You might also like
- Pharmacology Nursing MnemonicsDocument23 pagesPharmacology Nursing MnemonicsJoanne Bernadette Aguilar100% (1)
- Holotropic BreathworkDocument14 pagesHolotropic BreathworkHrvatski strelicarski savez100% (5)
- Psychotropic MedicationsDocument37 pagesPsychotropic MedicationsJoanne Bernadette AguilarNo ratings yet
- Hidden Power of The HeartDocument318 pagesHidden Power of The HeartMichael Kovach100% (2)
- PainDocument35 pagesPainixora n100% (1)
- Nursing Care Plan For Acute PainDocument5 pagesNursing Care Plan For Acute PainPhilippineNursingDirectory.com100% (9)
- Complete Head To Toe AssessmentDocument13 pagesComplete Head To Toe AssessmentJoanne Bernadette AguilarNo ratings yet
- Irene Diet - Imprisoned in The Spiritual VoidDocument42 pagesIrene Diet - Imprisoned in The Spiritual Voidstephen mattoxNo ratings yet
- Leadership and Managemen AssignmentDocument3 pagesLeadership and Managemen AssignmentaninNo ratings yet
- NCP - Acute Abdominal PainDocument3 pagesNCP - Acute Abdominal PainJet Bautista100% (2)
- Case Study ResearchDocument8 pagesCase Study ResearchDon Chiaw ManongdoNo ratings yet
- Pain Management CHNDocument38 pagesPain Management CHNVaibhavi ShastriNo ratings yet
- Assess Patient Pain ThoroughlyDocument5 pagesAssess Patient Pain Thoroughlyisapatrick8126No ratings yet
- Acute Pain Nursing Diagnosis & Care Plan - NurseslabsDocument1 pageAcute Pain Nursing Diagnosis & Care Plan - NurseslabsShimaa Al SiyabiNo ratings yet
- NCP Charm EditedDocument6 pagesNCP Charm EditedampogeNo ratings yet
- Grade 12 LM PR2 1 Module2Document33 pagesGrade 12 LM PR2 1 Module2Ariza Alvarez CabitanaNo ratings yet
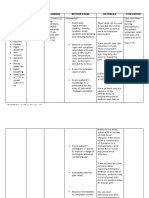
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument5 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationArian May MarcosNo ratings yet
- NURSING CARE PLAN of Hodgkin's Lymphoma: Assessment Nursing Diagnosis Planning Nursing Interventions Rationale EvaluationDocument5 pagesNURSING CARE PLAN of Hodgkin's Lymphoma: Assessment Nursing Diagnosis Planning Nursing Interventions Rationale Evaluationjoyrena ochondraNo ratings yet
- Health: Quarter 3 - Module 2: Coping With Stress, Dying and DeathDocument10 pagesHealth: Quarter 3 - Module 2: Coping With Stress, Dying and DeathDyanne De JesusNo ratings yet
- Compt - Appraisal Prelim 2 Glenda CasundoDocument19 pagesCompt - Appraisal Prelim 2 Glenda CasundoJoanne Bernadette AguilarNo ratings yet
- Pain assessment toolsDocument22 pagesPain assessment toolspuchioNo ratings yet
- Goals and Outcomes: Acute Pain Is Characterized by The Following Signs and SymptomsDocument5 pagesGoals and Outcomes: Acute Pain Is Characterized by The Following Signs and SymptomsCyril Jane Caanyagan AcutNo ratings yet
- Chronic Pain: Understanding and Managing Long-Term DiscomfortDocument10 pagesChronic Pain: Understanding and Managing Long-Term DiscomfortEki MegaraniNo ratings yet
- Heart Clinic: Alternative Learning System Related Learning ExperienceDocument8 pagesHeart Clinic: Alternative Learning System Related Learning ExperienceEdson John DemayoNo ratings yet
- 10-Powell+etal-V2 2 PDFDocument12 pages10-Powell+etal-V2 2 PDFPenelopeShamNo ratings yet
- Acute Pain (Nyeri Akut)Document8 pagesAcute Pain (Nyeri Akut)Eki MegaraniNo ratings yet
- Acute Pain Nursing Diagnosis & Care Plans - NurseTogetherDocument22 pagesAcute Pain Nursing Diagnosis & Care Plans - NurseTogetherrachealakusukNo ratings yet
- Updated CH 30 Pain Assessment and ManagementDocument30 pagesUpdated CH 30 Pain Assessment and Managementaabbccss1.z71No ratings yet
- Acute Pain - Marcos NCPDocument4 pagesAcute Pain - Marcos NCPArian May MarcosNo ratings yet
- 2009 Pain Assessment and ManagementDocument22 pages2009 Pain Assessment and ManagementErnawa RikaNo ratings yet
