You might also like
- TAE40116 DesignCluster AWB v2.1Document117 pagesTAE40116 DesignCluster AWB v2.1Mashael Suliman100% (1)
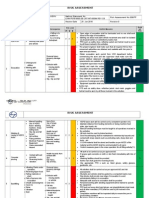
- Hse Risk Assessment - 006 Ra - Hdpe Duct LayingDocument7 pagesHse Risk Assessment - 006 Ra - Hdpe Duct Layingbinunalukandam83% (12)
- Chapter 39 Pain Management in ChildrenDocument3 pagesChapter 39 Pain Management in ChildrenAllyssa Mackinnon0% (1)
- TAE40116 DeliveryCluster AWB v1.10Document163 pagesTAE40116 DeliveryCluster AWB v1.10Mashael Suliman100% (1)
- Share your neck pain levelsDocument2 pagesShare your neck pain levelsnovaNo ratings yet
- Assess Patient Pain ThoroughlyDocument5 pagesAssess Patient Pain Thoroughlyisapatrick8126No ratings yet
- Health AssessmentDocument30 pagesHealth AssessmentWeng RamojalNo ratings yet
- Pain assessment toolsDocument22 pagesPain assessment toolspuchioNo ratings yet
- Final Post TestDocument23 pagesFinal Post TestJoanne Bernadette AguilarNo ratings yet
- CH 4D PainDocument41 pagesCH 4D PainKevin FacunNo ratings yet
- Nurses Guide to Pain Assessment & ManagementDocument32 pagesNurses Guide to Pain Assessment & ManagementroyNo ratings yet
- Updated CH 30 Pain Assessment and ManagementDocument30 pagesUpdated CH 30 Pain Assessment and Managementaabbccss1.z71No ratings yet
- Pain ManagementDocument14 pagesPain Managementsoumya mNo ratings yet
- Heart Clinic: Alternative Learning System Related Learning ExperienceDocument8 pagesHeart Clinic: Alternative Learning System Related Learning ExperienceEdson John DemayoNo ratings yet
- Pain AssessmentDocument33 pagesPain AssessmentmujawayezuNo ratings yet
- 3 Peran Perawat Dalam Managemen Nyeri-1Document55 pages3 Peran Perawat Dalam Managemen Nyeri-1Anonymous PBDr0ONo ratings yet
- Pain Assessment and Management in 40 CharactersDocument27 pagesPain Assessment and Management in 40 CharactersSWAPNIL WANJARINo ratings yet
- Pain Assessment in Older Adults Post Viewing ReportDocument2 pagesPain Assessment in Older Adults Post Viewing ReportLiam HenryNo ratings yet
- Pain AssessmentDocument43 pagesPain AssessmentJalajarani AridassNo ratings yet
- Pain Sessment: Pain in The Cognitively ImpairedDocument43 pagesPain Sessment: Pain in The Cognitively Impairedalya1alya1No ratings yet
- PainDocument35 pagesPainixora n100% (1)
- PainDocument42 pagesPainIkbal MaulanaNo ratings yet
- mindfulnessforchronicpainmanagementDocument4 pagesmindfulnessforchronicpainmanagementrasanka2014No ratings yet
- Review of Nursing Process Implementation Evaluation Hand OutDocument8 pagesReview of Nursing Process Implementation Evaluation Hand OutJurinia VicenteNo ratings yet
- NCP Charm EditedDocument6 pagesNCP Charm EditedampogeNo ratings yet
- 10-Powell+etal-V2 2 PDFDocument12 pages10-Powell+etal-V2 2 PDFPenelopeShamNo ratings yet
- Pain AssessmentDocument15 pagesPain AssessmentAvash ZhaNo ratings yet
- Lecture 6 Pain Management in Children by Pharmacological and NonDocument25 pagesLecture 6 Pain Management in Children by Pharmacological and NonRubinaNo ratings yet
- Pain Management: Assessing and Treating with ScalesDocument28 pagesPain Management: Assessing and Treating with ScalesSawera ChNo ratings yet
- Viii. Nursing Management Nursing Care Plan # 1 Assessment Diagnosis Planning Implementation Rationale EvaluationDocument6 pagesViii. Nursing Management Nursing Care Plan # 1 Assessment Diagnosis Planning Implementation Rationale EvaluationStar AlvarezNo ratings yet
- Self-Rating Pain And: Distress ScaleDocument7 pagesSelf-Rating Pain And: Distress ScaleMiila AzizahNo ratings yet
- Pain in Palliative CareDocument28 pagesPain in Palliative CareMhmoud NabehNo ratings yet
- Acute Pain Nursing Diagnosis & Care Plan - NurseslabsDocument1 pageAcute Pain Nursing Diagnosis & Care Plan - NurseslabsShimaa Al SiyabiNo ratings yet
- Lesson 2 SummaryDocument15 pagesLesson 2 SummarySarah SmithNo ratings yet
- Acute Pain (Nyeri Akut)Document8 pagesAcute Pain (Nyeri Akut)Eki MegaraniNo ratings yet
- Palliative CareDocument54 pagesPalliative CareOGU CourageNo ratings yet
