You might also like
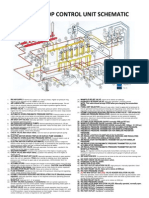
- Koomey Unit-53 Items - A3Document1 pageKoomey Unit-53 Items - A3Jayaprakash Gopala Kamath83% (6)
- It Is Finished - John 19 30Document4 pagesIt Is Finished - John 19 30payasrommelNo ratings yet
- Babylonian Cancer PDFDocument5 pagesBabylonian Cancer PDFCosmin A. TomescuNo ratings yet
- HFOV High-Frequency-Oscillatory-VentilationDocument22 pagesHFOV High-Frequency-Oscillatory-VentilationJZNo ratings yet
- Guidelines of Mechanic Ventilation in Newborn InfantsDocument62 pagesGuidelines of Mechanic Ventilation in Newborn InfantsJairo UrielNo ratings yet
- Pediatric Mechanical VentilationDocument49 pagesPediatric Mechanical VentilationNirubhana ArunthavasothyNo ratings yet
- Setting VentilatorDocument10 pagesSetting VentilatorHafiz YusaryahyaNo ratings yet
- Contoh Kasus-Dr - TunjungDocument22 pagesContoh Kasus-Dr - TunjungYas EliasNo ratings yet
- Mechanical VentilatorsDocument11 pagesMechanical VentilatorsIra Katrina Bernales MendozaNo ratings yet
- Initial Ventilator SettingsDocument22 pagesInitial Ventilator Settingskeperawatan rswnNo ratings yet
- Setting VentilatorDocument19 pagesSetting VentilatorPriscilla BudhipramonoNo ratings yet
- Initial Ventilator SettingsDocument22 pagesInitial Ventilator Settingsandi wija indrawanNo ratings yet
- High Frequency Oscillatory Ventilation (HFOV) تغريدDocument16 pagesHigh Frequency Oscillatory Ventilation (HFOV) تغريدtaghreednurseNo ratings yet
- WeaningDocument55 pagesWeaningKamal Mohamed100% (1)
- Initial Ventilator SettingsDocument5 pagesInitial Ventilator SettingsEloisaNo ratings yet
- ARDSNet VentilatorProtocolDocument3 pagesARDSNet VentilatorProtocolMohammed BadieNo ratings yet
- Managing A Mechanically Ventilated PatientDocument51 pagesManaging A Mechanically Ventilated PatientPeony03No ratings yet
- Adult Respiratory Distress Syndrome: Mazen Kherallah, MD, FCCPDocument51 pagesAdult Respiratory Distress Syndrome: Mazen Kherallah, MD, FCCPArsitoNo ratings yet
- S9600 Non-Invasive Ventilator-BrochureDocument2 pagesS9600 Non-Invasive Ventilator-Brochurevincent kuoNo ratings yet
- PICU Practical Vent GuidelinesDocument6 pagesPICU Practical Vent GuidelinesinaNo ratings yet
- Ventilator Management ProtocolDocument9 pagesVentilator Management ProtocolcrisdinasusenoNo ratings yet
- Spesifikasi Ventilator Draeger Savina 300 Select: Items DescriptionDocument3 pagesSpesifikasi Ventilator Draeger Savina 300 Select: Items DescriptionIZALNo ratings yet
- Weaning From Mechanical VentilationDocument45 pagesWeaning From Mechanical VentilationmartinNo ratings yet
- Mechanical Ventilator: Pressure Control ModeDocument50 pagesMechanical Ventilator: Pressure Control ModesanjibNo ratings yet
- Protocolo LOVDocument6 pagesProtocolo LOVV ANo ratings yet
- ARDS Management Protocol: February 2018Document6 pagesARDS Management Protocol: February 2018soulstakers100% (1)
- Mechanical Ventilation Handout - AllenhoDocument23 pagesMechanical Ventilation Handout - AllenhoTahani SulNo ratings yet
- Mechanical VentilationDocument69 pagesMechanical VentilationCutie PieNo ratings yet
- Fio2 Peep TV RR 12 6 +5 50%: PH Pco Pao HcoDocument1 pageFio2 Peep TV RR 12 6 +5 50%: PH Pco Pao Hcosunil AgarwalNo ratings yet
- NIV and HFNCDocument16 pagesNIV and HFNCMarceline GarciaNo ratings yet
