You might also like
- The Science Behind Mini-WorkoutsDocument5 pagesThe Science Behind Mini-WorkoutsMIIIBNo ratings yet
- Art 272Document8 pagesArt 272Homemade ANo ratings yet
- Financial Impact of A Comprehensive Multisite Workplace Health Promotion ProgramDocument7 pagesFinancial Impact of A Comprehensive Multisite Workplace Health Promotion ProgramGaurav SharmaNo ratings yet
- High Intensity Interval Training ThesisDocument6 pagesHigh Intensity Interval Training Thesiskarabellcary100% (1)
- The Effects of Pilates Exercise On Cardiopulmonary Function in The Chronic Stroke Patients A Randomized Controlled Trials PDFDocument5 pagesThe Effects of Pilates Exercise On Cardiopulmonary Function in The Chronic Stroke Patients A Randomized Controlled Trials PDFImam santosoNo ratings yet
- Exercise For Fitness: (Shs-Videolecture-1 & 2 Week)Document18 pagesExercise For Fitness: (Shs-Videolecture-1 & 2 Week)Mark Joshua MandaniNo ratings yet
- Long QuizDocument6 pagesLong QuizMae EsmadeNo ratings yet
- Module 1 Introduction To Physical Activity and FitnessDocument34 pagesModule 1 Introduction To Physical Activity and Fitnessalisa leyNo ratings yet
- Exercise For Fitness Lesson 1Document5 pagesExercise For Fitness Lesson 1Wendilyn PalaparNo ratings yet
- 148 2022 01 21 08 48 05 700Document6 pages148 2022 01 21 08 48 05 700Adithya PutraNo ratings yet
- 2018%2F7856823Document4 pages2018%2F7856823itskasho0332No ratings yet
- Ijerph 17 02632 v2Document16 pagesIjerph 17 02632 v2Ricardo Martín MoyaNo ratings yet
- Power of Strength Training For Older AdultsDocument6 pagesPower of Strength Training For Older Adultsvazrak100% (1)
- PE & HEALTH 1: Recommended Physical Activity Levels for Filipino TeenagersDocument4 pagesPE & HEALTH 1: Recommended Physical Activity Levels for Filipino TeenagersSea are YellowNo ratings yet
- The Benefits of Custom Exergames For Fitness, Balance, and Health-Related Quality of Life: A Randomized Controlled Trial With Community-Dwelling Older AdultsDocument9 pagesThe Benefits of Custom Exergames For Fitness, Balance, and Health-Related Quality of Life: A Randomized Controlled Trial With Community-Dwelling Older AdultsAnonymous HUY0yRexYfNo ratings yet
- Reading Report Electiva IVDocument8 pagesReading Report Electiva IVFelipe AcostaNo ratings yet
- Effects of Low-Intensity Resistance Exercise With Vascular Occlusion On Physical Function in Healthy Elderly People.-2Document7 pagesEffects of Low-Intensity Resistance Exercise With Vascular Occlusion On Physical Function in Healthy Elderly People.-2Ingrid Ramirez PNo ratings yet
- Physical Fitness HandoutsDocument4 pagesPhysical Fitness HandoutsMay B. Pineda100% (1)
- JPES Chenetal 2016 PDFDocument7 pagesJPES Chenetal 2016 PDFRizqiAnnisaPermatasariNo ratings yet
- Pathfit 2 LessonsDocument11 pagesPathfit 2 Lessonsalshameer0130No ratings yet
- 2008 Physical Activity Guidelines: National Council On Strength & FitnessDocument2 pages2008 Physical Activity Guidelines: National Council On Strength & FitnessPaulo ZulluNo ratings yet
- Circuit training improves fitness of athletes & non-athletesDocument18 pagesCircuit training improves fitness of athletes & non-athletesbugsbusgNo ratings yet
- Physical Activity and Exercise GuideDocument3 pagesPhysical Activity and Exercise GuideSophia FabriquierNo ratings yet
- IJPR.2016.191 Kebugaran Pada LansiaDocument8 pagesIJPR.2016.191 Kebugaran Pada LansiaMas AbrarNo ratings yet
- Exercise As Defensive Nutritional Paradigm - MSC Sem3FPP - 19-20 - NALSDocument18 pagesExercise As Defensive Nutritional Paradigm - MSC Sem3FPP - 19-20 - NALSdrashti shahNo ratings yet
