You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5808)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (843)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 2023 Grade 8 Mid-Term Test (95 Copies) - ComputersDocument6 pages2023 Grade 8 Mid-Term Test (95 Copies) - ComputersTahpehs PhiriNo ratings yet
- BlacksmithDocument2 pagesBlacksmithTahpehs PhiriNo ratings yet
- Fatsch-MOCK 2022-P1Document10 pagesFatsch-MOCK 2022-P1Tahpehs PhiriNo ratings yet
- 2022 Grade9 SBA #08 - PublisherDocument2 pages2022 Grade9 SBA #08 - PublisherTahpehs PhiriNo ratings yet
- 5 Feasibility ReportDocument37 pages5 Feasibility ReportTahpehs PhiriNo ratings yet
- E WasteDocument2 pagesE WasteTahpehs PhiriNo ratings yet
- 2023 Grade 10 EOT1 Computer StudiesDocument4 pages2023 Grade 10 EOT1 Computer StudiesTahpehs PhiriNo ratings yet
- Final Mongu Conference Presentation 2023 - 123743Document35 pagesFinal Mongu Conference Presentation 2023 - 123743Tahpehs PhiriNo ratings yet
- GCE1Document4 pagesGCE1Tahpehs PhiriNo ratings yet
- Cog 13 LipidsDocument27 pagesCog 13 LipidsTahpehs PhiriNo ratings yet
- Table of Contents PDFDocument3 pagesTable of Contents PDFTahpehs PhiriNo ratings yet
- Social Studies Grade 1 7Document40 pagesSocial Studies Grade 1 7Tahpehs Phiri100% (1)
- Cog 13 - MineralsDocument26 pagesCog 13 - MineralsTahpehs PhiriNo ratings yet
- Ministry of Education, Science, Vocational Training and Early Education Curriculum Development CentreDocument49 pagesMinistry of Education, Science, Vocational Training and Early Education Curriculum Development CentreTahpehs PhiriNo ratings yet
- CLME 1402 IntroductionDocument7 pagesCLME 1402 IntroductionTahpehs PhiriNo ratings yet
- Computer Studies Grade 8-9: Read These Instructions FirstDocument8 pagesComputer Studies Grade 8-9: Read These Instructions FirstTahpehs PhiriNo ratings yet
- Cog 13 - VitaminsDocument36 pagesCog 13 - VitaminsTahpehs PhiriNo ratings yet
- Cog 13 Disorders of Metabolism (Carbohydrates and Protein)Document8 pagesCog 13 Disorders of Metabolism (Carbohydrates and Protein)Tahpehs PhiriNo ratings yet
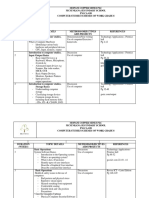
- Computer Studies SchemesDocument5 pagesComputer Studies SchemesTahpehs PhiriNo ratings yet
- Design and Technology G 5 7Document27 pagesDesign and Technology G 5 7Tahpehs PhiriNo ratings yet
- Computer Studies End of Term 3 TestDocument4 pagesComputer Studies End of Term 3 TestTahpehs Phiri100% (1)
- Grade 12 End of Term 2 2020Document12 pagesGrade 12 End of Term 2 2020Tahpehs PhiriNo ratings yet
- G10-12 Computer Studies SchemesDocument12 pagesG10-12 Computer Studies SchemesTahpehs Phiri100% (1)
- Circular Number 4, Term 1, 2021Document4 pagesCircular Number 4, Term 1, 2021Tahpehs PhiriNo ratings yet
- Eya MukwaiDocument1 pageEya MukwaiTahpehs PhiriNo ratings yet
- Kitwe District: Ministry of General EducationDocument11 pagesKitwe District: Ministry of General EducationTahpehs PhiriNo ratings yet
- Test Bank Kaplan and Sadocks Synopsis of Psychiatry 11th EditionDocument35 pagesTest Bank Kaplan and Sadocks Synopsis of Psychiatry 11th Editionspradfroggy.egxp8u100% (34)
- DEFEAT THE DRAGON by DRDocument203 pagesDEFEAT THE DRAGON by DRjose de jesusNo ratings yet
- Add Risk Min MeasDocument12 pagesAdd Risk Min MeasVladimir KostovskiNo ratings yet
- Benefits of Aerobic Exercise and RelatedDocument12 pagesBenefits of Aerobic Exercise and Relatedaleem_80No ratings yet
- Dissertation Topics MD BiochemistryDocument8 pagesDissertation Topics MD BiochemistrySomeoneToWriteMyPaperForMeEvansville100% (1)