- High Flow Nasal CannulaDocument6 pagesHigh Flow Nasal CannulaLord King LlamasNo ratings yet
- Peds Basic Principles Mechanical VentilationDocument39 pagesPeds Basic Principles Mechanical VentilationNav KovNo ratings yet
- Lockin Specs For Transport VentilatorDocument2 pagesLockin Specs For Transport VentilatorAlauddin SyahNo ratings yet
- Weingart Vent HandoutDocument4 pagesWeingart Vent HandoutStrept Pneumonia100% (1)
- Dräger Evita Infinity® V500 Elite: Advanced and Comprehensive Ventilation TherapyDocument4 pagesDräger Evita Infinity® V500 Elite: Advanced and Comprehensive Ventilation TherapyABHINANDAN SHARMANo ratings yet
- VentilatorDocument112 pagesVentilatorCarolin67% (3)
- APRV VentilationDocument5 pagesAPRV VentilationIrina UngureanuNo ratings yet
- Dräger Savina 300 Classic: Technical DataDocument4 pagesDräger Savina 300 Classic: Technical DataIZAL100% (1)
- Spesifikasi Draeger Evita V300Document3 pagesSpesifikasi Draeger Evita V300yusrimurahNo ratings yet
- Fabian VentilatorDocument17 pagesFabian VentilatorRohana AnaNo ratings yet
- Common Ventilatory SettingsDocument22 pagesCommon Ventilatory SettingsHamza IshtiaqNo ratings yet
- Mechanical Vent MeDocument71 pagesMechanical Vent MeSonaly KoiriNo ratings yet
- Spesifikasi Draeger Evita V300 Standard - FINALDocument3 pagesSpesifikasi Draeger Evita V300 Standard - FINALEny HardiyantiNo ratings yet
- Evita V300 enDocument4 pagesEvita V300 enIgor VinoraNo ratings yet
- Niv HFNCDocument15 pagesNiv HFNCFrank VaronaNo ratings yet
- Basics of Mechanical VentilationDocument38 pagesBasics of Mechanical VentilationbennyrolandnababanNo ratings yet
- Spesifikasi Draeger Evita V300 AdvanceDocument3 pagesSpesifikasi Draeger Evita V300 AdvanceTaufiq RizqullahNo ratings yet
- Weaning From Mechanical VentilationDocument33 pagesWeaning From Mechanical VentilationMuhammad UmairNo ratings yet
- Dräger Savina 300: Technical DataDocument4 pagesDräger Savina 300: Technical DataIfan JayusdianNo ratings yet
- Spesifikasi Ventilator Draeger Savina 300 (CO2) : Items DescriptionDocument2 pagesSpesifikasi Ventilator Draeger Savina 300 (CO2) : Items DescriptionAnonymous 7RJm3Aw5DNo ratings yet
- Pulmonary Function TestsDocument65 pagesPulmonary Function TestsPranathi PrasadNo ratings yet
- Wa0045Document1 pageWa0045Ahmed AlkabodyNo ratings yet
- Philips Respironics V680 VentilatorDocument4 pagesPhilips Respironics V680 VentilatorZuley Hurtado HernandezNo ratings yet
- Management of Acute Respiratory Failure in COVID-PUI Patient - Updated Feb. 2021Document7 pagesManagement of Acute Respiratory Failure in COVID-PUI Patient - Updated Feb. 2021Abhishek GoelNo ratings yet
- 4-6 MV For ARDS (Basic Level)Document49 pages4-6 MV For ARDS (Basic Level)salwafathiNo ratings yet
- Bivent PittsDocument63 pagesBivent PittsFarook BaigNo ratings yet
- Diskusi Teori Ventilator Mekanik - Renasya Nur SarifahDocument19 pagesDiskusi Teori Ventilator Mekanik - Renasya Nur SarifahRenasya Nur syarifahNo ratings yet
- Mechanical Ventilation 16-3Document40 pagesMechanical Ventilation 16-3Ahmed Shawky Mohammedin100% (1)
- Modes of Mechanical VentilationDocument34 pagesModes of Mechanical Ventilationsbraj86100% (1)
- Respiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsFrom EverandRespiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsJian-Xin ZhouNo ratings yet
- Advanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesFrom EverandAdvanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesRating: 4 out of 5 stars4/5 (6)
- Meeting IHPS 2017-10-30Document28 pagesMeeting IHPS 2017-10-30wawa chenNo ratings yet
- Pediatric Department, Pingtung Christian HospitalDocument41 pagesPediatric Department, Pingtung Christian Hospitalwawa chenNo ratings yet
- Alvesco Asthma-101-9-8Document63 pagesAlvesco Asthma-101-9-8wawa chenNo ratings yet
- 2017-06-26 Testis Torsion and Inguinal HerniaDocument20 pages2017-06-26 Testis Torsion and Inguinal Herniawawa chenNo ratings yet
- An Important Advancement in Valved Holding Chamber TechnologyDocument36 pagesAn Important Advancement in Valved Holding Chamber Technologywawa chenNo ratings yet
- Update On Short-Term Controller Usage of Wheezing Disorders in ChildrenDocument33 pagesUpdate On Short-Term Controller Usage of Wheezing Disorders in Childrenwawa chenNo ratings yet
- Reduced Lung Diffusion Capacity After Mycoplasma Pneumoniae PneumoniaDocument5 pagesReduced Lung Diffusion Capacity After Mycoplasma Pneumoniae Pneumoniawawa chenNo ratings yet
- Macrolide Resistant M. Pneumoniae in Children 20130327Document39 pagesMacrolide Resistant M. Pneumoniae in Children 20130327wawa chenNo ratings yet
- Necrotizing Pneumonitis Caused by Mycoplasma Pneumoniae in Pediatric PatientsDocument4 pagesNecrotizing Pneumonitis Caused by Mycoplasma Pneumoniae in Pediatric Patientswawa chenNo ratings yet
- Singular in Infant WheezerDocument31 pagesSingular in Infant Wheezerwawa chenNo ratings yet
- Mycoplasma Pneumoniae and Respiratory Virus Infections in Children With Persistent Cough in EnglandDocument5 pagesMycoplasma Pneumoniae and Respiratory Virus Infections in Children With Persistent Cough in Englandwawa chenNo ratings yet
- Laryngomalacia With Epiglottic Prolapse Obscuring The Laryngeal InletDocument3 pagesLaryngomalacia With Epiglottic Prolapse Obscuring The Laryngeal Inletwawa chenNo ratings yet
- Stridor in Child - Presentation TranscriptDocument18 pagesStridor in Child - Presentation Transcriptwawa chenNo ratings yet
- Bronchitis Obliterans Due To Mycoplasma PneumoniaDocument7 pagesBronchitis Obliterans Due To Mycoplasma Pneumoniawawa chenNo ratings yet
- Clinical Evaluation of Macrolide-Resistant Mycoplasma Pneumoniae-Antimicrob. Agents Chemother.-2006Document5 pagesClinical Evaluation of Macrolide-Resistant Mycoplasma Pneumoniae-Antimicrob. Agents Chemother.-2006wawa chenNo ratings yet
- Community Outbreak of Macrolide-Resistant Mycoplasma Pneumoniae in Yamagata, Japan in 2009Document4 pagesCommunity Outbreak of Macrolide-Resistant Mycoplasma Pneumoniae in Yamagata, Japan in 2009wawa chenNo ratings yet
- Laryngomalacia: Allison M. Dobbie,, David R. WhiteDocument10 pagesLaryngomalacia: Allison M. Dobbie,, David R. Whitewawa chenNo ratings yet
- Meconium aspiration syndrome: Reporter: R3 陳⽴欣 2017-10-31Document33 pagesMeconium aspiration syndrome: Reporter: R3 陳⽴欣 2017-10-31wawa chenNo ratings yet
- Laryngomalaci 2016 Ajoshua Bedwell, MD, GeorgeZalzal, MDNDocument4 pagesLaryngomalaci 2016 Ajoshua Bedwell, MD, GeorgeZalzal, MDNwawa chenNo ratings yet