- Dokumen - Tips - 46201478 NCP Acute Abdominal Pain PDFDocument5 pagesDokumen - Tips - 46201478 NCP Acute Abdominal Pain PDFmikhailNo ratings yet
- Pain Management Nursing Skills TypesDocument4 pagesPain Management Nursing Skills TypesBrittania CorbittNo ratings yet
- Materi Pelatihan Manajemen Nyeri 2019Document52 pagesMateri Pelatihan Manajemen Nyeri 2019Iman Muhamad FirmansyahNo ratings yet
- Bulandos BSN3-1 Duty Act 4Document7 pagesBulandos BSN3-1 Duty Act 4Rolan BulandosNo ratings yet
- Forgiveness Therapy: "It's Not About What They Did or Didn't Do. It's About How You Feel. You Have Control Over That."Document12 pagesForgiveness Therapy: "It's Not About What They Did or Didn't Do. It's About How You Feel. You Have Control Over That."Kinza Saher BasraNo ratings yet
- Post-CS Nursing Care Plan GoalsDocument7 pagesPost-CS Nursing Care Plan GoalsshinloNo ratings yet
- Module9Video2 PainManagementTrDocument9 pagesModule9Video2 PainManagementTrKrishnendu WorkNo ratings yet
- Pain Assessment: tEAM 5Document22 pagesPain Assessment: tEAM 5Lý VũNo ratings yet
- NCPDocument6 pagesNCPAndrea Marie SevillaNo ratings yet
- Managing Acute Pain: A Guide For PatientsDocument21 pagesManaging Acute Pain: A Guide For Patientsanindya2293No ratings yet
- A Guide To Pain Assessment and ManagementDocument14 pagesA Guide To Pain Assessment and ManagementKitesaMedeksaNo ratings yet
- EPM UK Workshop ManualDocument67 pagesEPM UK Workshop ManualMaisie RobertsNo ratings yet
- Module D Pain AssessmentDocument12 pagesModule D Pain Assessmentmwhite8051100% (1)
- EPM Partic Manual 2e FinalDocument64 pagesEPM Partic Manual 2e FinalRyan GusnaintinNo ratings yet
- Goals and Outcomes: Acute Pain Is Characterized by The Following Signs and SymptomsDocument5 pagesGoals and Outcomes: Acute Pain Is Characterized by The Following Signs and SymptomsCyril Jane Caanyagan AcutNo ratings yet
- Nursing Care PlanDocument6 pagesNursing Care PlanRohmanNo ratings yet
- Nursing Care PlanDocument9 pagesNursing Care PlanKenneth Mark B. TevesNo ratings yet
- 8.3 Pain PresentationDocument24 pages8.3 Pain PresentationEstela Such GilNo ratings yet
- Facing Your Feelings - 03 - Improving Distress PDFDocument15 pagesFacing Your Feelings - 03 - Improving Distress PDFletitia2hintonNo ratings yet
- Facing Your Feelings - 03 - Improving Distress PDFDocument15 pagesFacing Your Feelings - 03 - Improving Distress PDFletitia2hintonNo ratings yet
- 1 s2.0 S1094919422000457 MainDocument29 pages1 s2.0 S1094919422000457 MainRafael Silva CortésNo ratings yet
- Assessing People's PainDocument4 pagesAssessing People's PainJullienne ManguladNo ratings yet
- Vital Sign PainDocument42 pagesVital Sign PainAbdul MajidNo ratings yet
- TAE40116 AssessmentCluster AWB v2.8Document105 pagesTAE40116 AssessmentCluster AWB v2.8Mashael Suliman0% (2)
- Accredited Course Document Template 0Document30 pagesAccredited Course Document Template 0Mashael SulimanNo ratings yet
- Workshop Summary For 8th and 11th MarchDocument9 pagesWorkshop Summary For 8th and 11th MarchMashael Suliman0% (1)
- Friendly Reminder e Mail TemplateDocument1 pageFriendly Reminder e Mail TemplateMashael SulimanNo ratings yet
- Workshop Summary For 8th and 11th MarchDocument9 pagesWorkshop Summary For 8th and 11th MarchMashael Suliman0% (1)
- Trial Validation Process Template - V2021Document10 pagesTrial Validation Process Template - V2021Mashael SulimanNo ratings yet
- Workshop Summary For 22nd and 25th FebruaryDocument14 pagesWorkshop Summary For 22nd and 25th FebruaryMashael SulimanNo ratings yet
- Workshop Summary For 8th and 11th MarchDocument9 pagesWorkshop Summary For 8th and 11th MarchMashael Suliman0% (1)
- CHCPAL001 Deliver Care Services Using A Palliative Approach: Release: 2Document5 pagesCHCPAL001 Deliver Care Services Using A Palliative Approach: Release: 2Mashael SulimanNo ratings yet
- Pain Management Strategies in Aged Care FacilitiesDocument6 pagesPain Management Strategies in Aged Care FacilitiesMashael SulimanNo ratings yet
- Myths UpdatedDocument3 pagesMyths UpdatedMashael SulimanNo ratings yet