- Geriatrics 0 GerontologyDocument9 pagesGeriatrics 0 GerontologysajidaNo ratings yet
- Optimizing The Combination of Oxytocin M 7872188dDocument6 pagesOptimizing The Combination of Oxytocin M 7872188dAnggi WidyaNo ratings yet
- Study Proposal For Senior CitizensDocument15 pagesStudy Proposal For Senior CitizensParul ThakurNo ratings yet
- Coverage For QuizDocument12 pagesCoverage For QuizSaila mae SurioNo ratings yet
- Geriatrics 07 00088Document10 pagesGeriatrics 07 0008834. Putu Mariska Abdi CahyaniNo ratings yet
- Physical Education Objectives: Develop Skills and Promote Healthy LifestyleDocument12 pagesPhysical Education Objectives: Develop Skills and Promote Healthy Lifestylekeanee simbajonNo ratings yet
- Reviewer in PHYSICAL EDUCATION 11: Second SemesterDocument6 pagesReviewer in PHYSICAL EDUCATION 11: Second SemesterFredeline R. GonzalesNo ratings yet
- BENEFITS OF PHYSICAL ACTIVITY - 2023 10 11varDocument25 pagesBENEFITS OF PHYSICAL ACTIVITY - 2023 10 11varAuksė GalbuogienėNo ratings yet
- I T E P: Ntroduction O Xercise HysiologyDocument35 pagesI T E P: Ntroduction O Xercise HysiologyDoDongBulawinNo ratings yet
- Effectiveness of Poco-Poco Exercise On Elderly's Cholesterol Levels: A Preliminary StudyDocument10 pagesEffectiveness of Poco-Poco Exercise On Elderly's Cholesterol Levels: A Preliminary StudyAli FirdausNo ratings yet
- ACSMGuidelines UNMDocument6 pagesACSMGuidelines UNMWagner PereiraNo ratings yet
- Exercise As A Boost For The Health Promotion of The ElderlyDocument65 pagesExercise As A Boost For The Health Promotion of The ElderlyPeace OghoNo ratings yet
- Performance and Sports Nutrition: Handbook with nutritional factors that can influence physical performanceFrom EverandPerformance and Sports Nutrition: Handbook with nutritional factors that can influence physical performanceRating: 5 out of 5 stars5/5 (2)
- Eu Physical Activity Guidelines 2008 (Ab Beden Eğitimi Rehberi)Document38 pagesEu Physical Activity Guidelines 2008 (Ab Beden Eğitimi Rehberi)lukNo ratings yet
- SSRN Id4642178Document14 pagesSSRN Id4642178valands618No ratings yet
- PE Physical Fitness and Physical ActivityDocument13 pagesPE Physical Fitness and Physical ActivityLenajanelle LlamesNo ratings yet
- Impact of Whole Body Electromyostimulation On Velocity, Power and Body Composition in Postmenopausal Women: A Randomized Controlled TrialDocument17 pagesImpact of Whole Body Electromyostimulation On Velocity, Power and Body Composition in Postmenopausal Women: A Randomized Controlled TrialVALERIO KIKUCHINo ratings yet
- Taller Segunda LenguaDocument5 pagesTaller Segunda LenguaOscar AriasNo ratings yet
- Literature Review On Aerobic ExerciseDocument4 pagesLiterature Review On Aerobic Exercisegvzwyd4nNo ratings yet
- Importance of Fitness and WellnessDocument21 pagesImportance of Fitness and WellnessAmicable VanuNo ratings yet
- JurnalDocument7 pagesJurnalghozi hilmyNo ratings yet
- Assignment 06Document4 pagesAssignment 06ALISON JACOB OBEDENCIONo ratings yet
- PATHFITDocument12 pagesPATHFITJANREY NAVALTANo ratings yet
- DownloadDocument9 pagesDownloadcesar8319No ratings yet
- Tai chi improves proprioception in elderlyDocument5 pagesTai chi improves proprioception in elderlyPhooi Yee LauNo ratings yet
- Seniors' Musculoskeletal Health GuideDocument77 pagesSeniors' Musculoskeletal Health GuideMiden AlbanoNo ratings yet
- Ijerph 16 04205Document17 pagesIjerph 16 04205yrds consultNo ratings yet
- PATHFITT 2- HandoutsDocument14 pagesPATHFITT 2- HandoutsDona Caballejo- ArcenaNo ratings yet
