You might also like
- Proposal To UNICEFDocument14 pagesProposal To UNICEFJanet Ilott100% (2)
- Mali Situation Report - August 14Document6 pagesMali Situation Report - August 14InterActionNo ratings yet
- Reginald Xavier, MD: Summary of Key Achievements & StrengthsDocument5 pagesReginald Xavier, MD: Summary of Key Achievements & StrengthsAnonymous eq1sOnIUNo ratings yet
- Acra Quarter 3 Narrative Report 2023.Document15 pagesAcra Quarter 3 Narrative Report 2023.pmNo ratings yet
- Mali 120627 Sitrep10 FinalDocument8 pagesMali 120627 Sitrep10 FinalInterActionNo ratings yet
- Strengtheningemergencyhealthcare GambiaDocument10 pagesStrengtheningemergencyhealthcare GambiaDurroh YatimahNo ratings yet
- Reginald Xavier, MD: Summary of Key Achievements & StrengthsDocument5 pagesReginald Xavier, MD: Summary of Key Achievements & StrengthsReginald XavierNo ratings yet
- Critical Assessment of Zambian Health SystemDocument13 pagesCritical Assessment of Zambian Health SystemCObinyaNo ratings yet
- Saving Mothers, Giving Life Phase 1 Monitoring and Evaluation FindingsDocument28 pagesSaving Mothers, Giving Life Phase 1 Monitoring and Evaluation FindingsAnchored AfricaNo ratings yet
- WFP Chad, Standard Project Report 2011: "Assistance To CAR Refugees and Host Population in Chad"Document21 pagesWFP Chad, Standard Project Report 2011: "Assistance To CAR Refugees and Host Population in Chad"Kendra MasseyNo ratings yet
- International Health Agencies and Role of Commumity Health NurseDocument28 pagesInternational Health Agencies and Role of Commumity Health NurseMahak SachdevaNo ratings yet
- Who Covid-19 Situation Report For July 20, 2020Document21 pagesWho Covid-19 Situation Report For July 20, 2020CityNewsTorontoNo ratings yet
- Working Paper Health Service Delivery PNGDocument82 pagesWorking Paper Health Service Delivery PNGJoex Aim0% (1)
- Mali 120620 Sitrep9 FinalDocument8 pagesMali 120620 Sitrep9 FinalInterActionNo ratings yet
- A Health and Nutrition Head of DepartmentDocument3 pagesA Health and Nutrition Head of Departmentreem esamNo ratings yet
- Request For Expression of Interest For Endline Assessment of Protect-Gac ProjectDocument8 pagesRequest For Expression of Interest For Endline Assessment of Protect-Gac ProjectNhial Lam KhorNo ratings yet
- Kazakhstan: in BriefDocument13 pagesKazakhstan: in BriefGina MinjinaNo ratings yet
- Unicef Report 2013 ZimbabweDocument20 pagesUnicef Report 2013 ZimbabwejimmaloNo ratings yet
- Amhara Field Office Report: 1. Highlights & Critical Issues 2. Utilization ProgressDocument7 pagesAmhara Field Office Report: 1. Highlights & Critical Issues 2. Utilization ProgressTesfaye BelayeNo ratings yet
- Philippines: Situation Report 13Document5 pagesPhilippines: Situation Report 13Krizzia Mae Soriano-Sta InesNo ratings yet
- Echo Hip Evaluation Final 1Document68 pagesEcho Hip Evaluation Final 1Fuad AlawzariNo ratings yet
- Emergency Health Services 2019Document3 pagesEmergency Health Services 2019Think BeforeNo ratings yet
- In The Democratic Republic of Congo: Contributions To Its Economic DevelopmentDocument20 pagesIn The Democratic Republic of Congo: Contributions To Its Economic DevelopmentEurich EstradaNo ratings yet
- EMRO-report Health of Refugees and MigrantsDocument22 pagesEMRO-report Health of Refugees and MigrantsHiader RabeaaNo ratings yet
- United Nations: Six-Month US$28 Million Action Plan To Provide Immediate Health Care For Cyclone Survivors, andDocument5 pagesUnited Nations: Six-Month US$28 Million Action Plan To Provide Immediate Health Care For Cyclone Survivors, andmyochitmyanmarNo ratings yet
- ACF Tech The News FSL - July 2010 FinalDocument15 pagesACF Tech The News FSL - July 2010 FinalRS GFNo ratings yet
