You might also like
- The Ultimate Guide to Vascular Ultrasound: Diagnosing and Understanding Vascular ConditionsFrom EverandThe Ultimate Guide to Vascular Ultrasound: Diagnosing and Understanding Vascular ConditionsNo ratings yet
- Author Section Editor Deputy Editor Contributor DisclosuresDocument10 pagesAuthor Section Editor Deputy Editor Contributor DisclosuresannisNo ratings yet
- Duplex and Color Doppler Imaging of the Venous SystemFrom EverandDuplex and Color Doppler Imaging of the Venous SystemGerhard H. MostbeckNo ratings yet
- Reprod Domestic Animals - 2014 - Ortega Ferrusola - Use of Colour and Spectral Doppler Ultrasonography in StallionDocument9 pagesReprod Domestic Animals - 2014 - Ortega Ferrusola - Use of Colour and Spectral Doppler Ultrasonography in StallionAmanda CristinaNo ratings yet
- Genitourinary UltrasoundDocument215 pagesGenitourinary UltrasoundAnselmus Regie100% (4)
- Basicultrasound-Guided Procedures: Laurel Barr,, Nicholas Hatch,, Pedro J. Roque,, Teresa S. WuDocument30 pagesBasicultrasound-Guided Procedures: Laurel Barr,, Nicholas Hatch,, Pedro J. Roque,, Teresa S. WuKenzo HongThanhNo ratings yet
- Decoding Cardiac Electrophysiology: Understanding the Techniques and Defining the JargonFrom EverandDecoding Cardiac Electrophysiology: Understanding the Techniques and Defining the JargonAfzal SohaibNo ratings yet
- Röntgen's X-ray Discovery Revolutionized Medical ImagingDocument2 pagesRöntgen's X-ray Discovery Revolutionized Medical ImagingNitin AwasthiNo ratings yet
- Appendix A: Doppler Ultrasound and Ankle-Brachial Pressure IndexDocument26 pagesAppendix A: Doppler Ultrasound and Ankle-Brachial Pressure IndexabigailNo ratings yet
- Medical Ultrasound - WikipediaDocument30 pagesMedical Ultrasound - WikipedianibNo ratings yet
- Ultrasound A CL 2021Document17 pagesUltrasound A CL 2021Alejandra SanchezNo ratings yet
- Vasc Med 2006 Gerhard Herman 183 200Document19 pagesVasc Med 2006 Gerhard Herman 183 200Ahmad ShaltoutNo ratings yet
- Fundamentals of Body CT 5th EdDocument415 pagesFundamentals of Body CT 5th EdRuxandra TartaNo ratings yet
- Point of Care NHJMDocument9 pagesPoint of Care NHJMFernanda Araújo AvendanhaNo ratings yet
- Fundamentals of CT PDFDocument415 pagesFundamentals of CT PDFAl Marchese100% (1)
- CT Angiography of The Lower Extremities The Peripheral Vascular System Presents Unique Imaging ChallengesDocument7 pagesCT Angiography of The Lower Extremities The Peripheral Vascular System Presents Unique Imaging ChallengesDavid Puyó100% (1)
- Mehu107 - U28 - T1 - Trauma Abdominal - Artículo - 2Document39 pagesMehu107 - U28 - T1 - Trauma Abdominal - Artículo - 2Diana Salas SosaNo ratings yet
- Diagnostic Ultrasound For The Detection of Atherosclerotic Changes Inside Femoral Arteries of Lower LimbDocument4 pagesDiagnostic Ultrasound For The Detection of Atherosclerotic Changes Inside Femoral Arteries of Lower LimbInternational Jpurnal Of Technical Research And ApplicationsNo ratings yet
- Ultrasound Exam in The Practice of UrologyDocument12 pagesUltrasound Exam in The Practice of UrologychimbimbNo ratings yet
- Role of US and IVU in evaluating hematuriaDocument8 pagesRole of US and IVU in evaluating hematuriaalda aldaNo ratings yet