- Diagnostic Findings:: Short Term Goal Short Term GoalDocument3 pagesDiagnostic Findings:: Short Term Goal Short Term GoalGiselle EstoquiaNo ratings yet
- Acute PainDocument5 pagesAcute PainEricka MunsayacNo ratings yet
- 1 s2.0 S1094919422000457 MainDocument29 pages1 s2.0 S1094919422000457 MainRafael Silva CortésNo ratings yet
- Assessing People's PainDocument4 pagesAssessing People's PainJullienne ManguladNo ratings yet
- Hospice, Palliative and Supportive Care for the Terminally IllDocument4 pagesHospice, Palliative and Supportive Care for the Terminally IllJudy Ignacio EclarinoNo ratings yet
- Pain Assessment and Management in 40 CharactersDocument27 pagesPain Assessment and Management in 40 CharactersSWAPNIL WANJARINo ratings yet
- Grieve and LossDocument6 pagesGrieve and LossRuffy AbdulazisNo ratings yet
- Nurses Guide to Pain Assessment & ManagementDocument32 pagesNurses Guide to Pain Assessment & ManagementroyNo ratings yet
- Palliative CareDocument54 pagesPalliative CareOGU CourageNo ratings yet
- Assessment Nursing Diagnosis Scientific Explanation Planning Intervention Rationale Evaluation IndeoendentDocument3 pagesAssessment Nursing Diagnosis Scientific Explanation Planning Intervention Rationale Evaluation IndeoendentDiane Sarino CabonceNo ratings yet
- Chap 10 - Lewis MSN Philippine 8eDocument26 pagesChap 10 - Lewis MSN Philippine 8eCHABELITA DAVIDNo ratings yet
- Disorders NCPDocument7 pagesDisorders NCPFaye Dianne Damian-BuenafeNo ratings yet
- Understanding Pain ManagementDocument32 pagesUnderstanding Pain ManagementAbbeygale GalanNo ratings yet
- Amabel U. Cortez (G4A) March 1, 2019 Mary Mediatrix Medical Center Head Nurse: Jose Marco B. de CastroDocument9 pagesAmabel U. Cortez (G4A) March 1, 2019 Mary Mediatrix Medical Center Head Nurse: Jose Marco B. de CastroBel CortezNo ratings yet
- LP KDP Minggu 1 Ghandis - R.MawarDocument13 pagesLP KDP Minggu 1 Ghandis - R.MawarrafaNo ratings yet
- Nursing interventions for pain and nutrition managementDocument8 pagesNursing interventions for pain and nutrition managementNyeam NyeamNo ratings yet
- Pain Measurement 2Document6 pagesPain Measurement 2Shahnawaz ShahNo ratings yet
- Assessment NyeriDocument18 pagesAssessment NyerisnookumsnjNo ratings yet
- Pain Management: Assessing and Treating with ScalesDocument28 pagesPain Management: Assessing and Treating with ScalesSawera ChNo ratings yet
- Nursing Care Plan - Acute PainDocument1 pageNursing Care Plan - Acute PainAj GoNo ratings yet
- Coping Resources and Affective Responses: Assessment InterviewDocument6 pagesCoping Resources and Affective Responses: Assessment Interviewrahtu suzi ameliaNo ratings yet
- Dokumen - Tips - 46201478 NCP Acute Abdominal Pain PDFDocument5 pagesDokumen - Tips - 46201478 NCP Acute Abdominal Pain PDFmikhailNo ratings yet
- Pain Management Strategies in Aged Care FacilitiesDocument6 pagesPain Management Strategies in Aged Care FacilitiesMashael SulimanNo ratings yet
- Clinician Pain Assessment TemplatesDocument23 pagesClinician Pain Assessment TemplatesAhmed YunusNo ratings yet
- The Nurse's Role in Pain Assessment and ManagementDocument12 pagesThe Nurse's Role in Pain Assessment and Managementbea_estiponaNo ratings yet
- Assessment of Chronic Pain: Domains, Methods, and MechanismsDocument11 pagesAssessment of Chronic Pain: Domains, Methods, and MechanismsDana LebadaNo ratings yet
- 3 Peran Perawat Dalam Managemen Nyeri-1Document55 pages3 Peran Perawat Dalam Managemen Nyeri-1Anonymous PBDr0ONo ratings yet
- Ncm-212-Pain Reliever and Anti-Inflammatory DrugsDocument8 pagesNcm-212-Pain Reliever and Anti-Inflammatory Drugskristine caminNo ratings yet
- NCP For ChronicPain PDFDocument2 pagesNCP For ChronicPain PDFjay kusainNo ratings yet
- Pain Assessment in Older Adults Post Viewing ReportDocument2 pagesPain Assessment in Older Adults Post Viewing ReportLiam HenryNo ratings yet
