleDocument5 pagesAntenatal Care During The COVID-19 Pandemic: Original Research ArticleAita Utsukushi HyuugaNo ratings yet
- Privateroom JournalDocument5 pagesPrivateroom JournalNathaniel PulidoNo ratings yet
- JMRH - Volume 9 - Issue 4 - Pages 2883-2891Document9 pagesJMRH - Volume 9 - Issue 4 - Pages 2883-2891Chellyani Chantika DamayantiNo ratings yet
- mm7239 HDocument30 pagesmm7239 Hchigozieatuanye66No ratings yet
- COVID 19 en UCIP Paises de Recursos Limitados. DR Carcillo. Pediatric Research 2020 Muy BuenaDocument12 pagesCOVID 19 en UCIP Paises de Recursos Limitados. DR Carcillo. Pediatric Research 2020 Muy BuenaDark LouNo ratings yet
- 2020 08 03 20167361v1 FullDocument28 pages2020 08 03 20167361v1 FullNovel SaputraNo ratings yet
- Research Article: Machine Learning-Based Model To Predict The Disease Severity and Outcome in COVID-19 PatientsDocument10 pagesResearch Article: Machine Learning-Based Model To Predict The Disease Severity and Outcome in COVID-19 Patientsamin mohNo ratings yet
- IJC 9999 NaDocument29 pagesIJC 9999 NaSimona VisanNo ratings yet
- COVID-19 and Newborn HealthDocument12 pagesCOVID-19 and Newborn HealthBrendaElielParedesRodriguezNo ratings yet
- EJMCM - Volume 10 - Issue 1 - Pages 2795-2818Document24 pagesEJMCM - Volume 10 - Issue 1 - Pages 2795-2818Mitul KalathiaNo ratings yet
- B12.Knowledge and Perceptions About COVID-19 Among The Medical and Allied Health Science Students in IndiaDocument6 pagesB12.Knowledge and Perceptions About COVID-19 Among The Medical and Allied Health Science Students in IndiaWislianaNo ratings yet
- Obesity Aggravates COVID-19: A Systematic Review and Meta-AnalysisDocument20 pagesObesity Aggravates COVID-19: A Systematic Review and Meta-AnalysisLuis C Ribon VNo ratings yet
- PBC 28546 PDFDocument2 pagesPBC 28546 PDFRustamNo ratings yet
- Journal Pre-Proof: International Journal of Infectious DiseasesDocument27 pagesJournal Pre-Proof: International Journal of Infectious DiseasesMohammed Shuaib AhmedNo ratings yet
- 2021 04 29 21256327v1 FullDocument33 pages2021 04 29 21256327v1 Fullangel.paternina423No ratings yet
- Covid-19 Vaccination in Pregnancy - The BMJDocument12 pagesCovid-19 Vaccination in Pregnancy - The BMJrichardonNo ratings yet
- Risk Factors For Disease Severity in Paediatric Patients With Covid-19: A Literature ReviewDocument8 pagesRisk Factors For Disease Severity in Paediatric Patients With Covid-19: A Literature ReviewRabania RN29No ratings yet
- BJC 2017154Document8 pagesBJC 2017154Altair CamargoNo ratings yet
- Maternal and Neonatal Outcomes of Pregnant Women With COVID-19 Pneumonia: A Case-Control StudyDocument20 pagesMaternal and Neonatal Outcomes of Pregnant Women With COVID-19 Pneumonia: A Case-Control StudyYogi drNo ratings yet
- Neonatal Covid 19 Exposures and Infections A Systematic Review of Modes of Transmission Manifestations and ManagementDocument18 pagesNeonatal Covid 19 Exposures and Infections A Systematic Review of Modes of Transmission Manifestations and ManagementadeNo ratings yet
- Outcome of Coronavirus Spectrum Infections (SARS, MERS, COVID-19) During Pregnancy: A Systematic Review and Meta-AnalysisDocument9 pagesOutcome of Coronavirus Spectrum Infections (SARS, MERS, COVID-19) During Pregnancy: A Systematic Review and Meta-AnalysisyukihannaNo ratings yet
- Caregivers' Willingness To Accept Expedited Vaccine Research During The COVID-19 Pandemic: A Cross-Sectional SurveyDocument10 pagesCaregivers' Willingness To Accept Expedited Vaccine Research During The COVID-19 Pandemic: A Cross-Sectional SurveyDedi IrawandiNo ratings yet