- Echocardiographic Assessment of Valve Stenosis: EAE/ASE Recommendations For Clinical PracticeDocument25 pagesEchocardiographic Assessment of Valve Stenosis: EAE/ASE Recommendations For Clinical PracticeLucy ManuriNo ratings yet
- 心脏超声基础知识(超声心动图基础知识)Document12 pages心脏超声基础知识(超声心动图基础知识)Xin HuangNo ratings yet
- WSAVA Proceedings Highlights HRCT for Small Animal Lung ImagingDocument5 pagesWSAVA Proceedings Highlights HRCT for Small Animal Lung ImagingKiki D. RestikaNo ratings yet
- PIIS0749070413000742Document46 pagesPIIS0749070413000742Juan Carlos MezaNo ratings yet
- Imaging Abdominal Trauma Focus On FAST Revisi DR - BahtiarDocument54 pagesImaging Abdominal Trauma Focus On FAST Revisi DR - BahtiarJackson HakimNo ratings yet
- Ultrasound diagnosis and management of pleural effusionDocument5 pagesUltrasound diagnosis and management of pleural effusionegerpratamaNo ratings yet
- Intervencion Usg EmergenciasDocument22 pagesIntervencion Usg EmergenciasSaul Gonzalez HernandezNo ratings yet
- Radiology Case ReportsDocument5 pagesRadiology Case ReportsLaila Maria UlfahNo ratings yet
- Guide To USDocument11 pagesGuide To USAdel HamadaNo ratings yet
- Clinical Applications of Transthoracic UltrasoundDocument20 pagesClinical Applications of Transthoracic UltrasoundFabiana Gonzalez da NóbregaNo ratings yet
- EJE2010 - Eco en Enfermedad de AortaDocument14 pagesEJE2010 - Eco en Enfermedad de AortaRaul GascueñaNo ratings yet
- Ultrasound Imaging of The AbdomenDocument224 pagesUltrasound Imaging of The AbdomenAsztalos Attila100% (9)
- Gambar Usg TestisDocument28 pagesGambar Usg TestisIrfan YHNo ratings yet
- Echocardiography Dissertation IdeasDocument8 pagesEchocardiography Dissertation IdeasWhoCanWriteMyPaperForMeCanada100% (1)
- Point-Of-care Ultrasonography N Engl J Med 3648749Document10 pagesPoint-Of-care Ultrasonography N Engl J Med 3648749Andreas Natan100% (1)
- Zuva MuzachimDocument6 pagesZuva MuzachimZuva MuzachimNo ratings yet
- Thyroid UltrasoundDocument9 pagesThyroid UltrasoundMoh SuriyawalNo ratings yet
- Cannulation: Meta-Analysis Ultrasonic Locating Devices For Central VenousDocument8 pagesCannulation: Meta-Analysis Ultrasonic Locating Devices For Central VenousandriellycamposNo ratings yet
- Hallifax Radiological Investigation of Pleural DiseaseDocument38 pagesHallifax Radiological Investigation of Pleural Diseaselaila.forestaNo ratings yet
- Aortic AneurysmDocument17 pagesAortic AneurysmTeguh Imana NugrahaNo ratings yet
- Policies and Statements: Peripheral Arterial UltrasoundDocument5 pagesPolicies and Statements: Peripheral Arterial UltrasoundJing CruzNo ratings yet
- Scrotal Ultrasound in AdultsDocument17 pagesScrotal Ultrasound in AdultsMagzNo ratings yet
- Focusedassessment Withsonographyfor Trauma:Methods, Accuracy, and IndicationsDocument13 pagesFocusedassessment Withsonographyfor Trauma:Methods, Accuracy, and IndicationsOtto Guillermo SontayNo ratings yet
- GINECOLOGIEDocument105 pagesGINECOLOGIEBanaru AnaNo ratings yet
- Ultrasoundforthe Diagnosisand Managementof Ureterolithiasisinthe Emergency DepartmentDocument3 pagesUltrasoundforthe Diagnosisand Managementof Ureterolithiasisinthe Emergency DepartmentMarcelitaTaliaDuwiriNo ratings yet