- NCP - GeriaDocument4 pagesNCP - GeriaMarielle J GarciaNo ratings yet
- NCP 1Document2 pagesNCP 1oguitekim1No ratings yet
- Review of Nursing Process Implementation Evaluation Hand OutDocument8 pagesReview of Nursing Process Implementation Evaluation Hand OutJurinia VicenteNo ratings yet
- Intervene Education BookletDocument24 pagesIntervene Education BookletMashael SulimanNo ratings yet
- A01 Pain in The Cognitively Impaired ElderlyDocument9 pagesA01 Pain in The Cognitively Impaired ElderlyGabriel CampolinaNo ratings yet
- Assessing Pain in Verbal Older AdultsDocument5 pagesAssessing Pain in Verbal Older Adultsronald tadicNo ratings yet
- Pain ManagementDocument14 pagesPain Managementsoumya mNo ratings yet
- Pain Management Plan MCN 314Document3 pagesPain Management Plan MCN 314claudette1882No ratings yet
- Bulandos BSN3-1 Duty Act 4Document7 pagesBulandos BSN3-1 Duty Act 4Rolan BulandosNo ratings yet
- Assessing Pain in Patients: Art ScienceDocument5 pagesAssessing Pain in Patients: Art ScienceShweta SheoranNo ratings yet
- Analysis of Smoking Practices Among College StudentsDocument17 pagesAnalysis of Smoking Practices Among College StudentsJoanne Bernadette AguilarNo ratings yet
- Community Health Nursing NotesDocument4 pagesCommunity Health Nursing NotesJoanne Bernadette AguilarNo ratings yet
- The Problem and The Review of Related LiteratureDocument16 pagesThe Problem and The Review of Related LiteratureJoanne Bernadette AguilarNo ratings yet
- Summary of Findings, Conclusion and Recommendatiojn: The ProblemDocument10 pagesSummary of Findings, Conclusion and Recommendatiojn: The ProblemJoanne Bernadette AguilarNo ratings yet
- Tornado Touches Down in Johnson CountyDocument2 pagesTornado Touches Down in Johnson CountyJoanne Bernadette AguilarNo ratings yet
- Christmas Song Medley 2021Document5 pagesChristmas Song Medley 2021Joanne Bernadette AguilarNo ratings yet
- Smokeless Tobacco Usage, Smoking Location, Cigars and Pipe Use, Peer Behaviors, Alcohol-Related Smoking Behavior, and Stress-Related Smoking BehaviorDocument1 pageSmokeless Tobacco Usage, Smoking Location, Cigars and Pipe Use, Peer Behaviors, Alcohol-Related Smoking Behavior, and Stress-Related Smoking BehaviorJoanne Bernadette AguilarNo ratings yet
- Application LetterDocument1 pageApplication LetterJoanne Bernadette AguilarNo ratings yet
- Chapter 2Document3 pagesChapter 2Joanne Bernadette AguilarNo ratings yet
- QUIZDocument1 pageQUIZJoanne Bernadette AguilarNo ratings yet
- Becoming A Future Good Nurse Leader in Clinical Areas by Making A Better Leadership Roles and Management FunctionsDocument9 pagesBecoming A Future Good Nurse Leader in Clinical Areas by Making A Better Leadership Roles and Management FunctionsJoanne Bernadette AguilarNo ratings yet
- © 2019 Journal of The Practice of Cardiovascular Sciences - Published by Wolters Kluwer - MedknowDocument15 pages© 2019 Journal of The Practice of Cardiovascular Sciences - Published by Wolters Kluwer - MedknowJoanne Bernadette AguilarNo ratings yet
- Quiz 1 3 Johannah Alexis GuiloDocument14 pagesQuiz 1 3 Johannah Alexis GuiloJoanne Bernadette AguilarNo ratings yet
- Intensive Care Unit (ICU)Document6 pagesIntensive Care Unit (ICU)Joanne Bernadette AguilarNo ratings yet
- Philippines: Cancer Mortality ProfileDocument3 pagesPhilippines: Cancer Mortality ProfileJoanne Bernadette AguilarNo ratings yet
- Philo Assignment GuiloDocument1 pagePhilo Assignment GuiloJoanne Bernadette AguilarNo ratings yet
- Review Related LiteratureDocument2 pagesReview Related LiteratureJoanne Bernadette AguilarNo ratings yet
- GUILODocument2 pagesGUILOJoanne Bernadette AguilarNo ratings yet
- Nursing Exam Answers Key LawsDocument2 pagesNursing Exam Answers Key LawsJoanne Bernadette AguilarNo ratings yet