- Efficacy and Safety of COVID-19 Vaccines A Systematic ReviewDocument16 pagesEfficacy and Safety of COVID-19 Vaccines A Systematic ReviewJuan Paulo P. PulancoNo ratings yet
- Alkodaymi Et Al., 2022 PDFDocument11 pagesAlkodaymi Et Al., 2022 PDFjuliamoreira1No ratings yet
- COVID-19 and The Production of Knowledge Regarding Recommendations During Pregnancy: A Scoping ReviewDocument10 pagesCOVID-19 and The Production of Knowledge Regarding Recommendations During Pregnancy: A Scoping ReviewvalentinNo ratings yet
- Rationale: Prenatal Care in Sta. Maria Health Center Amidst COVID-19: Adjustments For Safe Childbearing OutcomesDocument6 pagesRationale: Prenatal Care in Sta. Maria Health Center Amidst COVID-19: Adjustments For Safe Childbearing OutcomesChristine Joy MolinaNo ratings yet
- Nurses' Burnout and AssociatedDocument18 pagesNurses' Burnout and AssociatedTalipNo ratings yet
- COVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19From EverandCOVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19No ratings yet
- Lab SnakeDocument2 pagesLab SnakeanggipuspaNo ratings yet
- Rabies Vaccine: What You Need To KnowDocument3 pagesRabies Vaccine: What You Need To KnowanggipuspaNo ratings yet
- Journal 1Document14 pagesJournal 1anggipuspaNo ratings yet
- Chart WHO + IDAIDocument46 pagesChart WHO + IDAILovely PoppyNo ratings yet
- HF and Your Ejection Fraction ExplainedDocument1 pageHF and Your Ejection Fraction ExplainedOki AmwinNo ratings yet
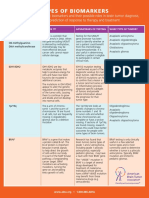
- Types of BiomarkersDocument2 pagesTypes of BiomarkersanggipuspaNo ratings yet
- Red and Orange Flags For Secondary Headaches in Clinical PracticeDocument15 pagesRed and Orange Flags For Secondary Headaches in Clinical PracticeanggipuspaNo ratings yet
- Tuberculous Spondylitis: Risk Factors and Clinical/paraclinical Aspects in The South West of IranDocument5 pagesTuberculous Spondylitis: Risk Factors and Clinical/paraclinical Aspects in The South West of IranDewina Dyani Rosari IINo ratings yet
- Headache Disorders: Differentiating and Managing The Common SubtypesDocument12 pagesHeadache Disorders: Differentiating and Managing The Common SubtypesanggipuspaNo ratings yet
- Handa Notebook Thesis: Here Is Where Your Presentation BeginsDocument56 pagesHanda Notebook Thesis: Here Is Where Your Presentation BeginsSarifudin HusniNo ratings yet
- Intramedullary Conus Medullaris Tuberculoma: A Case Report and Review of The LiteratureDocument7 pagesIntramedullary Conus Medullaris Tuberculoma: A Case Report and Review of The LiteratureanggipuspaNo ratings yet
- S Tibi PDFDocument15 pagesS Tibi PDFagisagitaNo ratings yet
- Operated by The Anterior Approach: A Single-Center Outcome Analysis of Subaxial Cervical Spine TuberculosisDocument9 pagesOperated by The Anterior Approach: A Single-Center Outcome Analysis of Subaxial Cervical Spine TuberculosisanggipuspaNo ratings yet
- Lumbar Puncture - StatPearls - NCBI BookshelfDocument6 pagesLumbar Puncture - StatPearls - NCBI BookshelfanggipuspaNo ratings yet
- Telaah Kritis Artikel Review SistematikDocument4 pagesTelaah Kritis Artikel Review SistematikNorbertus MacekaNo ratings yet
- Cranial Nerves SummaryDocument4 pagesCranial Nerves SummaryanggipuspaNo ratings yet
- Anaesthesia in The Prone Position - British Journal of AnaesthesiaDocument79 pagesAnaesthesia in The Prone Position - British Journal of AnaesthesiaanggipuspaNo ratings yet
- Kriteria Akne VulgarisDocument2 pagesKriteria Akne VulgarisanggipuspaNo ratings yet
- Anemia MantapDocument63 pagesAnemia MantapyasminNo ratings yet
- CT Scan BrainDocument3 pagesCT Scan BrainanggipuspaNo ratings yet
