You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Pathophysiology of Cluster HeadacheDocument13 pagesPathophysiology of Cluster HeadacheMichael HostiadiNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Chronic Headache 2019 PDFDocument398 pagesChronic Headache 2019 PDFDaniel SisniegasNo ratings yet
- Approach To Patient With HeadacheDocument89 pagesApproach To Patient With Headachehemanthshah2801No ratings yet
- Headaches Clinical Case PDFDocument38 pagesHeadaches Clinical Case PDFGholam AdeliNo ratings yet
- CT Scan BrainDocument3 pagesCT Scan BrainanggipuspaNo ratings yet
- Neurology MCQDocument3 pagesNeurology MCQAlshare NisreenNo ratings yet
- Vol 24.4 - Headache.2018 PDFDocument287 pagesVol 24.4 - Headache.2018 PDFMartoiu MariaNo ratings yet
- Neurological ExaminationDocument55 pagesNeurological ExaminationWasemBhatNo ratings yet
- Exam 2018 PDFDocument62 pagesExam 2018 PDFWondimu Koy100% (1)
- General Practitioner - Neurology MCQsDocument20 pagesGeneral Practitioner - Neurology MCQsAsif Newaz100% (3)
- Cluster Headache and Other Trigeminal Autonomic CephalalgiasDocument19 pagesCluster Headache and Other Trigeminal Autonomic CephalalgiasBryan100% (1)
- Lab SnakeDocument2 pagesLab SnakeanggipuspaNo ratings yet
- Journal 1Document14 pagesJournal 1anggipuspaNo ratings yet
- Rabies Vaccine: What You Need To KnowDocument3 pagesRabies Vaccine: What You Need To KnowanggipuspaNo ratings yet
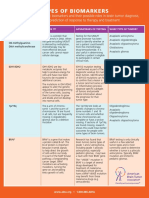
- Types of BiomarkersDocument2 pagesTypes of BiomarkersanggipuspaNo ratings yet
- Intramedullary Conus Medullaris Tuberculoma: A Case Report and Review of The LiteratureDocument7 pagesIntramedullary Conus Medullaris Tuberculoma: A Case Report and Review of The LiteratureanggipuspaNo ratings yet
- Clinical Presentation and Outcomes of Pregnant Women With Coronavirus Disease 2019: A Systematic Review and Meta-AnalysisDocument13 pagesClinical Presentation and Outcomes of Pregnant Women With Coronavirus Disease 2019: A Systematic Review and Meta-AnalysisanggipuspaNo ratings yet
- Anaesthesia in The Prone Position - British Journal of AnaesthesiaDocument79 pagesAnaesthesia in The Prone Position - British Journal of AnaesthesiaanggipuspaNo ratings yet
- Nyeri Kepala IAFKU, DR Betty, SPSDocument43 pagesNyeri Kepala IAFKU, DR Betty, SPSMuhammad AsrizalNo ratings yet
- #2 Headache DestroyerDocument47 pages#2 Headache DestroyerBruce rNo ratings yet
- The Use of Cannabis For Headache DisordersDocument11 pagesThe Use of Cannabis For Headache DisordersNazmi ZegarraNo ratings yet
- Greater Occipital Nerve Block For Migraine Prophylaxis - Full Text View - ClinicalTrials - GovDocument10 pagesGreater Occipital Nerve Block For Migraine Prophylaxis - Full Text View - ClinicalTrials - Govkillingeyes177No ratings yet
- Evaluation of Headache in Adults - UpToDateDocument18 pagesEvaluation of Headache in Adults - UpToDateSebastianNo ratings yet
- Insect PoliticsDocument5 pagesInsect PoliticsFOBCNo ratings yet
- Headache & Fascial Pain Blok NEURO 2020Document67 pagesHeadache & Fascial Pain Blok NEURO 2020lathifatulNo ratings yet
- Cluster HeadacheDocument1 pageCluster HeadacheDaniel FuentesNo ratings yet
- SDL 21 Headaches BMS16091064Document8 pagesSDL 21 Headaches BMS16091064Jonathan YeohNo ratings yet
- Review Article: Cluster Headache-Acute and Prophylactic TherapyDocument24 pagesReview Article: Cluster Headache-Acute and Prophylactic TherapyPurna Adi PutraNo ratings yet
- Chapter 60: Headache: Section 10: NeurologyDocument16 pagesChapter 60: Headache: Section 10: NeurologyAnonymous Xmb6QQvRNo ratings yet
- Headache: Paul G. Mathew, M.D., and Ivan Garza, M.DDocument13 pagesHeadache: Paul G. Mathew, M.D., and Ivan Garza, M.DElizabeth PedruezaNo ratings yet
- CephalgiaDocument30 pagesCephalgiaMurdani MurdaniasihNo ratings yet
- 5.nervous System PDFDocument88 pages5.nervous System PDFMelancholy MedicineNo ratings yet
- Migraine and Cluster HeadacheDocument24 pagesMigraine and Cluster HeadachekhemamettaNo ratings yet
- Cluster HeadacheDocument2 pagesCluster HeadachenanikNo ratings yet
- Gaul Et Al 2011Document9 pagesGaul Et Al 2011gottid1No ratings yet
- Inbound 4715243803028409675Document12 pagesInbound 4715243803028409675NylNo ratings yet
- 11 Types of Headaches - Causes, Symptoms, and TreatmentDocument27 pages11 Types of Headaches - Causes, Symptoms, and TreatmentCHIMA ONWUKA MONGNo ratings yet
- Cluster HeadacheDocument14 pagesCluster HeadacheadriantiariNo ratings yet