- 5 Laws in The Philippines Affecting The Nursing ProfessionDocument6 pages5 Laws in The Philippines Affecting The Nursing ProfessionaninNo ratings yet
- Name of System Laboratory/ Diagnostic Examination Short Description Normal Result Signifcance of An Abnormal ResultDocument8 pagesName of System Laboratory/ Diagnostic Examination Short Description Normal Result Signifcance of An Abnormal ResultJoanne Bernadette AguilarNo ratings yet
- Cardiac Failures and Myocardial InfarctionDocument41 pagesCardiac Failures and Myocardial InfarctionJoanne Bernadette AguilarNo ratings yet
- Name: Glenda S, Casundo Date: Nov. 3, 2020 Course/Yr: BSN Iv Comp - Appraisal Quiz No.3Document4 pagesName: Glenda S, Casundo Date: Nov. 3, 2020 Course/Yr: BSN Iv Comp - Appraisal Quiz No.3Joanne Bernadette AguilarNo ratings yet
- Name: Glenda S, Casundo Date: Nov. 3, 2020 Course/Yr: BSN Iv Comp - Appraisal Quiz No.1Document4 pagesName: Glenda S, Casundo Date: Nov. 3, 2020 Course/Yr: BSN Iv Comp - Appraisal Quiz No.1Joanne Bernadette AguilarNo ratings yet
- Family Systems TheoryDocument2 pagesFamily Systems TheoryCyrus KayaniNo ratings yet
- HBO Module 1aDocument7 pagesHBO Module 1aPonsica RomeoNo ratings yet
- Foundation To OBDocument16 pagesFoundation To OBDivya SharmaNo ratings yet
- Cooking and Mental HealthDocument4 pagesCooking and Mental Health劉偉慈No ratings yet
- Unit 03 Intro To Business CommunicationDocument14 pagesUnit 03 Intro To Business CommunicationpseNo ratings yet
- Choose More Lose MoreDocument271 pagesChoose More Lose MoreLynseyNo ratings yet
- Smart Students Need Know Principles LearningDocument14 pagesSmart Students Need Know Principles Learning007phantomNo ratings yet
- Analysis of VerbalDocument9 pagesAnalysis of VerbalnindiNo ratings yet
- Define Marketing. Distinguish Product Marketing and Services Marketing With SuitableDocument24 pagesDefine Marketing. Distinguish Product Marketing and Services Marketing With Suitablegkmishra2001 at gmail.com50% (2)
- IALP ProgammaDocument244 pagesIALP ProgammaMarco CicioNo ratings yet
- Qualitative Data Analysis and Interpretation: Systematic Search For MeaningDocument21 pagesQualitative Data Analysis and Interpretation: Systematic Search For MeaningSaad KhanNo ratings yet
- Assessment Brief BMSW5106-KIM - A1 3Document7 pagesAssessment Brief BMSW5106-KIM - A1 3Sagor ChakrabortyNo ratings yet
- SOP Sample 1Document3 pagesSOP Sample 1AnitaNo ratings yet
- Manage Stress with Recreational ActivitiesDocument17 pagesManage Stress with Recreational ActivitiesApryll Anne EdadesNo ratings yet
- Broadcasting Codes of AIR/DDDocument16 pagesBroadcasting Codes of AIR/DDKavita ko100% (3)
- Langer de Ramirez Empowering English Language Learners With Tools From The Web Ch1Document12 pagesLanger de Ramirez Empowering English Language Learners With Tools From The Web Ch1Jorge MendezNo ratings yet
- English Argument Analysis NotesDocument7 pagesEnglish Argument Analysis NotesCharles HuynhNo ratings yet
- Mackay 1973 PDFDocument19 pagesMackay 1973 PDFM. MikeNo ratings yet
- Educ 121-Myvirtualchild Assignment and Rubric 1Document21 pagesEduc 121-Myvirtualchild Assignment and Rubric 1api-316008946No ratings yet
- Observational and Survey ResearchDocument2 pagesObservational and Survey ResearchIop UioNo ratings yet
- Theories of Second Language Acquisition: Input Hypothesis (Krashen)Document15 pagesTheories of Second Language Acquisition: Input Hypothesis (Krashen)Shi Ze100% (1)
- 1 MR Mock Interview Questions and EvaluationDocument3 pages1 MR Mock Interview Questions and Evaluationapi-268290595No ratings yet
- Where Are You Going, Where Have You Been.Document6 pagesWhere Are You Going, Where Have You Been.Nidhi SethiNo ratings yet
- How everyday lives create art through rhythmDocument2 pagesHow everyday lives create art through rhythmMika GrantozaNo ratings yet