- Challenges Faced During The Development of New High DemandDocument11 pagesChallenges Faced During The Development of New High DemandDr Ruth SengonziNo ratings yet
- MCH Program Description: PhilippinesDocument3 pagesMCH Program Description: PhilippinesMaya RodajeNo ratings yet
- The Infews (JORDAN) - June 2012Document2 pagesThe Infews (JORDAN) - June 2012InfewsNo ratings yet
- CI EA Evaluation ToRDocument7 pagesCI EA Evaluation ToRresearchkenyaNo ratings yet
- Kakuma Emergency UpdateDocument4 pagesKakuma Emergency Updatedjsonja07No ratings yet
- Final Proposal - NutritionDocument31 pagesFinal Proposal - NutritionKafil Ahmed0% (1)
- Namibia 2015 COARDocument50 pagesNamibia 2015 COARKhushboo ParikhNo ratings yet
- "Sehat Sahulat Program" - A Leap Into The Universal Health CoveraDocument9 pages"Sehat Sahulat Program" - A Leap Into The Universal Health Coverasameershah9sNo ratings yet
- Kenya Questions FinalDocument13 pagesKenya Questions Finalrossimaia35No ratings yet
- Bakamushanga Francis - Assgmt Hospital MGTDocument8 pagesBakamushanga Francis - Assgmt Hospital MGTMulongo LinoNo ratings yet
- Dilla, Ethiopia May, 2018 Chapter One 1 1.1. Background of The StudyDocument84 pagesDilla, Ethiopia May, 2018 Chapter One 1 1.1. Background of The StudyKindhun TegegnNo ratings yet
- National Health Accounts of The Republic of Botswana: 2000-2002Document35 pagesNational Health Accounts of The Republic of Botswana: 2000-2002iisteNo ratings yet
- Social Infrrastructure (Andhrapradesh)Document23 pagesSocial Infrrastructure (Andhrapradesh)ramachanderbNo ratings yet
- Pang Yuyu TongtaDocument27 pagesPang Yuyu Tongtaapi-280412367No ratings yet
- ETHIOPIA: COVID-19 Humanitarian Impact Situation Update No. 2Document7 pagesETHIOPIA: COVID-19 Humanitarian Impact Situation Update No. 2Marema GetachewNo ratings yet
- NHM RCHDocument37 pagesNHM RCHAnju MargaretNo ratings yet
- iNSCALE Stakeholder Analysis Final Report - iCCM in UgandaDocument20 pagesiNSCALE Stakeholder Analysis Final Report - iCCM in UgandaiNSCALENo ratings yet
- Information On UNHCDocument6 pagesInformation On UNHCHanan BiyaNo ratings yet
- UNFPADocument4 pagesUNFPAAmna KhanNo ratings yet
- Launch of UPHIA 2020Document6 pagesLaunch of UPHIA 2020GCICNo ratings yet
- Emergency Plan of Action (Epoa) Niger Complex Emergency: A. Situation AnalysisDocument28 pagesEmergency Plan of Action (Epoa) Niger Complex Emergency: A. Situation AnalysisNaveed UllahNo ratings yet
- Application For Grants Organization Information Name of Organization/InstitutitionDocument11 pagesApplication For Grants Organization Information Name of Organization/InstitutitionMarrion Adrian L. SolisNo ratings yet
- Case Studies 2012Document68 pagesCase Studies 2012Yay SandovalNo ratings yet
- Articles: BackgroundDocument9 pagesArticles: BackgroundBassim BirklandNo ratings yet
- Namibia 2016 COARDocument59 pagesNamibia 2016 COARKhushboo ParikhNo ratings yet
- SICKLEDocument5 pagesSICKLEmutoto andrewNo ratings yet
- 438 D 70432Document51 pages438 D 70432Silent TravelerNo ratings yet
- United Arab Emirates: Health & DevelopmentDocument2 pagesUnited Arab Emirates: Health & DevelopmentMichelle ChangNo ratings yet
- Equity and The Expansion of Access To Treatment and Care For HIV/AIDS in Southern Africa: Report of A Workshop at ICASADocument7 pagesEquity and The Expansion of Access To Treatment and Care For HIV/AIDS in Southern Africa: Report of A Workshop at ICASAOxfamNo ratings yet
- ACERWC 3rd CSO Forum Session Safe Motherhood Campaign PresentationDocument12 pagesACERWC 3rd CSO Forum Session Safe Motherhood Campaign PresentationACERWC CSO ForumNo ratings yet
- Vision Centre Swali, Bayelsa StateDocument25 pagesVision Centre Swali, Bayelsa StateAF Dowell MirinNo ratings yet
- India Situation Report 73Document3 pagesIndia Situation Report 73dhivyascrNo ratings yet