- ACT Best Practice Palliative Care WorkbookDocument22 pagesACT Best Practice Palliative Care WorkbookMashael SulimanNo ratings yet
- S4019772final ThesisDocument284 pagesS4019772final ThesisMashael SulimanNo ratings yet
- Documentation SkillsDocument2 pagesDocumentation SkillsCharles SauerNo ratings yet
- Topic 1: © Aspire Training & ConsultingDocument20 pagesTopic 1: © Aspire Training & ConsultingMashael SulimanNo ratings yet
- Ni Hms 783055Document27 pagesNi Hms 783055Mashael SulimanNo ratings yet
- Acute Complications of Diabetes MellitusDocument1 pageAcute Complications of Diabetes MellitusGerardLum100% (1)
- The30 Itemand15 itemBostonnamingtestCzechBezdiceketal.2022Document17 pagesThe30 Itemand15 itemBostonnamingtestCzechBezdiceketal.2022Alexander OrzocoNo ratings yet
- Penile Injection TherapyDocument4 pagesPenile Injection Therapydr NayanBharadwajNo ratings yet
- Republic Act 10932 Anti-Hospital Deposit LawDocument9 pagesRepublic Act 10932 Anti-Hospital Deposit LawVenus PangilinanNo ratings yet
- West Fertilizer FINAL Report For Website 0223161 PDFDocument267 pagesWest Fertilizer FINAL Report For Website 0223161 PDFJawahar KhetanNo ratings yet
- Round Hill Community Garden FAQ - Round Hill, VirginiaDocument3 pagesRound Hill Community Garden FAQ - Round Hill, VirginiaZafiriou MavrogianniNo ratings yet
- Display PDFDocument8 pagesDisplay PDFSri BalajiNo ratings yet
- Anatomia SufletuluiDocument1 pageAnatomia SufletuluiAlexandrina DeaşNo ratings yet
- Booklet - e 1 - 2013Document101 pagesBooklet - e 1 - 2013Dani AedoNo ratings yet
- Evaluation and Treatment of Aphasia Among The Elderly With StrokeDocument11 pagesEvaluation and Treatment of Aphasia Among The Elderly With StrokemgpastorNo ratings yet
- T2anklearthrodesis Optech b1000044d0710Document36 pagesT2anklearthrodesis Optech b1000044d0710Alsed GjoniNo ratings yet
- Intern Performance Review TemplateDocument3 pagesIntern Performance Review TemplatePrincess Joan InguitoNo ratings yet
- Food Safety Plan For CateringDocument80 pagesFood Safety Plan For CateringNghia Khang100% (1)
- Health Declaration FormDocument1 pageHealth Declaration FormAlintana JobelleNo ratings yet
- Borderline Personality DisorderDocument7 pagesBorderline Personality DisorderleaNo ratings yet
- SSIPDocument4 pagesSSIPGlenn Clemente100% (2)
- U WORLD (Step 1) – INFECTIOUS DISEASES + MICROBIOLOGY (EDUCATIONAL OBJECTIVESDocument75 pagesU WORLD (Step 1) – INFECTIOUS DISEASES + MICROBIOLOGY (EDUCATIONAL OBJECTIVESDrbee10No ratings yet
- Neonatal Care Pocket Guide For Hospital Physicians PDFDocument319 pagesNeonatal Care Pocket Guide For Hospital Physicians PDFelmaadawy2002100% (7)
- Power of The Pinch Pinch Lower Lid BlepharoplastyDocument6 pagesPower of The Pinch Pinch Lower Lid BlepharoplastyBFF BotoxNo ratings yet
- Quality Improvement: The Model For Improvement, PDSA Cycles, and Accelerating ImprovementDocument37 pagesQuality Improvement: The Model For Improvement, PDSA Cycles, and Accelerating ImprovementDewi ListyoriniNo ratings yet
- Child Abuse Research JournalDocument9 pagesChild Abuse Research JournaladrianekattnerNo ratings yet
- Rizzuto God MindDocument22 pagesRizzuto God MindSpats65No ratings yet
- Pesticide ApplicationDocument5 pagesPesticide ApplicationPrashant GurjarNo ratings yet
- Hsmi Hudco TrainingDocument20 pagesHsmi Hudco TrainingThomas PeguNo ratings yet
- Study To Access The Knowledge Under Five Mothers Regarding Prevention of Malnutrition in Ankuli Berhampur Ganjam OdishaDocument59 pagesStudy To Access The Knowledge Under Five Mothers Regarding Prevention of Malnutrition in Ankuli Berhampur Ganjam OdishaPabhat Kumar100% (2)
- BPN Datangi MalaysiaDocument62 pagesBPN Datangi MalaysiaafandianddonkeyNo ratings yet
- Empowering Women Key to Ending PovertyDocument25 pagesEmpowering Women Key to Ending PovertydassmbaNo ratings yet
- 1.2 POWERPOINT History of ForensicsDocument23 pages1.2 POWERPOINT History of ForensicsSilay Parole & ProbationNo ratings yet
- Kurukshetra University PhD Entrance Exam GuideDocument27 pagesKurukshetra University PhD Entrance Exam GuidemanojrkmNo ratings yet