- Primary Malignant Bone Tumor Chondrosarcoma of The Sternum I Ketut Suyasa, Gede Ketut Alit Satria Nugraha, I Gede Eka WiratnayaDocument5 pagesPrimary Malignant Bone Tumor Chondrosarcoma of The Sternum I Ketut Suyasa, Gede Ketut Alit Satria Nugraha, I Gede Eka WiratnayaIkram BachtiarNo ratings yet
- Pediatric Hemato OncologyDocument27 pagesPediatric Hemato OncologySilent StalkerNo ratings yet
- Van Der Speeten Et Al. - Current Practice in Delivering HIPEC, EPIC and NIPSDocument10 pagesVan Der Speeten Et Al. - Current Practice in Delivering HIPEC, EPIC and NIPSDiego EskinaziNo ratings yet
- Anatomic Therapy New English PDF Book (2014) PDFDocument262 pagesAnatomic Therapy New English PDF Book (2014) PDFGunalan Pasubathy100% (1)
- Pediatric Bone TumorsDocument20 pagesPediatric Bone TumorsFelipe VenegasNo ratings yet
- Laparoscopic-Assisted Radical Vaginal Hysterectomy (LARVH) : Prospective Evaluation of 200 Patients With Cervical CancerDocument7 pagesLaparoscopic-Assisted Radical Vaginal Hysterectomy (LARVH) : Prospective Evaluation of 200 Patients With Cervical CancerHari NugrohoNo ratings yet
- Retinoblastoma: Carlos Rodriguez-Galindo Matthew W. WilsonDocument162 pagesRetinoblastoma: Carlos Rodriguez-Galindo Matthew W. WilsonJonathan Escobedo EspinozaNo ratings yet
- 1.6 Cell DivisionDocument5 pages1.6 Cell DivisionmariamNo ratings yet
- OF BLADDER CANCER" For M.Ch. Urology, Session 2020-2023Document24 pagesOF BLADDER CANCER" For M.Ch. Urology, Session 2020-2023flammator100% (1)
- What Are Oral Cancers?Document2 pagesWhat Are Oral Cancers?amnaNo ratings yet
- Rycan 2021210036Document7 pagesRycan 2021210036Imagenologia Hospital de ClinicasNo ratings yet
- IndometacinDocument47 pagesIndometacinSava1988No ratings yet
- Disease of Immune System: Sharon Hazel Joyce C. Sebastian, RMTDocument47 pagesDisease of Immune System: Sharon Hazel Joyce C. Sebastian, RMTGilo IlaganNo ratings yet
- Part B: Manual Extract: Patient-Centered Informed Consent in Surgical PracticeDocument10 pagesPart B: Manual Extract: Patient-Centered Informed Consent in Surgical PracticeNaveen Abraham100% (2)
- Deodorant Use and Breast Cancer Risk: To The EditorDocument1 pageDeodorant Use and Breast Cancer Risk: To The EditoragungNo ratings yet
- Berbamine Application Beyond CancerDocument6 pagesBerbamine Application Beyond CancernavneetNo ratings yet
- Daftar Pustaka PDFDocument6 pagesDaftar Pustaka PDFTommy AreanNo ratings yet
- AiluDocument13 pagesAilurashim_bey5853No ratings yet
- Vol 21.2 Neuro-Oncology.2015Document315 pagesVol 21.2 Neuro-Oncology.2015sammy_emerichNo ratings yet
- Singapore-Based Independent Radiotherapy and Oncology Clinic, AARO, Appoints Dr. David Tan Boon Harn As Consultant Radiation OncologistDocument3 pagesSingapore-Based Independent Radiotherapy and Oncology Clinic, AARO, Appoints Dr. David Tan Boon Harn As Consultant Radiation OncologistWeR1 Consultants Pte LtdNo ratings yet
- Syllabus For BPKMCH NEPALDocument7 pagesSyllabus For BPKMCH NEPALDeep SharmaNo ratings yet
- Life Skills 3 and 4-1Document55 pagesLife Skills 3 and 4-1Wakale Nzako100% (1)
- Assay Summary: ADVIA Centaur CPDocument14 pagesAssay Summary: ADVIA Centaur CPGuneyden GuneydenNo ratings yet
- Chemotherapy DrugsDocument43 pagesChemotherapy Drugsbrigette_lagat100% (2)
- Healing Colon Liver & Pancreas Cancer - The Gerson Way - Charlotte Gerson PDFDocument18 pagesHealing Colon Liver & Pancreas Cancer - The Gerson Way - Charlotte Gerson PDFLeonardo Velez De VillaNo ratings yet