- Impact of Resistance Circuit Training On Neuromuscular, Cardiorespiratory and Body Composition Adaptations in The ElderlyDocument8 pagesImpact of Resistance Circuit Training On Neuromuscular, Cardiorespiratory and Body Composition Adaptations in The ElderlyBryan HuaritaNo ratings yet
- Medicina 57010072Document8 pagesMedicina 57010072SportsciencesNo ratings yet
- Suzzzan WorkDocument4 pagesSuzzzan WorkmarymagvichillNo ratings yet
- Ansai Et Al. (2016) PDFDocument8 pagesAnsai Et Al. (2016) PDFvabrandaoNo ratings yet
- 3 ActivityDocument46 pages3 ActivityFlourence ZafranNo ratings yet
- PE1 Lecture1Document26 pagesPE1 Lecture1Raphael Morante0% (1)
- Launch of A Model of Care For Specialist Geriatric ServicesDocument4 pagesLaunch of A Model of Care For Specialist Geriatric ServiceseimearNo ratings yet
- Find or Check An EircodeDocument1 pageFind or Check An EircodeeimearNo ratings yet
- (Grade Code 6404) : Louise - Collins4@hse - IeDocument7 pages(Grade Code 6404) : Louise - Collins4@hse - IeeimearNo ratings yet
- CH 230 20 Job SpecificationDocument8 pagesCH 230 20 Job SpecificationeimearNo ratings yet
- 2016 National Clinical Guideline For Stroke 5th Edition - 24 11 16 PDFDocument178 pages2016 National Clinical Guideline For Stroke 5th Edition - 24 11 16 PDFRegina TungkumasNo ratings yet
- Irish Heart Foundation: Council For StrokeDocument117 pagesIrish Heart Foundation: Council For StrokeeimearNo ratings yet
- Framework for Improving Health Service QualityDocument26 pagesFramework for Improving Health Service QualityNIAZ HUSSAINNo ratings yet
- European Physiotherapy Guideline For Parkinson's PDFDocument191 pagesEuropean Physiotherapy Guideline For Parkinson's PDFAnonymous Da2Idf100% (3)
- CGA Terjemah PDFDocument64 pagesCGA Terjemah PDFagung kurniawanNo ratings yet
- RP50Document7 pagesRP50eimearNo ratings yet
- Physiotherapy in Parkinsons DiseaseDocument21 pagesPhysiotherapy in Parkinsons DiseaseeimearNo ratings yet
- Circuit Class Therapy For Improving Mobility After Stroke (Review)Document31 pagesCircuit Class Therapy For Improving Mobility After Stroke (Review)eimearNo ratings yet
- National Clinical Programme for Respiratory End to End COPD Model of CareDocument86 pagesNational Clinical Programme for Respiratory End to End COPD Model of CareeimearNo ratings yet
- Virtual Pulmonary Rehab GuideDocument24 pagesVirtual Pulmonary Rehab GuideeimearNo ratings yet
- Hse Guidance Document On Pulmonary RehabilitationDocument48 pagesHse Guidance Document On Pulmonary RehabilitationeimearNo ratings yet
- Copd in General Practice - Icgp Quality in Clinical Practice CommitteeDocument21 pagesCopd in General Practice - Icgp Quality in Clinical Practice CommitteeeimearNo ratings yet
- Mul - Factorial Falls Risk Assessment: (Acute Hospital)Document2 pagesMul - Factorial Falls Risk Assessment: (Acute Hospital)eimearNo ratings yet
- COPD Guide for GPsDocument28 pagesCOPD Guide for GPseimearNo ratings yet
- Guidance For Setting Up A Virtual Supported Discharge Service For Covid 19Document20 pagesGuidance For Setting Up A Virtual Supported Discharge Service For Covid 19eimearNo ratings yet
- Abbreviated Mental Test ScoreDocument1 pageAbbreviated Mental Test ScoreeimearNo ratings yet
- h09 Sat 0900 LindopDocument23 pagesh09 Sat 0900 LindopeimearNo ratings yet
- Clinical Frailty Scale AssessmentDocument1 pageClinical Frailty Scale AssessmenteimearNo ratings yet
- Mul - Factorial Falls Risk Assessment: (Acute Hospital)Document2 pagesMul - Factorial Falls Risk Assessment: (Acute Hospital)eimearNo ratings yet
- Super satisfying & calorie-light Superfree foodsDocument5 pagesSuper satisfying & calorie-light Superfree foodseimear100% (1)