- Ultrasound: Asst - Lec. Sura Mohammed Saeed AhmedDocument17 pagesUltrasound: Asst - Lec. Sura Mohammed Saeed AhmedOsama HayderNo ratings yet
- T - P D U I R E: Hree Dimensional and Ower Oppler Ltrasonography in Nfertility and Eproductive NdocrinologyDocument6 pagesT - P D U I R E: Hree Dimensional and Ower Oppler Ltrasonography in Nfertility and Eproductive NdocrinologyAripinSyarifudinNo ratings yet
- Lung BiopsyDocument8 pagesLung BiopsySiya PatilNo ratings yet
- Angiographic ThoracalisDocument22 pagesAngiographic ThoracalisermaendahNo ratings yet
- UltrasoundTraumaCh02 Fast ExamDocument23 pagesUltrasoundTraumaCh02 Fast Exam108dudleyNo ratings yet
- Ankle-Brachial Index For Assessment of Peripheral Arterial DiseaseDocument5 pagesAnkle-Brachial Index For Assessment of Peripheral Arterial DiseaseindrawepeNo ratings yet
- Fast Scan 2022Document9 pagesFast Scan 2022rosieNo ratings yet
- Coronary Artery Occlusions Diagnosed by Transthoracic DopplerDocument11 pagesCoronary Artery Occlusions Diagnosed by Transthoracic DopplerNag Mallesh RaoNo ratings yet
- Fluid Collection USGDocument103 pagesFluid Collection USGhendrizalzubirNo ratings yet
- CT of Abdominal Trauma: A Step-By-Step Approach: Robert A. Halvorsen, JR., M.DDocument11 pagesCT of Abdominal Trauma: A Step-By-Step Approach: Robert A. Halvorsen, JR., M.DKamlesh AgrawalNo ratings yet
- 04mos PDFDocument10 pages04mos PDFMarcelitaTaliaDuwiriNo ratings yet
- Accessory Spleen: V. Durgesh, CH. Roja RaniDocument3 pagesAccessory Spleen: V. Durgesh, CH. Roja RaniIOSRjournalNo ratings yet
- Ultrasonography in EffusionDocument6 pagesUltrasonography in EffusionRachmat AnsyoriNo ratings yet
- عرض تقديمي5Document41 pagesعرض تقديمي5Elshaer MohammedNo ratings yet
- Testicular Ultrasound: A Concise GuideDocument26 pagesTesticular Ultrasound: A Concise GuideElshaer MohammedNo ratings yet
- عرض تقديمي1Document19 pagesعرض تقديمي1Elshaer MohammedNo ratings yet
- Question 1Document5 pagesQuestion 1Elshaer MohammedNo ratings yet
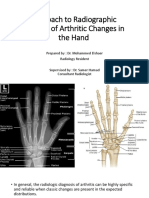
- Approach To Radiographic Analysis of Arthritic Changes in The HandDocument49 pagesApproach To Radiographic Analysis of Arthritic Changes in The HandElshaer MohammedNo ratings yet
- Pediatric Bone Imaging Differentiating Benign Lesions From MalignantDocument9 pagesPediatric Bone Imaging Differentiating Benign Lesions From MalignantElshaer MohammedNo ratings yet
- Imaging of Acute Pancreatitis and Its ComplicationsDocument62 pagesImaging of Acute Pancreatitis and Its ComplicationsElshaer MohammedNo ratings yet
- Pediatric Bone Imaging Differentiating Benign Lesions From MalignantDocument9 pagesPediatric Bone Imaging Differentiating Benign Lesions From MalignantElshaer MohammedNo ratings yet
- Journeys B2 Teacher's Resource Pack: Grammar ThemesDocument2 pagesJourneys B2 Teacher's Resource Pack: Grammar ThemesMiriam SanchezNo ratings yet
- TwistiesDocument2 pagesTwistiesHazwan Hj YusofNo ratings yet
- National Power Corporation vs. Teresita Diato-Bernal 2Document3 pagesNational Power Corporation vs. Teresita Diato-Bernal 2mickcarpioNo ratings yet