- Protection Project Implemented in Yemen, Hani BanafaDocument3 pagesProtection Project Implemented in Yemen, Hani BanafaHani BanafaNo ratings yet
- Somalia Administrative Units BoundariesDocument1 pageSomalia Administrative Units BoundariesJohn ShearerNo ratings yet
- Marketing Research Product: BournvitaDocument23 pagesMarketing Research Product: BournvitaTanveer Singh Rainu75% (20)
- Lapkas Marasmus-Down SyndromeDocument37 pagesLapkas Marasmus-Down SyndromeKURBULDKNo ratings yet
- The Importance of Maternal Nutrition During Breastfeeding: Do Breastfeeding Mothers Need Nutritional Supplements?Document8 pagesThe Importance of Maternal Nutrition During Breastfeeding: Do Breastfeeding Mothers Need Nutritional Supplements?Nadya SafitriNo ratings yet
- Feeding ProgramDocument5 pagesFeeding ProgramElenor Abrigo25% (4)
- Marasmus Kwashiorkor 12022009Document62 pagesMarasmus Kwashiorkor 12022009Ardie Ceme ThedoctorNo ratings yet
- Early Childhood Development - UNICEF Vision For Every ChildDocument32 pagesEarly Childhood Development - UNICEF Vision For Every ChildYakubu Abdul sommedNo ratings yet
- JOURNAL Where Is The Nurse in Nutritional CareDocument5 pagesJOURNAL Where Is The Nurse in Nutritional Carevia macarioNo ratings yet
- TSFP Monitoring ChecklistDocument5 pagesTSFP Monitoring ChecklistAnas Abdo Senan100% (4)
- New Developments in Clinical Practice Guidelines: Invited CommunicationDocument4 pagesNew Developments in Clinical Practice Guidelines: Invited CommunicationCar OrdzNo ratings yet
- FNCP MalnutritionDocument1 pageFNCP MalnutritionoctoberttwentythreeNo ratings yet
- The State of The World's Children 2011: Adolescence - An Age of OpportunityDocument148 pagesThe State of The World's Children 2011: Adolescence - An Age of OpportunityUNICEF100% (2)
- Hepatic EncephalopathyDocument65 pagesHepatic Encephalopathyvishal padwaleNo ratings yet
- Passion ProjectDocument10 pagesPassion Projectapi-315431657No ratings yet
- The Global Goals in AfricaDocument55 pagesThe Global Goals in AfricashjahsjanshaNo ratings yet
- Reaction Paper On DivergentDocument3 pagesReaction Paper On DivergentAndy MolinaNo ratings yet
- Module 1 4 PrelimDocument27 pagesModule 1 4 PrelimChezka MendozaNo ratings yet
- 5 Sorting Paper 2-PalsDocument4 pages5 Sorting Paper 2-PalsYogesh SukhdeveNo ratings yet
- Maternal & Child Health CareDocument209 pagesMaternal & Child Health CareAhsan Ul Kayum Bhuiyan100% (1)
- 2016 Nutrition Month Talking PointsDocument28 pages2016 Nutrition Month Talking PointsEli Benjamin Nava Taclino89% (9)
- - أسئلة التغذيةDocument52 pages- أسئلة التغذيةMicheal Mikhail YoussefNo ratings yet
- Guidance Document - Nutritional Care & Support For TB Patients in India PDFDocument107 pagesGuidance Document - Nutritional Care & Support For TB Patients in India PDFekalubisNo ratings yet
- Essential Nutrition Actions in Nigeria: The Basics Ii ExperienceDocument59 pagesEssential Nutrition Actions in Nigeria: The Basics Ii ExperienceFrancis AminuNo ratings yet
- Sustaining The Earth 10th Edition Miller Test BankDocument28 pagesSustaining The Earth 10th Edition Miller Test Bankrowenagabrieleatq100% (23)
- Rhetorical Analysis On HungerDocument7 pagesRhetorical Analysis On Hungerapi-402344897No ratings yet
- V. End The Ache Today: The AdvocacyDocument2 pagesV. End The Ache Today: The AdvocacyAudrey RamosNo ratings yet
- NNSA StrategyDocument35 pagesNNSA StrategyHenock GezahegnNo ratings yet
- NRC Guidelines GujrathDocument68 pagesNRC Guidelines GujrathNirajkumar KondekarNo ratings yet
- Nutrition and DisabilityDocument7 pagesNutrition and DisabilityNUR SYAHIRA AQILAH NOR IZAMNo ratings yet
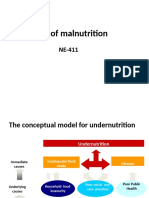
- Causes of MalnutritionDocument13 pagesCauses of MalnutritionEman ZahraNo ratings yet