- Clinical Frailty Scale AssessmentDocument1 pageClinical Frailty Scale AssessmenteimearNo ratings yet
- Signature: Patient Name: Hospital NumberDocument1 pageSignature: Patient Name: Hospital NumbereimearNo ratings yet
- Service Annotated BibDocument3 pagesService Annotated Bibapi-302015493No ratings yet
- Endurance, Resistance and Flexibility ExerciseDocument6 pagesEndurance, Resistance and Flexibility ExerciseNicole ReidNo ratings yet
- Birdetal 2005SportsMed3510841-851Document12 pagesBirdetal 2005SportsMed3510841-851Edu SantosNo ratings yet
- First Periodical Exam in MAPEH 11 - SHSDocument4 pagesFirst Periodical Exam in MAPEH 11 - SHSkentjames corales100% (1)
- PE and Health Week 7 Module 7 Participating in An Organized Event (Hiphop) What I KnowDocument13 pagesPE and Health Week 7 Module 7 Participating in An Organized Event (Hiphop) What I KnowAshlyn WilsonNo ratings yet
- 5 The Stretching Debate'Document2 pages5 The Stretching Debate'АлексNo ratings yet
- Sports Day ScriptDocument3 pagesSports Day ScriptSargam PahakNo ratings yet
- I. Case-Body PowerDocument11 pagesI. Case-Body PowerKaushik NayakNo ratings yet
- UNIT-5 Physical Fitness, Wellness & HealthDocument6 pagesUNIT-5 Physical Fitness, Wellness & HealthSwayam Dayanand MalakasamudrNo ratings yet
- 25 Pull Up ProgramDocument6 pages25 Pull Up Programmooney2375% (4)
- 100 No-Equipment Workouts: 2015 EditionDocument209 pages100 No-Equipment Workouts: 2015 EditionChristian López MasNo ratings yet
- ACTIVITY 1 Week 7Document6 pagesACTIVITY 1 Week 7more100% (1)
- Kayaking 3 Week Lesson PlanDocument3 pagesKayaking 3 Week Lesson Planapi-294951409No ratings yet
- Hipertrofia MuscularDocument22 pagesHipertrofia MuscularNonato MendonçaNo ratings yet
- Master Class 100 MDocument151 pagesMaster Class 100 MJorge Lozano DiezNo ratings yet
- The Calisthenics Skill Tree (template)1.6.1.xlsx - TREEDocument1 pageThe Calisthenics Skill Tree (template)1.6.1.xlsx - TREEtahaNo ratings yet
- DLP Free Style Basic SkillsDocument6 pagesDLP Free Style Basic SkillsYklim V ZepedaNo ratings yet
- Muscle & Fitness UK 01-2015Document196 pagesMuscle & Fitness UK 01-2015Petra100% (3)
- Southeastern College Final Exam Questions on First Aid, Wellness, Climate ChangeDocument2 pagesSoutheastern College Final Exam Questions on First Aid, Wellness, Climate ChangeJayson Quito BudionganNo ratings yet
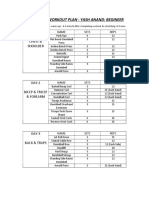
- 90 DAY GYM PLAN FOR BEGINNERSDocument2 pages90 DAY GYM PLAN FOR BEGINNERSDebarghya NandaNo ratings yet
- Physical Education and Health-G12 Ms. Keren Kiscia Jemimah A. Gonzales & Ms. Danica C. CablaidaDocument5 pagesPhysical Education and Health-G12 Ms. Keren Kiscia Jemimah A. Gonzales & Ms. Danica C. CablaidaCade MorganNo ratings yet
- Complete ThesisDocument35 pagesComplete ThesisSunny BediNo ratings yet
- Walk FitDocument24 pagesWalk FitPaul JonesNo ratings yet
- Ped1 Final Part 1Document2 pagesPed1 Final Part 1Jay Carlo BagayasNo ratings yet
- Calendario InsanityDocument2 pagesCalendario InsanityyujoeyNo ratings yet
- Activities 1Document63 pagesActivities 1Angelito AdoptanteNo ratings yet
- Sports VocabularyDocument17 pagesSports Vocabularyhelloisme933No ratings yet
- Course Outline PE 1 Fitness Education 123Document2 pagesCourse Outline PE 1 Fitness Education 123arianeNo ratings yet
- Health Optimizing Physical Education 2ND SemesterDocument7 pagesHealth Optimizing Physical Education 2ND Semesteruno100% (2)
- Eric J Carpenter CV October 2014Document11 pagesEric J Carpenter CV October 2014api-269904708No ratings yet