- WWII 2nd Army HistoryDocument192 pagesWWII 2nd Army HistoryCAP History Library100% (1)
- Syllabus Changes: March 2021 Version 1Document20 pagesSyllabus Changes: March 2021 Version 1Azul IrlaundeNo ratings yet
- Lcasean PaperDocument6 pagesLcasean Paperkean ebeoNo ratings yet
- 5 Integumentary SystemDocument67 pages5 Integumentary SystemchelsealivesforeverNo ratings yet
- Business Studies Project: Made By: Rahil JainDocument29 pagesBusiness Studies Project: Made By: Rahil JainChirag KothariNo ratings yet
- Underwater Cutting and Welding Equipment - 89250054 - AbDocument38 pagesUnderwater Cutting and Welding Equipment - 89250054 - AbAhmed Adel100% (1)
- Pas 220Document71 pagesPas 220JuwitaNo ratings yet
- Biology and Aquaculture of Tilapia-Routledge (2022)Document324 pagesBiology and Aquaculture of Tilapia-Routledge (2022)Pablo Antonio Pintos TeránNo ratings yet
- 9th Science Mcqs PTB PDFDocument25 pages9th Science Mcqs PTB PDFUmar JuttNo ratings yet
- MSDS TriacetinDocument4 pagesMSDS TriacetinshishirchemNo ratings yet
- Breakfast For Kirsten GillibrandDocument5 pagesBreakfast For Kirsten GillibrandSunlight FoundationNo ratings yet
- Research Project On Capital PunishmentDocument6 pagesResearch Project On Capital PunishmentNitwit NoddyNo ratings yet
- Plattischemic Stroke Lesson PlanDocument18 pagesPlattischemic Stroke Lesson Planapi-216258123100% (3)
- Advertising and Imc Principles and Practice 11th Edition Moriarty Solutions ManualDocument28 pagesAdvertising and Imc Principles and Practice 11th Edition Moriarty Solutions Manualcemeteryliana.9afku100% (19)
- MMA2019 SDocument2 pagesMMA2019 SToni IbrahimNo ratings yet
- Art of Public Speaking 11th Edition Lucas Test BankDocument25 pagesArt of Public Speaking 11th Edition Lucas Test BankBryanMillernicy100% (49)
- Revised SCOPE OF WORK and SCCDocument363 pagesRevised SCOPE OF WORK and SCCZia KhanNo ratings yet
- Sam's Melancholic MorningDocument4 pagesSam's Melancholic Morningali moizNo ratings yet
- Facilitating Learner Centered Teaching FinalsDocument3 pagesFacilitating Learner Centered Teaching FinalsPatricia Andrei De GuzmanNo ratings yet
- Manocha Icile Feasibility StudyDocument95 pagesManocha Icile Feasibility StudyAlmadin KeñoraNo ratings yet
- NIMS University Jaipur - Ph.D. Economics Selection Process, Course Fee, PlacementDocument6 pagesNIMS University Jaipur - Ph.D. Economics Selection Process, Course Fee, PlacementstepincollegeNo ratings yet
- Quiz Bowl QuestionsDocument8 pagesQuiz Bowl QuestionsKeenan Dave RivoNo ratings yet
- Curative Petition Draft TutorialDocument4 pagesCurative Petition Draft TutorialBhavya SinghNo ratings yet
- Sat Psat Word GamesDocument166 pagesSat Psat Word Gamesapi-360773187No ratings yet
- Warehousing Functions and TypesDocument5 pagesWarehousing Functions and TypesporseenaNo ratings yet
- Gateway A2 Test 1BDocument3 pagesGateway A2 Test 1BNewteacher29100% (6)
- Edge Computing As A Service: How Macrometa is Revolutionizing Global Data ProcessingDocument8 pagesEdge Computing As A Service: How Macrometa is Revolutionizing Global Data ProcessingAtlantis-ILIONo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (41)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)