- Ascending Sensory TractDocument1 pageAscending Sensory TractanggipuspaNo ratings yet
- DMDocument1 pageDManggipuspaNo ratings yet
- Annotated Bibliography 2Document5 pagesAnnotated Bibliography 2api-697306255No ratings yet
- Nursing Management of Patients With Occupational DisordersDocument100 pagesNursing Management of Patients With Occupational DisordersNandini VermaNo ratings yet
- BodyBallancer Lipo Brochure PDFDocument2 pagesBodyBallancer Lipo Brochure PDFRoss Gale100% (1)
- Yoga ScopusDocument6 pagesYoga ScopusAtikah AbayNo ratings yet
- UrosepsaDocument2 pagesUrosepsaHazir AziriNo ratings yet
- Perspective On Teaching and LearningDocument67 pagesPerspective On Teaching and LearningJoybelle HarayoNo ratings yet
- Registration at AWC-EnglishDocument2 pagesRegistration at AWC-EnglishSamtha MasineniNo ratings yet
- 封面Document5 pages封面xiaoxin zhang100% (1)
- Prevention of Postpartum Psychosis PDFDocument7 pagesPrevention of Postpartum Psychosis PDFAjengNo ratings yet
- MALNUTRITIONDocument6 pagesMALNUTRITIONEndah FitriNo ratings yet
- Case Study Part II - TogetherDocument8 pagesCase Study Part II - Togetherapi-388989059No ratings yet
- NCM 113 Examination Coverage and DateDocument81 pagesNCM 113 Examination Coverage and DateDONNA MAE FUENTESNo ratings yet
- Zahid RevisedDocument7 pagesZahid Revisedrokeya tamannaNo ratings yet
- 7 Medicine RheumatologyDocument28 pages7 Medicine RheumatologyAmitNo ratings yet
- Infusion Pump: Infuses Medication Nutrients Patient's Circulatory System Intravenously Subcutaneous Arterial EpiduralDocument6 pagesInfusion Pump: Infuses Medication Nutrients Patient's Circulatory System Intravenously Subcutaneous Arterial EpiduralpratonyNo ratings yet
- Sensory Stimulation of Nonverbal Patients in The IcuDocument36 pagesSensory Stimulation of Nonverbal Patients in The Icuapi-506496190No ratings yet
- Stage1 7080971 1048423935 230319 122605Document2 pagesStage1 7080971 1048423935 230319 122605DVET IndiaNo ratings yet
- (Main Manuscript) Clinical Practice Guidelines For The Screening, Diagnosis, Treatment and Prevention of Neonatal SepsisDocument69 pages(Main Manuscript) Clinical Practice Guidelines For The Screening, Diagnosis, Treatment and Prevention of Neonatal Sepsiskaydee.arNo ratings yet
- Intro To Hazardous Materials Unit 1Document17 pagesIntro To Hazardous Materials Unit 1Anonymous pzXvSP25I100% (1)
- Non-Hemolytic Transfusion ReactionDocument32 pagesNon-Hemolytic Transfusion Reactiondreyngerous100% (4)
- SBIL - Health QuestionnaireDocument2 pagesSBIL - Health QuestionnaireKrishna GBNo ratings yet
- 1st Term .Jss3 PheDocument17 pages1st Term .Jss3 Phesamuel joshuaNo ratings yet
- Bpacnz Antibiotics GuideDocument40 pagesBpacnz Antibiotics GuideBulborea MihaelaNo ratings yet
- Basic Concepts in Occupational MedicineDocument52 pagesBasic Concepts in Occupational MedicineEldorhezaNo ratings yet
- Title of The ResearchDocument5 pagesTitle of The ResearchNAMAN PARMARNo ratings yet
- MGT-404Document10 pagesMGT-404Amna KhalidNo ratings yet
- GB 20799-2016 Code of Hygienic Practice For Meat and Meat ProductsDocument6 pagesGB 20799-2016 Code of Hygienic Practice For Meat and Meat Productsjose ManuelNo ratings yet
- Foreign and Local LiteratureDocument3 pagesForeign and Local LiteratureAlexa MayNo ratings yet
- ★★ SOSORT 2022 Abstracts (부보대 마이스터대)Document45 pages★★ SOSORT 2022 Abstracts (부보대 마이스터대)이강민No ratings yet
- Comfort, Effectiveness, AND Self-Awareness AS Criteria OF Improvement IN Psychotherapy"2Document10 pagesComfort, Effectiveness, AND Self-Awareness AS Criteria OF Improvement IN Psychotherapy"2Ilaria PacificoNo ratings yet