- Congenital Laryngomalacia Is Related To Exercise-Induced Laryngeal Obstruction in Adolescence - Archdischild-2015.fullDocument7 pagesCongenital Laryngomalacia Is Related To Exercise-Induced Laryngeal Obstruction in Adolescence - Archdischild-2015.fullwawa chenNo ratings yet
- Fortified TeaDocument12 pagesFortified TeaRahul TripathiNo ratings yet
- English Lesson Plan - Week 3Document11 pagesEnglish Lesson Plan - Week 3Chender DadangNo ratings yet
- Relé PDFDocument94 pagesRelé PDFjuanNo ratings yet
- LV36 Ignition SystemsDocument67 pagesLV36 Ignition SystemsĐức HòangNo ratings yet
- Class 6 Social PaperDocument5 pagesClass 6 Social PaperManav RachchhNo ratings yet
- Flashover ReportDocument9 pagesFlashover ReportMahmoud A. SalemNo ratings yet
- 12th Sprint Reloaded-SolutionsDocument47 pages12th Sprint Reloaded-SolutionsMuhammad Anas BilalNo ratings yet
- IMO Shortlist 2010Document72 pagesIMO Shortlist 2010Florina TomaNo ratings yet
- Needs Assessments Processes, Methods and Examples - Annotated Bibliography - Extension - University of Nevada, RenoDocument3 pagesNeeds Assessments Processes, Methods and Examples - Annotated Bibliography - Extension - University of Nevada, RenoSatish UlliNo ratings yet
- Lesson 1Document35 pagesLesson 1Irish GandolaNo ratings yet
- Given Below Are The Features of The Indian Financial SystemDocument3 pagesGiven Below Are The Features of The Indian Financial SystemALLIED AGENCIES0% (1)
- Compiler LabDocument63 pagesCompiler LabAbhishek YadavNo ratings yet
- ASTM D610 - Standard Practice For Evaluating Degree of Rusting On Painted Steel SurfacesDocument6 pagesASTM D610 - Standard Practice For Evaluating Degree of Rusting On Painted Steel SurfacesRoger SchvepperNo ratings yet
- The Times ProjectionDocument5 pagesThe Times ProjectionBelinda NiuNo ratings yet
- Fairview Terminal PhaseII Expansion Project Report - Oct2012Document436 pagesFairview Terminal PhaseII Expansion Project Report - Oct2012NewsroomNo ratings yet
- Ann. Anim. Sci., Vol. 16, No. 2 (2016) 507-519 DOI: 10.1515/aoas-2015-0087Document13 pagesAnn. Anim. Sci., Vol. 16, No. 2 (2016) 507-519 DOI: 10.1515/aoas-2015-0087Cristian José CardozoNo ratings yet
- Group 2I - Herman Miller Case AnalysisDocument7 pagesGroup 2I - Herman Miller Case AnalysisRishabh Kothari100% (1)
- MDA Report Tata Industries FY20 21Document6 pagesMDA Report Tata Industries FY20 21Darshan VadherNo ratings yet
- Review of Status of Advanced Materials (Cost)Document60 pagesReview of Status of Advanced Materials (Cost)enriquesantaolallaNo ratings yet
- Neil Armstrong BiographyDocument4 pagesNeil Armstrong Biographyapi-232002863No ratings yet
- PWD Comfort Room Plan and DetailsDocument1 pagePWD Comfort Room Plan and DetailsRexter UnabiaNo ratings yet
- For Moment of Inertia For PSC GirderDocument6 pagesFor Moment of Inertia For PSC GirderAshutosh GuptaNo ratings yet
- Case Study-Canine ParvoDocument7 pagesCase Study-Canine Parvoapi-437365077No ratings yet
- Mathematics Grade 10 Weeks 1-5 - Term 3Document63 pagesMathematics Grade 10 Weeks 1-5 - Term 3Daniel Dowding100% (1)
- Report Tapioca HarvestingDocument42 pagesReport Tapioca HarvestingAmal NirmalNo ratings yet
- K2042 ManualDocument20 pagesK2042 ManualAthanasios S. ArampatzisNo ratings yet
- Remedial Measures in Astrology by G.S. Kapoor PDFDocument45 pagesRemedial Measures in Astrology by G.S. Kapoor PDFVikas75% (4)